Download presentation
Presentation is loading. Please wait.

1
98 年專科護理師訓練 神經系統常見問題之評估 ( 一 ) 頭痛 Headache 頭暈 Dizziness 成大醫院神經科 黃涵薇醫師
 頭痛 Headache 頭暈 Dizziness 成大醫院神經科 黃涵薇醫師")
2
頭痛 Headache

3
Pain-sensitive cranial structures 顱外 Skin, subcutaneous tissues, muscles extracranial arteries, periosteum of skull Eye, ear nasal cavities perinasal sinuses 顱內 血管 Intracranial venous sinuses and their large tributaries, esp. pericavernous structures Arteries within the dura and pia-subarachnoid, particulary the proximal parts of the ACA, MCA and the intracranial segment of ICA The middle meningeal and superficial temporal arteries 腦膜 Parts of the dura at the base of the brain 顱神經 The optic, oculomotor, trigeminal, glossopharyngeal, vagus, (and the first three cervical nerves)
.")
4
From supratentorial structures Anterior 2/3 of head (V1, V2 dermatones) From infratenotrial structures Vertex, posterior head and neck From VII, IX, X cranial nerves Naso-orbital region, ear, throat Pain from extracrainal part of body NOT refer to head, EXCEPT Cervical portion of ICA Eyebrow, supraorbital region Upper cervical spine occiput Angina pectoris (rare) Jaw, vertex Areas of refer pain from intracranial structures
 From infratenotrial structures Vertex, posterior head and neck From VII, IX, X cranial nerves Naso-orbital region, ear, throat Pain from extracrainal part of body NOT refer to head, EXCEPT Cervical portion of ICA Eyebrow, supraorbital region Upper cervical spine occiput Angina pectoris (rare) Jaw, vertex Areas of refer pain from intracranial structures")
5
「國際頭痛疾病分類」 ICHD (International Classification of Headache Disorders) 第一版在 1988 年公布,第二版於 2004 年刊登於 Cephalalgia 雜誌。 不論是中文版或英文版的「國際頭痛疾病分類」都長 達一百五十頁以上 ! 在英文版第二版中,作者建議-「這份內容龐大的 分類文件不是用來背的,這是一份須要一次又一次 不斷查看的文件。」

6
原發性 (Primary) 次發性 (Secondary) 以決定頭痛的原因及訂定適切的治療計畫 頭痛 Headache
 次發性 (Secondary) 以決定頭痛的原因及訂定適切的治療計畫 頭痛 Headache")
7
原發性頭痛 (primary headache) 意謂頭痛本身即為痛的成因。 超過百分之九十的頭痛患者屬於此類。 重點就是排除次發性的可能。
 意謂頭痛本身即為痛的成因。 超過百分之九十的頭痛患者屬於此類。 重點就是排除次發性的可能。")
8
無預兆偏頭痛 Migraine without aura A. 至少有 5 次能符合基準 B-D 的發作 B. 頭痛發作持續 4-72 小時 ( 未經治療或治療無效 ) C. 頭痛至少具下列二項特徵: 1. 單側 2. 搏動性 3. 疼痛程度中或重度 4. 日常活動會使頭痛加劇或避免此類活動(如走路或爬樓 梯) D. 當頭痛發作時至少有下列一項: 1. 噁心及 / 或嘔吐 2. 畏光及怕吵 E. 非歸因於其他疾患
 C. 頭痛至少具下列二項特徵: 1. 單側 2. 搏動性 3. 疼痛程度中或重度 4. 日常活動會使頭痛加劇或避免此類活動(如走路或爬樓 梯) D. 當頭痛發作時至少有下列一項: 1. 噁心及 / 或嘔吐 2. 畏光及怕吵 E. 非歸因於其他疾患.")
9
典型預兆偏頭痛性頭痛 Typical aura with migraine headache A. 至少有 2 次符合基準 B-D 的發作 B. 預兆至少包括下列一項,但無肢體無力: 1. 完全可逆視覺症狀,包括正向特徵 ( 如:閃爍的光、點或線 ) 及 / 或負向特 徵 ( 即視力喪失 ) 2. 完全可逆感覺症狀,包括正向特徵 ( 即針刺感 ) 及 / 或負向特徵 ( 即麻木感 ) 3. 完全可逆失語性語言障礙 C. 至少具下列 2 項: 1. 單 側的視覺症狀及 / 或單側感覺症狀 2. 至少一種預兆症狀在≧ 5 分鐘逐漸產生,及 / 或不同預兆症狀,在≧ 5 分鐘相 繼發生 3. 每一種症狀持續≧ 5 及≦ 60 分鐘 D. 符合無預兆偏頭痛 基準 B-D 的頭痛,在預兆同時或預兆之後的 60 分鐘內發生 E. 非歸因於其他疾患
 及 / 或負向特 徵 ( 即視力喪失 ) 2. 完全可逆感覺症狀,包括正向特徵 ( 即針刺感 ) 及 / 或負向特徵 ( 即麻木感 ) 3. 完全可逆失語性語言障礙 C. 至少具下列 2 項: 1. 單 側的視覺症狀及 / 或單側感覺症狀 2. 至少一種預兆症狀在≧ 5 分鐘逐漸產生,及 / 或不同預兆症狀,在≧ 5 分鐘相 繼發生 3. 每一種症狀持續≧ 5 及≦ 60 分鐘 D. 符合無預兆偏頭痛 基準 B-D 的頭痛,在預兆同時或預兆之後的 60 分鐘內發生 E. 非歸因於其他疾患.")
10
緊縮型頭痛 Tension-type headache A. Frequent: 至少有十次能符合基準 B-D 之發作,且發作平均每月≧ 1 日但< 15 日,已至少三個月(每年≧ 12 日且< 180 日, 頭痛持續 30 分鐘至 7 日 Chronic: 頭痛平均發作每月≧ 15 日,已> 3 個月(每年≧ 180 日)且符合基 準 B-D, 頭痛持續數小時或可能持續不斷 B. 頭痛至少具下列二項特徵: 1. 雙側 2. 壓迫 / 緊縮性(非搏動性) 3. 程度輕或中度 4. 不因日常活動如走路或爬樓梯而加劇 C. 下列兩項皆符合: 1. 無噁心或嘔吐(可能有食慾不振) 2. 最多只有畏光或怕吵其中一項症狀 D. 非歸因於其他疾患
且符合基 準 B-D, 頭痛持續數小時或可能持續不斷 B. 頭痛至少具下列二項特徵: 1. 雙側 2. 壓迫 / 緊縮性(非搏動性) 3. 程度輕或中度 4. 不因日常活動如走路或爬樓梯而加劇 C. 下列兩項皆符合: 1. 無噁心或嘔吐(可能有食慾不振) 2. 最多只有畏光或怕吵其中一項症狀 D. 非歸因於其他疾患.")
11
叢發性頭痛 Cluster headache A. 至少有 5 次符合基準 B-D 之發作 B. 位於單側眼眶、上眼眶及 / 或顳部重度或極重度疼痛,如不治 療可持續 15 至 180 分鐘 C. 頭痛時至少伴隨下列一項: 1. 同側結膜充血及 / 或流淚 2. 同側鼻腔充血及 / 或流鼻水 3. 同側眼皮水腫 4. 同側前額及臉部出汗 5. 同側瞳孔縮小及 / 或眼皮下垂 6. 不安的感覺或躁動 D. 發作頻率為每二日一次至每日八次 E. 非歸因於其他疾患

12
典型三叉神經痛 Classical trigeminal neuralgia A. 發作性 (paroxysmal) 疼痛發作,持續由不到一秒到兩分鐘,影 響三叉神經一支或一支以上分支的支配區,且符合基準 B 及 C B. 疼痛至少具下列一項特徵: 1. 劇烈、尖銳、表淺或刺戳痛 2. 於誘發區引發或由誘因引發 C. 就個別病人而言,疼痛的發作型態是固定 (stereotyped) 的 D. 沒有神經功能缺損的臨床證據 E. 非歸因於其他疾患
 疼痛發作,持續由不到一秒到兩分鐘,影 響三叉神經一支或一支以上分支的支配區,且符合基準 B 及 C B. 疼痛至少具下列一項特徵: 1. 劇烈、尖銳、表淺或刺戳痛 2. 於誘發區引發或由誘因引發 C. 就個別病人而言,疼痛的發作型態是固定 (stereotyped) 的 D. 沒有神經功能缺損的臨床證據 E. 非歸因於其他疾患.")
13
次發性頭痛 (Secondary headache) 意謂頭痛由其他原因所引起 頭部與頸部外傷 顱部或頸部血管疾患 非血管性顱內疾患 物質或物質戒斷 感染 體內恆定疾患 頭顱, 頸, 眼, 鼻, 耳, 口, 鼻竇, 牙或其他面部或顱部結構疾患 精神疾患 「國際頭痛疾病分類」 ICHD II 需治療引起頭痛之原因。
 意謂頭痛由其他原因所引起 頭部與頸部外傷 顱部或頸部血管疾患 非血管性顱內疾患 物質或物質戒斷 感染 體內恆定疾患 頭顱, 頸, 眼, 鼻, 耳, 口, 鼻竇, 牙或其他面部或顱部結構疾患 精神疾患 「國際頭痛疾病分類」 ICHD II 需治療引起頭痛之原因。")
14
與腦瘤相關的頭痛 The pain has no specific features tend to be deep-seated, usually non-throbbing Lasts a few minutes to an hour or more Occur once or many times during a day Physical activity and changes in position of the head may provoke pain, whereas rest diminishes its frequency If unilateral, the pain is nearly always on the same side of tumor Supratentorial/infratentorial tumor 的頭痛以 interauricular circumference 為分界 Late stage, IICP leads to Unilateral to bioccipital or bifrontal headache, nocturnal awakening, projectile vomiting

15
與中風相關的頭痛 25% stroke with headache around the onset 50% headache onset prior to the neurological deficits pressing or throbbing If unilateral, pain is usually ipsilateral to the side of stroke More in large stroke posterior circulation with a history of primary headache

16
老年人的特殊頭痛 Temporal arteritis (Giant cell arteritis) 肇因於頭部動脈的發炎, 多是外頸動脈的分支 頭皮動脈腫脹壓痛併 ESR 或 CRP 上升 可能伴隨 polymyalgia rheumatica 及 jaw claudication 變異性大, 故凡是 60 歲以上新發的持續性頭痛均需懷疑此診斷, 進行適當的診察 易併發前側缺血性視神經病變 (anterior ischemic optic neuropathy) 導致失明, 由一側失明進展至另一側的時間小於一週 需積極用高劑量類固醇預防治療, 治療三天內顯著緩解頭痛 通常也有腦部缺血及失智的危險 Hypnic headache 鈍痛, 只在睡眠中發生, 使病人醒來 三項中具其二 首次發作在 50 歲以後, 醒來後頭痛持續 15 分鐘以上, 一個月 發生 15 次以上 無自主神經系統症狀, 且噁心, 畏光, 怕吵不超過一項
 肇因於頭部動脈的發炎, 多是外頸動脈的分支 頭皮動脈腫脹壓痛併 ESR 或 CRP 上升 可能伴隨 polymyalgia rheumatica 及 jaw claudication 變異性大, 故凡是 60 歲以上新發的持續性頭痛均需懷疑此診斷, 進行適當的診察 易併發前側缺血性視神經病變 (anterior ischemic optic neuropathy) 導致失明, 由一側失明進展至另一側的時間小於一週 需積極用高劑量類固醇預防治療, 治療三天內顯著緩解頭痛 通常也有腦部缺血及失智的危險 Hypnic headache 鈍痛, 只在睡眠中發生, 使病人醒來 三項中具其二 首次發作在 50 歲以後, 醒來後頭痛持續 15 分鐘以上, 一個月 發生 15 次以上 無自主神經系統症狀, 且噁心, 畏光, 怕吵不超過一項")
17
” 雷擊般頭痛 ” T hunderclap headache Subarachnoid hemorrhage Sentinel leak Acute hypertensive crisis Cervical artery dissection Pituitary hypoplexy Cerebral spasm Primary thunderclap headache Primary cough headache Primary headache associated with sexual activity Cerebral venous thrombosis

18
需懷疑顱內高壓之頭痛 IICP Headache Symptoms 廣泛性脹痛, 平躺更易頭痛 Valsalva maneuver 會更痛 半夜痛醒 (nocturnal awakening) 噴射性嘔吐 (projectile vomiting) IICP Signs 視乳頭水腫 (papilloedema) 盲點擴大 視野缺損 第六對腦神經痲痺 臥姿經腰椎穿刺測量出腦脊髓液壓力增加 ( 在非肥胖者 > 200mm H2O ;在肥胖者> 250mm H2O) Cushing response Hypertension, bradycardia, slow and irregular breathing
 噴射性嘔吐 (projectile vomiting) IICP Signs 視乳頭水腫 (papilloedema) 盲點擴大 視野缺損 第六對腦神經痲痺 臥姿經腰椎穿刺測量出腦脊髓液壓力增加 ( 在非肥胖者 > 200mm H2O ;在肥胖者> 250mm H2O) Cushing response Hypertension, bradycardia, slow and irregular breathing")
19
腦脊髓液低壓之頭痛 Intracranial hypotension A. 整個頭 (diffuse) 及 / 或鈍痛,在坐起或站立後 15 分鐘內惡化,至少具 下列一項,且符合基準 D : 1. 頸部僵硬 2. 耳鳴 3. 聽力障礙 4. 畏光 5. 噁心 B. 至少具下列一項: 1. MRI 有腦脊髓液低壓的證據(如:硬腦膜對比增強) 2. 傳統脊髓攝影、 CT 脊髓攝影、或腦池攝影術證實有腦脊髓液滲漏 3. 在坐姿,腦脊髓液起始壓力< 60mm H2O C. 有 / 無硬腦膜穿刺或導致腦脊髓液瘻管病因等病史 D. 頭痛在硬腦膜外血液貼片後 72 小時內緩解
 2. 傳統脊髓攝影、 CT 脊髓攝影、或腦池攝影術證實有腦脊髓液滲漏 3. 在坐姿,腦脊髓液起始壓力< 60mm H2O C. 有 / 無硬腦膜穿刺或導致腦脊髓液瘻管病因等病史 D. 頭痛在硬腦膜外血液貼片後 72 小時內緩解.")
20
原發性頭痛和次發性頭痛可以並存 !

21
Approach patients with headache

22
Location Quality Tightness, pressure, throbbing, stabbing… Intensity Mode of onset, time-intensity curve, and duration Precipitating, aggravating and relieving factors Associative symptoms Head Ache … 有關頭痛需要獲得的病史

23
評估頭痛的嚴重程度 目測類比量表 (Visual analogue scale,VAS) 區分頭痛為十級,即 1 至 10 分。 「 0 」代表沒有頭痛、「 10 」代表這一輩子最嚴 重的疼痛。 概括而言 1 到 3 分表示「輕度」, 4 到 6 分表「中 度」, 7 到 9 分表「重度」,而 10 分表示「極重 度」。
 區分頭痛為十級,即 1 至 10 分。 「 0 」代表沒有頭痛、「 10 」代表這一輩子最嚴 重的疼痛。 概括而言 1 到 3 分表示「輕度」, 4 到 6 分表「中 度」, 7 到 9 分表「重度」,而 10 分表示「極重 度」。")
24
SNOOP Maria-Carman B. Wilson, MD. Symptoms (症狀)如發燒,倦怠,體重減輕 Neurological (神經學)症狀或徵象 Onset (發生)突然,快速惡化 Older (年紀大的病患)出現新發生或逐漸惡 化之頭痛 Previous (原先)頭痛的頻率、強度、時程、 特色改變
如發燒,倦怠,體重減輕 Neurological (神經學)症狀或徵象 Onset (發生)突然,快速惡化 Older (年紀大的病患)出現新發生或逐漸惡 化之頭痛 Previous (原先)頭痛的頻率、強度、時程、 特色改變.")
25
焦點病史 病人這種頭痛有多久了? 長時間持續多年且未曾改變的頭痛常為原發性頭痛, 如偏頭痛。 新頭痛的發生,特別是超過 50 歲,則是個警訊。 若病人已有多年頭痛,它改變了嗎? 了解原本頭痛的改變,包括頻率、強度、時程等不 同的特徵。

26
何時頭痛發生? 夜間頭痛可能是次發性,導因於某些引起顱內壓上 昇的情形。有些時候,剛睡醒時也會有次發性頭痛。 因為這些相似性,頭痛發生的時間需進一步探討來 決定原發或次發。 睡眠時發生的頭痛可以是原發的。叢發性頭痛及偏 頭痛都可在睡眠時發生或將人痛醒。

27
頭痛是突發或慢慢發生? 對於數秒或數分鐘即痛到最痛者,可能會評估是否 有潛在疾患如腦出血、栓塞、顱內壓上昇等情形。 原發性頭痛,包括不明原因( idiopathic )、刺戳性 (stabbing) 頭痛、咳嗽或用力 (exertion) 引起的、和性 交有關的、叢發性及叢發類 (variant) ,都可以快速發 生。
、刺戳性 (stabbing) 頭痛、咳嗽或用力 (exertion) 引起的、和性 交有關的、叢發性及叢發類 (variant) ,都可以快速發 生。")
28
是否曾注意到下列神經學症狀:意識混亂、意 識不清、麻木、無力、言語視力或平衡因難、 或其他神經學不正常的症狀及徵象? 若在偏頭痛發生前產生這些症狀,病人可能符合預 兆偏頭痛。然而,必須區分不符合典型預兆偏頭痛 的症狀及徵象,因此會仔細的詢問相關病史看看是 否這些症狀指向其他問題。

29
若病人曾經歷過預兆,它是如何發生又持續多 久? 偏頭痛預兆通常在數分鐘內逐漸產生,約在 15 至 20 分鐘達到頂峰後,約 25 分鐘消失。 依定義,偏頭痛預兆小於一小時。若預兆超過一小 時,需小心是否為 migraineous infarct 。 是否曾經歷發燒、倦怠、體重減輕或全身不適? 這些症狀可能和潛在的感染、發炎或惡性腫瘤有關, 可能有進一步檢查的必要

30
焦點身體檢查 Physical examination T/P/R and BP Head and neck Local heat/swelling/erythema Local tenderness / knocking pain Eyes injection/ bruit Neck bruit Neck stiffness

31
Neurological examination Consciousness level / content Cranial nerves Pupil size, light reflex, (eye fundus) EOM limitation Facial palsy, gag reflex, tongue deviation Motor system Muscle power DTR Sensory system Pinprick, light touch Coordination system F-N-F / H-K-S test Gait
 EOM limitation Facial palsy, gag reflex, tongue deviation Motor system Muscle power DTR Sensory system Pinprick, light touch Coordination system F-N-F / H-K-S test Gait")
32
III, IV, VI 眼動神經 眼皮下垂 ptosis partial / complete 眼動是否對稱, 有無雙影 X 00 0 00 0 X 00 0 00 0 0 正常 ~ -4 不動

33
肌力 Muscle Power 5 分 : 正常 4 分 : 抗阻力 3 分 : 抗重力 2 分 : 平移 1 分 : 肌肉收縮 0 分 : 不動 5 5 5 5 5 5 5 5 5 5 5 5

34
肌腱反射 DTR (deep tendon reflex) Hypo 0~1 Low motor neuron lesion Normal 2 Hyper 3~clonus Upper motor neuron lesion ++ ↓↑
 Hypo 0~1 Low motor neuron lesion Normal 2 Hyper 3~clonus Upper motor neuron lesion ++ ↓↑")
35
實驗室與診斷檢查 血液檢查 影像學檢查 CT or MRI ? CTA/MRA or conventional angiography ? 腦脊髓液檢查 Open / close pressure CSF appearance WBC, RBC, total protein, lactic acid, glucose Culture / antigen identification / PCR

37
Headache Hygiene Tips (1) Get Regular Sleep Go to bed and wake up at regular times each day Do not sleep excessively on the weekends and too little on the weekdays Most adults need approximately 6-8 hours of sleep per night Eat Regular Meals Low blood sugar can trigger a headache Eat regular meals three times each day including protein, fruits, vegetables and carbohydrates Too much sugar may lead to a rapid increase in blood sugar followed by a rapid decline in blood sugar, which can trigger a headache Get Moderate Amounts of Routine Exercise Moderate exercise three to five times each week will help reduce stress and keep you physically fit Too much exercise or inconsistent patterns of exercise may trigger headache
 Get Regular Sleep Go to bed and wake up at regular times each day Do not sleep excessively on the weekends and too little on the weekdays Most adults need approximately 6-8 hours of sleep per night Eat Regular Meals Low blood sugar can trigger a headache Eat regular meals three times each day including protein, fruits, vegetables and carbohydrates Too much sugar may lead to a rapid increase in blood sugar followed by a rapid decline in blood sugar, which can trigger a headache Get Moderate Amounts of Routine Exercise Moderate exercise three to five times each week will help reduce stress and keep you physically fit Too much exercise or inconsistent patterns of exercise may trigger headache")
38
Headache Hygiene Tips (2) Drink Plenty of Water A normal adult should drink plenty of water throughout the day Dehydration may cause headaches Limit Caffeine, Alcohol and other Drugs Caffeine is a stimulant and caffeine withdrawal may cause headaches when blood levels of caffeine taper Alcohol may be a trigger for headaches and alcohol in moderation may reduce the number of headaches Reduce Stress Stress may lead to an increase in headache Relaxation and stress management may help reduce headaches
 Drink Plenty of Water A normal adult should drink plenty of water throughout the day Dehydration may cause headaches Limit Caffeine, Alcohol and other Drugs Caffeine is a stimulant and caffeine withdrawal may cause headaches when blood levels of caffeine taper Alcohol may be a trigger for headaches and alcohol in moderation may reduce the number of headaches Reduce Stress Stress may lead to an increase in headache Relaxation and stress management may help reduce headaches")
39
Headache - Cases discussion

40
CASE 1 28 歲女性 主訴 : 頭痛三個月 現在病史: 似乎三個月前就開始會頭痛,然後發現次數愈來愈頻繁,也愈痛, 尤其最近這兩週較嚴重,甚至胃口不好,吃不下飯。 頭痛的部位是整個頭,緊緊脹脹的痛、好像是整圈緊紮的痛,早 上睡醒或者好好去睡一覺後,會覺得好一點,經常是越到下午越 容易頭痛。但是不曾有半夜痛醒來的經驗。 頭痛起來時,並沒有眼前出現閃光,眼睛周圍沒有痛,不會怕光, 沒有伴隨嘔吐或噁心,最近視力正常,記憶力也還好。 最近沒有感冒、發燒、鼻塞、濃鼻涕,也沒有過敏性鼻炎、鼻竇 炎。耳朵也不會痛。手腳活動正常,不會常跌倒 最近半年換新工作,因工作還未完全熟悉,且業務量大,常常加 班,自覺很辛苦 。 身體檢查: 血壓 136/88 mmHg 心跳 96/min 意識清醒、記憶正常,神經學檢查一切正常

41
CASE 2 25 year-old female, no underlying disease Subacute progressive headache for 2 months Diffuse, swelling sensation Cough and defecation worse the headache Midnight headache, awaking her from sleep nausea/vomiting while headache Blurred vision (+) Body weight loss (+) Fever (-)
 Body weight loss (+) Fever (-)")
42
Summary of N.E. & lab Conscious clear Neck supple NE all normal, except papilloedema (OU) CSF open pressure 310 mmH2O, no cell
 CSF open pressure 310 mmH2O, no cell.")
43
Lupus leukoencephalopathy with IICP

44
頭暈 Dizziness

45
病人主訴 Dizziness ” 頭暈 ” 的意思是 …. ? Vertigo 眩暈 an illusion of motion “spinning sensation”, ”whirling”, ”tilting” likely to indicate an abnormality of the semicircular canals or the central nervous system structures that process signals from the semicircular canals Nonspecific “dizziness” “giddy” or “lightheaded” Disequilibrium Presyncope

46
40% have peripheral vestibular dysfunction 25% have other problems, such as presyncope and disequilibrium 15% have a psychiatric disorder 10% have a central brainstem vestibular lesion 10 % remains uncertain in approximately 當病人主訴 ” 頭暈 ”….

47
區分 vertigo 和 dizziness (1) Time course Vertigo is never continuous Even when the vestibular lesion is permanent, the central nervous system adapts to the defect so that vertigo subsides over several weeks Provoking factors Some are precipitated by maneuvers that change head position or middle ear pressure maneuvers that change head position without lowering blood pressure or decreasing cerebral blood flow is diagnostic Aggravating factors All vertigo is made worse by moving the head. If head motion does not worsen the feeling, it is probably another type of dizziness.

48
Associated signs and symptoms Nystagmus is not always readily visible, although it often can be elicited by provocative maneuvers or with electronystagmography. Postural instability it is common for patients with vertigo to have difficulty maintaining steady upright posture when walking, standing, and even sitting unsupported, particularly when the symptoms are acute. Hearing loss very suggestive of a peripheral cause of vertigo, although their absence does not exclude the diagnosis Brainstem signs The presence of additional neurologic signs strongly suggests the presence of a central vestibular lesion. 區分 vertigo 和 dizziness (2)
.")
50
Peripheral vertigo

51
Benign paroxysmal positional vertigo The most common form of positional vertigo, accounting for nearly 1/2 of patients with peripheral vestibular dysfunction Most commonly attributed to calcium debris within the posterior semicircular canal, known as canalithiasis posterior canal BPPV more often than the anterior (superior) and horizontal semicircular canals Symptoms recurrent episodes of vertigo lasting one minute or less provoked by specific types of head movements typically recur periodically for weeks to months without therapy may be associated with nausea and vomiting have no other neurologic complaints
 and horizontal semicircular canals Symptoms recurrent episodes of vertigo lasting one minute or less provoked by specific types of head movements typically recur periodically for weeks to months without therapy may be associated with nausea and vomiting have no other neurologic complaints")
52
Dix-Hallpike maneuver With the patient sitting, the neck is extended and turned to one side. The p’t is then placed supine rapidly, so that the head hangs over the edge of the bed. The patient is kept in this position and observed for nystagmus for 30 seconds. Nystagmus usually appears with a latency of a few seconds and lasts less than 30 seconds. It has a typical trajectory, beating upward and torsionally, with the upper poles of the eyes beating toward the ground. After it stops and the patient sits up, the nystagmus will recur but in the opposite direction. Therefore, the patient is returned to upright and again observed for nystagmus for 30 seconds. If nystagmus is not provoked, the maneuver is repeated with the head turned to the other side. If nystagmus is provoked, the patient should have the maneuver repeated to the same (provoked) side; with each repetition, the intensity and duration of nystagmus will diminish.
 side; with each repetition, the intensity and duration of nystagmus will diminish..")
53
Vestibular neuritis Viral or postviral inflammatory disorder affecting the vestibular portion of the eighth cranial nerve Symptoms Sapid onset of severe vertigo nausea, vomiting gait instability. preserved ability to ambulate. toward the affected side have no other neurologic complaints Signs Spontaneous vestibular nystagmus unilateral, horizontal, or horizontal-torsional suppressed with visual fixation does not change direction with gaze fast phase of nystagmus beats away from the affected side.

54
Meniere's disease Arise from abnormal fluid and ion homeostasis in the inner ear endolymphatic hydrops with distortion and distention of the membranous, endolymph-containing portions of the labyrinthine system Syndrome episodic vertigo associated with nausea and vomiting, and persists from 20 minutes to 24 hours duration Sensorineural hearing loss often initially affects the lower frequencies. progresses over time, and often results in permanent hearing loss at all frequencies in the affected ear over an 8 to 10 year period typically associated with intense aural fullness or pressure in the ear or the side of the head Tinnitus characteristically low pitch may be associated with auditory distortion

55
Central vertigo

56
Lateral medullary infarction Wallenberg syndrome Ipsilateral Horner's syndrome Dissociated sensory loss (loss of pain and temperature sensation on the ipsilateral face and contralateral limbs and trunk) Abnormal eye movements Ipsilateral loss of corneal reflex Hoarseness and dysphagia Ipsilateral limb ataxia
 Abnormal eye movements Ipsilateral loss of corneal reflex Hoarseness and dysphagia Ipsilateral limb ataxia")
57
Cerebellar stroke Vertigo, may with nausea/vomiting Limb dysmetria, dysarthria, or headache Usually unable to stand or walk unsupported The direction of falling is not necessarily opposite to the direction of the nystagmus Nystagmus other than horizontal or horizontal-torsional, may change direction with gaze not suppressed with visual fixation Patients with a vascular event are typically older and/or have atherosclerosis risk factors (hypertension, diabetes, smoking).
.")
58
Vestibular schwannoma ( acoustic neuroma) Symptoms can be due to cranial nerve involvement, cerebellar compression, or tumor progression. Cochlear nerve (95%) The two major symptoms were hearing loss usually chronic Tinnitus was present in 63 percent. Vestibular nerve (61%) Unsteadiness while walking, which was typically mild to moderate in nature and frequently fluctuated in severity True spinning vertigo was uncommon. The most nondescript vertiginous sensations Trigeminal nerve (17%) facial numbness (paresthesia), hypesthesia, and pain. Facial nerve (6%) facial paresis and, less often, taste disturbances. Tumor progression press on the cerebellum or brainstem and result in ataxia. lower cranial nerves (nerves IX, X, and XI, leading to dysarthria, dysphagia, aspiration, and hoarseness Brainstem compression, cerebellar tonsil herniation, hydrocephalus and death can occur in untreated cases.
 The two major symptoms were hearing loss usually chronic Tinnitus was present in 63 percent. Vestibular nerve (61%) Unsteadiness while walking, which was typically mild to moderate in nature and frequently fluctuated in severity True spinning vertigo was uncommon. The most nondescript vertiginous sensations Trigeminal nerve (17%) facial numbness (paresthesia), hypesthesia, and pain. Facial nerve (6%) facial paresis and, less often, taste disturbances. Tumor progression press on the cerebellum or brainstem and result in ataxia. lower cranial nerves (nerves IX, X, and XI, leading to dysarthria, dysphagia, aspiration, and hoarseness Brainstem compression, cerebellar tonsil herniation, hydrocephalus and death can occur in untreated cases..")
59
Peripheral vs. Central vertigo Nystagmus Latency 2-20 seconds Usually < 1min Fatiguability (+) Unidirectional, fast phase toward the normal ear; never reverses direction Horizontal with a torsional component, never purely torsional or vertical visual fixation Suppressed Unidirectional instability, walking preserved Deafness or tinnitus may be present Nystagmus No latency Usually > 1min No fatiguability Sometimes reverses direction when patient looks in the direction of slow phase Can be any direction visual fixation NOT Suppressed Severe instability, patient often falls when walking Other neurologic signs often present Usually less severe vertigo
 Unidirectional, fast phase toward the normal ear; never reverses direction Horizontal with a torsional component, never purely torsional or vertical visual fixation Suppressed Unidirectional instability, walking preserved Deafness or tinnitus may be present Nystagmus No latency Usually > 1min No fatiguability Sometimes reverses direction when patient looks in the direction of slow phase Can be any direction visual fixation NOT Suppressed Severe instability, patient often falls when walking Other neurologic signs often present Usually less severe vertigo.")
60
Other “dizziness”

61
Presyncope The prodromal symptom of fainting or a near faint. Symptoms Lasts for seconds to minutes and is often recognized by the patient as "nearly blacking out", "nearly fainting.", lightheadedness, a feeling of warmth, diaphoresis, nausea, and visual blurring occasionally proceeding to blindness usually occurs when the patient is standing or seated upright and not when supine Signs An observation of pallor by onlookers A history of cardiac disease, including cardiac dysrhythmias (tachycardias or bradyarrhythmias), coronary heart disease, congestive heart failure, is relevant The etiology Orthostatic hypotension, cardiac arrhythmias, and vasovagal attacks..
, coronary heart disease, congestive heart failure, is relevant The etiology Orthostatic hypotension, cardiac arrhythmias, and vasovagal attacks...")
62
Disequilibrium A sense of imbalance that occurs primarily when walking Etiology peripheral neuropathy a musculoskeletal disorder interfering with gait vestibular disorder cervical spondylosis Parkinsonism visual impairment.

63
Nonspecific dizziness 精神科疾病 Often builds up gradually, waxes and wanes over a period of 20 minutes or longer, and gradually resolves 1/4 major depression 1/4 generalized anxiety or panic disorder 1/2 somatization disorder, alcohol dependence, and/or personality disorder in one series Commonly related to hyperventilation; may be no sensation of "air hunger" since these patients are hyperventilating only to a slight degree 頭部外傷、貧血、慢性阻塞性肺病、 睡眠不足、營養不良、血糖過低 過高、電解質不平衡、長期在密閉的空間工作,疲倦加上工作場所的 不良氣體(二氧化碳、油漆、塗料、麥克筆、修正液、印表機的碳粉 油墨 … ) 藥物 ( 例 降血壓藥、鎮定劑、酒精、帕金森氏症藥物、精神用藥、抗 生素.. )
.")
64
Approach patients with dizziness

65
焦點病史 Dizziness? Vertigo? Onset (posture), duration, course, aggravating factor, relieving factor Associated Symptoms Vomiting? Headache? Visual loss (black- or white-out)? Hearing loss? Palpitations? Chest discomfort? Dyspnea? Staggering or ataxic gait? Double vision? Slurred speech? Numbness / weakness of the face or body? Clumsiness, or incoordination? Medications / Substance
, duration, course, aggravating factor, relieving factor Associated Symptoms Vomiting. Headache. Visual loss (black- or white-out). Hearing loss. Palpitations. Chest discomfort. Dyspnea. Staggering or ataxic gait. Double vision. Slurred speech. Numbness / weakness of the face or body. Clumsiness, or incoordination. Medications / Substance.")
66
焦點身體檢查 Physical examination Pulse rate and BP Head and neck Eyes: conjunctiva pale or not, visual acuity Ear: tenderness / discharge Neck: pain / ROM limitation Extremities Joints pain / deformity

67
Neurological examination Consciousness level / content Cranial nerves EOM limitation Facial sensation, corneal reflex Nystagmus, hearing Facial palsy, gag reflex, tongue deviation Motor system Muscle power DTR Sensory system Pinprick, light touch Coordination system F-N-F / H-K-S test Gait

68
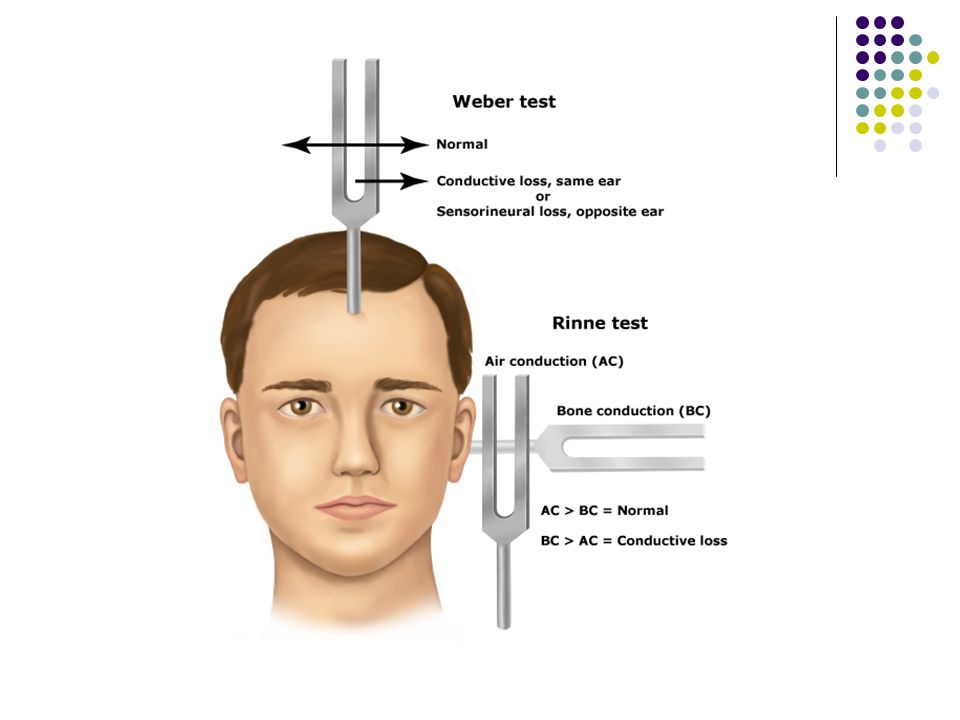
VIII 聽平衡神經 聽力 Rinne test: AC>BC Weber test: 中央或偏向 眼振 0 0 0 00 ← ← ← 線條越粗代表 幅度越大 箭頭越多代表 速度越快 小腦, 腦幹或平衡神經問題皆有可能出現眼振 區分中耳問題 或聽神經問題

70
血液檢查 Caloric test The head of the patient should be tilted at 30º When warm water at 44ºC is infused into an ear, the normal response is nystagmus with the fast component toward the infused ear. When cold water at 30ºC is infused; the normal response is nystagmus with the fast component away from the cold water- infused ear. Audiometry 聽力檢查 Brainstem auditory evoked potentials 腦幹聽覺誘發電位 Electronystagmography 眼振圖檢查 影像學檢查 對於後顱窩的病灶 MRI 優於 CT 實驗室與診斷檢查

71
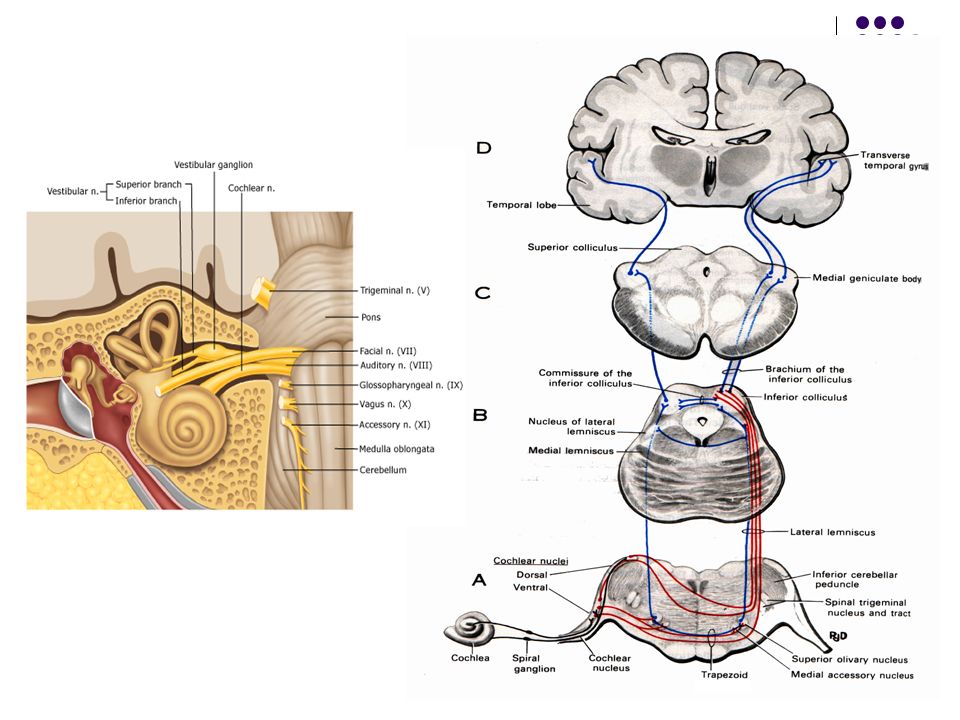
Short-latency components of BAEP

72
Dizziness- Cases discussion

73
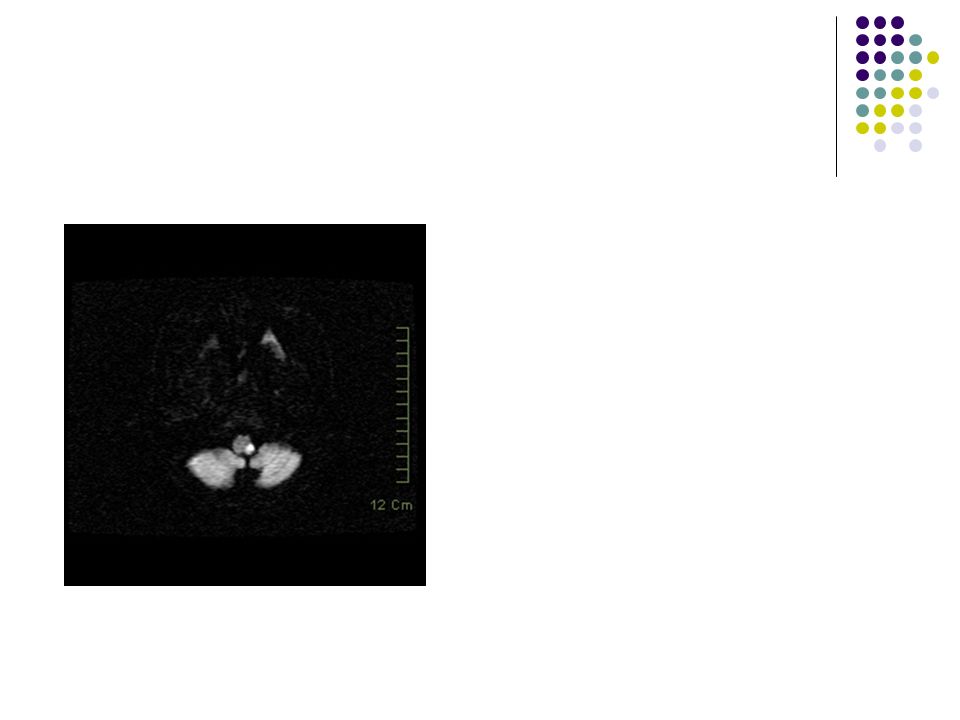
CASE 1 65 y/o male, DM and H/T poor control Acute vertigo and unsteadiness since yesterday morning (noted while getting up) Tend to deviate to right side while walking Can’t use chopstickes well while eating Right occipital dull headache (+), nausea(+) No vomiting, no tinnitus No limbs weakness or numbness, no sphincter problem No ottohrea, ear pain, drug usage or significant infection episode LMD Mx ineffective, thus visit our ER
 Tend to deviate to right side while walking Can’t use chopstickes well while eating Right occipital dull headache (+), nausea(+) No vomiting, no tinnitus No limbs weakness or numbness, no sphincter problem No ottohrea, ear pain, drug usage or significant infection episode LMD Mx ineffective, thus visit our ER")
74
Summary of N.E. Hearing normal Gaze-evoked nystagmus, fast phase to left side Normal muscle power and sensation Right limbs dysmetria and dysdiadochokinesia Tends deviate to right side while standing and walking

75
Right cerebellar hemisphere infarct

76
CASE 2 20 y/o female, no significant past history Progressive R’t hearing impairment since about 4 years ago Intermittent vertigo, R’t tinnitus associated with unsteadiness while changing position in recent 1 year, with increasing frequency Mouth angle deviate to L’t, mild slurred speech and occasional choking in recent 1 month Denied facial numbness and double vision No limbs weakness or numbness, no sphincter problem No ottohrea, ear pain, drug usage or significant infection episode

77
Summary of N.E. Cranial nerves involvement R’t Facial (VII) nerve palsy R’t Vestibulocochlear (VIII) nerve Suspicious CrN IX, X involvement (according to history) No obvious pyramidal system involvement
 nerve palsy R’t Vestibulocochlear (VIII) nerve Suspicious CrN IX, X involvement (according to history) No obvious pyramidal system involvement .")
78
Huge right acoustic neuroma with brainstem and cerebellar compression

79
Thanks For Your Attention ~

80
需要立刻求醫的頭痛警訊 任何突發性嚴重的頭痛。 頭痛伴隨抽筋的現象。 頭痛伴隨有發燒的現象。 頭痛伴隨神智不清。 頭痛伴隨昏迷。 頭部外傷以後的疼痛。 以前不頭痛,現在突然發生的頭痛。 以前有頭痛,但現在的型態改變。 咳嗽、用力或彎腰的時候,其頭痛增加。 頭痛導致半夜醒來。 頭痛伴隨著眼睛或耳朵的疼痛。 頭痛伴隨著頸部僵硬。

Similar presentations








 河南中医学院第一附属医院 杜正光>")




>")


>")
>")

