Download presentation
Presentation is loading. Please wait.

1
肾病综合征 附属二院内科

2
诊断标准 ①尿蛋白 >3.5g/d ②血浆白蛋白低于 30g/L ③水肿 ④血脂升高 其中①②为必备条件

3
病因 原发性 ● 微小病变型(儿童) ● 系膜增生性 ● 系膜毛细血管性 ● 局灶节段性硬化 ● 膜性肾病(中老年) 继发性 ● 过敏性紫癜肾炎 ● 乙肝相关性肾炎 ● 狼疮性肾炎 ● 糖尿病肾病 ● 骨髓瘤性肾病 ● 肾淀粉样变性 ● 其它
 ● 系膜增生性 ● 系膜毛细血管性 ● 局灶节段性硬化 ● 膜性肾病(中老年) 继发性 ● 过敏性紫癜肾炎 ● 乙肝相关性肾炎 ● 狼疮性肾炎 ● 糖尿病肾病 ● 骨髓瘤性肾病 ● 肾淀粉样变性 ● 其它")
4
病理生理 大量蛋白尿:肾小球滤过膜分子屏障及 电荷屏障受损,通透性增加 血浆蛋白减低:尿丢失,蛋白摄入不足 水肿:血浆胶体渗透压 ↓ 高脂血症:肝合成增加,外周利用减少

5
(一)微小病变型肾病: LM :肾小球基本正常 IF :阴性 EM :广泛肾小球脏层上皮细胞足突融合 原发性肾病综合征的病理类 型及临床特征
微小病变型肾病: LM :肾小球基本正常 IF :阴性 EM :广泛肾小球脏层上皮细胞足突融合 原发性肾病综合征的病理类 型及临床特征")
6
This is a normal glomerulus by light microscopy. The glomerular capillary loops are thin and delicate. Endothelial and mesangial cells are normal in number. The surrounding tubules are normal. Life is good.

8
(一)微小病变型肾病: LM :肾小球基本正常 IF :阴性 EM :广泛肾小球脏层上 皮细胞足突融合 原发性肾病综合征的病理类型及 临床特征
微小病变型肾病: LM :肾小球基本正常 IF :阴性 EM :广泛肾小球脏层上 皮细胞足突融合 原发性肾病综合征的病理类型及 临床特征")
10
(一)微小病变型肾病 临床表现: 儿童,老年 典型肾综表现 15% 血尿 一般无持续性高血压、肾衰 50% 自发缓解, 90% 激素敏感,易复 发
微小病变型肾病 临床表现: 儿童,老年 典型肾综表现 15% 血尿 一般无持续性高血压、肾衰 50% 自发缓解, 90% 激素敏感,易复 发")
11
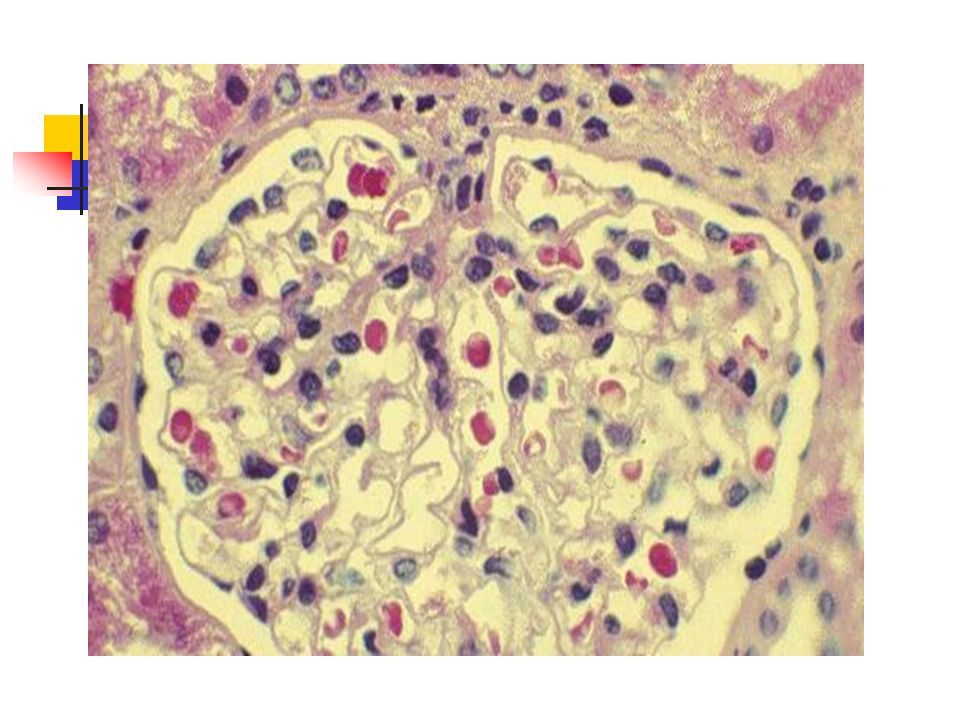
(二)系膜增生性肾小球肾炎 ■ LM :肾小球系膜细胞、系膜基质弥漫增 生 ■ IF : IgA 或 IgM 、 IgG 、 C 3 于系膜区、系 膜区及毛细血管壁颗粒样沉积 ■ EM :系膜区,有时内皮下见到电子致 密物
系膜增生性肾小球肾炎 ■ LM :肾小球系膜细胞、系膜基质弥漫增 生 ■ IF : IgA 或 IgM 、 IgG 、 C 3 于系膜区、系 膜区及毛细血管壁颗粒样沉积 ■ EM :系膜区,有时内皮下见到电子致 密物")
12
This is Berger's disease, or IgA nephropathy. The IgA is deposited mainly in mesangium, which then increases mesangial cellularity as shown at the arrow. Patients with IgA nephropathy usually present with hematuria.

13
(二)系膜增生性肾小球肾炎 ■ LM :肾小球系膜细胞、系膜基质弥漫增生 ■ IF : IgA 或 IgM 、 IgG 、 C 3 于系膜区、系 膜区及毛细血管壁颗粒样沉积 ■ EM :系膜区,有时内皮下见到电子致 密物
系膜增生性肾小球肾炎 ■ LM :肾小球系膜细胞、系膜基质弥漫增生 ■ IF : IgA 或 IgM 、 IgG 、 C 3 于系膜区、系 膜区及毛细血管壁颗粒样沉积 ■ EM :系膜区,有时内皮下见到电子致 密物")
14
This immunofluorescence micrograph demonstrates positivity with antibody to IgA. Note that the pattern is that of mesangial staining. This is IgA nephropathy.

15
( 二)系膜增生性肾小球肾炎 临床表现: 青少年,男性, 50% 前驱感染 IgA:15% 肾综,几乎均有血尿 非 IgA : 30% 肾综, 70% 血尿 逐渐发生高血压、肾衰 激素、细胞毒药物反应不一
系膜增生性肾小球肾炎 临床表现: 青少年,男性, 50% 前驱感染 IgA:15% 肾综,几乎均有血尿 非 IgA : 30% 肾综, 70% 血尿 逐渐发生高血压、肾衰 激素、细胞毒药物反应不一")
16
(三)系膜毛细血管性肾小球肾 炎 病理: LM :系膜细胞及基质弥漫增生,毛细 血管袢呈 “ 双轨征 ” IF : IgG 、 C 3 呈颗粒状系膜区及毛细血 管壁沉积 EM :系膜区、内皮下电子致密物沉积
系膜毛细血管性肾小球肾 炎 病理: LM :系膜细胞及基质弥漫增生,毛细 血管袢呈 双轨征 IF : IgG 、 C 3 呈颗粒状系膜区及毛细血 管壁沉积 EM :系膜区、内皮下电子致密物沉积")
17
This is membranoproliferative glomerulonephritis (MPGN). Those that are idiopathic are divided into types I and II by pathologic findings. As seen here, the glomerulus has increased overall cellularity, mainly mesangial.

18
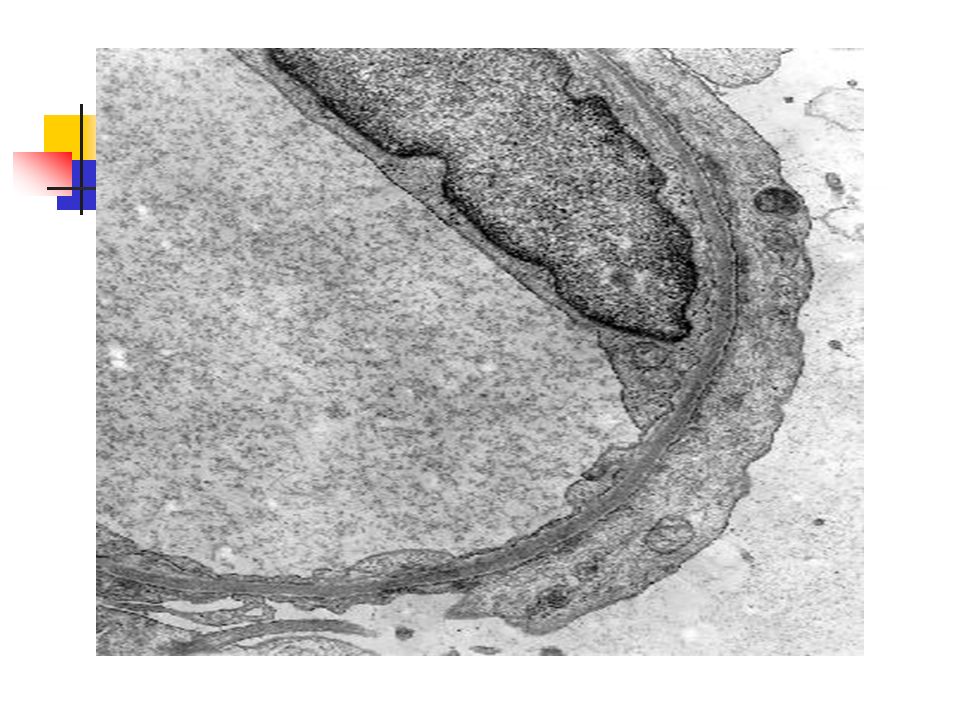
This electron micrograph demonstrates a mesangial cell at the lower left that is interposing its cytoplasm at the arrow into the basement membrane, leading to splitting and reduplication of basement membrane that is piled up above the mesangial cytoplasm in this micrograph. This is MPGN type I. These characteristic EM changes occur when the mesangial cell (which has a macrophage-like function) goes after subendothelial immune deposits, but makes a mess of the basement membrane in the process.
 goes after subendothelial immune deposits, but makes a mess of the basement membrane in the process..")
19
This electron micrograph demonstrates the dense deposits in the basement membrane of MPGN type II. There are dark electron dense deposits within the basement membrane that often coalesce to form a ribbon-like mass of deposits.

21
(三)系膜毛细血管性肾炎 临床表现: 青壮年男性, 70% 前驱感染 60% 肾综, 30% 急性肾炎综合征 肉眼血尿 肾损、高血压出现早, 10 年 50% 肾 衰 激素效果差
系膜毛细血管性肾炎 临床表现: 青壮年男性, 70% 前驱感染 60% 肾综, 30% 急性肾炎综合征 肉眼血尿 肾损、高血压出现早, 10 年 50% 肾 衰 激素效果差")
Similar presentations

 肾球囊 (脏层囊腔,壁层) 近端小管 曲部 (近曲小管) 直部 (降支粗部) 细管 降起细部 升支细部 远端小管 直部(升支粗部) 致密斑 曲部 (远曲小管) 髓拌降支.>")
 过敏性休克 过敏性休克是 I 型变态反应中最严重的一组危急症候群。 发病通常在接触变应原数分钟内出现症状,表现为气急、>")
 ,但病因、发病机制、 病理改变、病程和预后不尽相同,病变主要累 及双肾肾小球的疾病。 肾小球疾病系指一组有相似的临床表现 ( 如 血尿、蛋白尿、高血压等 ) ,但病因、发病机制、>")
. 主要内容 概述 病因 病理生理 病理类型及临床特征 并发症 诊断与鉴别诊断 治疗.>")
血尿 IgA 肾病 内 容内 容.>")
. B 01. 良性腎硬化症( benign nephrosclerosis )係下 列哪一種病況合併的腎臟病變? (A) 糖尿病 (B) 高血壓 (C) 痛風 (D) 敗血症。 ( ’98 專高) C 02. 尿路的惡性上皮性腫瘤多數是: (A)>")

 急性感染后肾小球肾炎是一种常见的肾脏病。 急性起,以血尿、蛋白尿、水肿和高血压为主 要表现,并可有一过性氮质血症。多见于链球 菌感染后 。 急性感染后肾小球肾炎是一种常见的肾脏病。 急性起,以血尿、蛋白尿、水肿和高血压为主.>")

 :变态反应性炎,非特殊 性和特殊性泌尿道炎 二、代谢性疾病 (Metabolic Disease) :糖尿病性肾病 三、血管疾病 (Vascular Disease) 四、中毒性疾病 — 肾小管坏死 (tubular Necrosis)>")


 免疫球蛋白的基本结构 2 抗体的概念 31 免疫球蛋白的生物学特性 33 抗 体( antibody , Ab )>")






