Download presentation
Presentation is loading. Please wait.

1
藥物與慢性腎臟病 之相關性 國立台灣大學醫學院附設醫院雲林分院 腎臟科主治醫師 李玟儀 醫師

2
盛行個案數 52,537 血液透析 48,072 腹膜透析 4,465 盛行率 2,288 每百萬人口 發生率 416 每百萬人口 TSN Renal Registry 1990 ~ 2007 腹膜透析 8.5 % 血液透析 91.5 % 2007 年度台灣地區透析狀況

3
透析治療現況 腎臟相關疾病致死率,多年來一直在全國十大死 因排行榜上 ( 第十名 ) 洗腎高居重大傷病花費的第一位 平均洗腎每人每年花費六十多萬 洗腎盛行率高居世界第二 洗腎發生率高居世界第一
 洗腎高居重大傷病花費的第一位 平均洗腎每人每年花費六十多萬 洗腎盛行率高居世界第二 洗腎發生率高居世界第一")
4
原因 人口老化 濫服西藥(止痛劑,消炎藥) 濫服中藥(馬兜鈴酸) 透析照護品質良好(洗腎一年死亡率:台 灣, 15 %;美加, 25 %;日本, 9 %)
 濫服中藥(馬兜鈴酸) 透析照護品質良好(洗腎一年死亡率:台 灣, 15 %;美加, 25 %;日本, 9 %)")
5
非類固醇抗發炎藥物 Non- steroid anti-inflammatory drug (NSAID)
")
6
PGI2, PGE2 PGI2, PGE2, TXA2 PGE2, PGF2a Maintain GFR, Vasoconstriction(TXA2) Enhance NaCl and water excretion. Influence regional blood flow (vasa recta)
.")
7
PGE2, PGI2 PGI2, PGE2 Vasodilation (PGI2/E2,direct) Vasoconstriction (PGE2,indirect) Stimulates renin release
 Vasoconstriction (PGE2,indirect) Stimulates renin release")
8
Compartmentalization of PG -- act as autocoids SiteEicosanoidAction ArteriolesPGI 2, PGE 2 PGE 2 Vasodilation (direct) Vasoconstriction (indirect) GlomeruliPGI 2 >PGE 2 TXA 2 Maintain GFR Vasoconstriction Tubules (most collecting duct) PGE 2, PGF 2α Enhance NaCl and water excretion Influence regional blood flow (vasa recta) Interstitial cells PGE 2 JG apparatusPGE 2, PGI 2 Stimulates renin release
 Vasoconstriction (indirect) GlomeruliPGI 2 >PGE 2 TXA 2 Maintain GFR Vasoconstriction Tubules (most collecting duct) PGE 2, PGF 2α Enhance NaCl and water excretion Influence regional blood flow (vasa recta) Interstitial cells PGE 2 JG apparatusPGE 2, PGI 2 Stimulates renin release")
9
使用 NSAID 造成的腎臟問題 1.Vasomotor acute renal failure 血管舒縮性急性 腎衰竭 2.Nephrotic syndrome with tubulointerstitial nephritis 腎病症候群與腎小管間質性腎炎 3.Chronic renal failure 慢性腎衰竭 4.Salt retention 鹽分滯留 5.Hyponatremia 低血鈉症 6.Hyperkalemia 高血鉀症

10
NSAID 引發之血管舒縮性急性腎衰竭 臨床表現 Oligouria Usually occurs with a few days of beginning medicine Hyperkalemia out of proportion to renal failure Low FeNa, unlike other oligouric ARF. Urinalysis is unremarkable. Usually does not require dialysis Usually reversible with discontinuation of NSAID. Oxford textbook: acute tubular necrosis

11
NSAID 引發之血管舒縮性急性腎衰竭 危險因子 urinary passage of metabolites of PG is elevated in these conditions Decreased effective arterial blood flow Normal or increased effective arterial blood flow Congestive heart failure Cirrhosis (esp. ascites/low UNa) Nephrotic syndrome Sepsis Hemorrhage Diuretic therapy Postoperative patients with 3 rd space fluid Volume depletion/hypotension Chronic renal failure Glomerulonephritis Elderly Contrast-induced nephropathy Obstructive uropathy Cyclosporine use (in these conditions, the vasodilatory effect of PG is important for maintain GFR)
 Nephrotic syndrome Sepsis Hemorrhage Diuretic therapy Postoperative patients with 3 rd space fluid Volume depletion/hypotension Chronic renal failure Glomerulonephritis Elderly Contrast-induced nephropathy Obstructive uropathy Cyclosporine use (in these conditions, the vasodilatory effect of PG is important for maintain GFR).")
12
Isoforms of COX COX-1: constitutively expressed in most tiuuse, involved in normal homeostasis. Gastric cytoprotection. COX-2: inducible under stimuli (GF, cytokine) in inflammation. Specific COX-2 inhibitors can reduce GI complications. Current evidences revealed that, both in human and animal studies, COX-2 is constitutively existed and is important to maintain GFR in normal conditions. Mostly expressed in endothelial and smooth muscle cells of arteries, arterioles, veins, and visceral epithelial cells.
 in inflammation. Specific COX-2 inhibitors can reduce GI complications. Current evidences revealed that, both in human and animal studies, COX-2 is constitutively existed and is important to maintain GFR in normal conditions. Mostly expressed in endothelial and smooth muscle cells of arteries, arterioles, veins, and visceral epithelial cells..")
13
對腎臟而言, 是否所有 NSAID 都一樣 ? Celecoxib reduce the urinary excretion of prostacyclin metabolite to a comparable degree as with indomethacin. In older patients with GFR 30-80, rofecoxib and indomethacin both reduced GFR to a similar extent. Celecoxib and rofecoxib has similar risk of renal toxicity, compaired with traditional NSAIDs in high risk persons. (FDA) Specific COX-2 inhibitor may not offer any distinct advantage over traditional NSAIDs with regard to renal toxicity.
 Specific COX-2 inhibitor may not offer any distinct advantage over traditional NSAIDs with regard to renal toxicity..")
14
NSAID 引發慢性腎衰竭 Chronic renal failure Anagesic nephropathy: aspirin+phenacetin+ caffeine Long-term use NSAID alone can lead to CRF. NSAID related CRF: tubulomedullary dysfunction: impaired concentrating ability, acidification defect, salt-losing state. Slowly progressive, nonspecific symptoms. Mixture of glomerular and tubular proteinuria. Common sterile pyuria, occasionally hematuria.

15
NSAID 引發慢性腎衰竭 Suggestion of chronic analgesic use Suggestion by National Kidney Fundation (NKF): Ingestion of aspirin and NSAID was not encouraged. (increased risk when combine use) Habitual consumption of analgesics is discouraged. Monitoring is recommended if used. Combination analgesics is recommended to be available by prescription only with an explicit warning to physicians that habitual consumption of the combination products could lead to the insidious development of CRF.
 Habitual consumption of analgesics is discouraged. Monitoring is recommended if used. Combination analgesics is recommended to be available by prescription only with an explicit warning to physicians that habitual consumption of the combination products could lead to the insidious development of CRF..")
16
NSAID 引發慢性腎衰竭 Suggestion of chronic analgesic use 4. There should be an explicit warning to consumer regarding NSAID use. 5. There is negligible evidence of habitual use of acetaminophen alone leading to CRF, and no evidence of that occasional use of acetaminophen cause renal failure. 6. There is no risk of regular use of aspirin in the doses recommended for preventing CV event.

17
中草藥腎病變

18
中藥的迷思 中藥藥性溫和, 又可以固本強身 ?? 未經科學驗證的治療或強身固本之道, 都不 應採信 藥性溫和 = 可能沒效 ?? 有一些中藥應該是有效的, 但在沒有科學驗 證之前, 我們沒有辦法知道

19
中藥的迷思 天然 = 安全 ?? 其實天然物如曼陀羅花、夾竹桃等植物也 可能含有毒性物質 再好的東西若食用過量,對於健康都會造 成危害,甚至需要送醫治療。

20
中藥的迷思 西藥的殘留物會破壞身體 ?? 無論中藥或西藥, 都會經由身體代謝排泄 例外的是, 一些重金屬會與身體成分緊密結 合, 而無法很快排出 例如鉛會與骨骼組織結合, 並會破壞神經細 胞及紅血球, 所以慢性鉛中毒會有許多後遺 症 西藥對於各種有毒物質的管制甚嚴, 上市前 必須經過嚴密的化驗分析

21
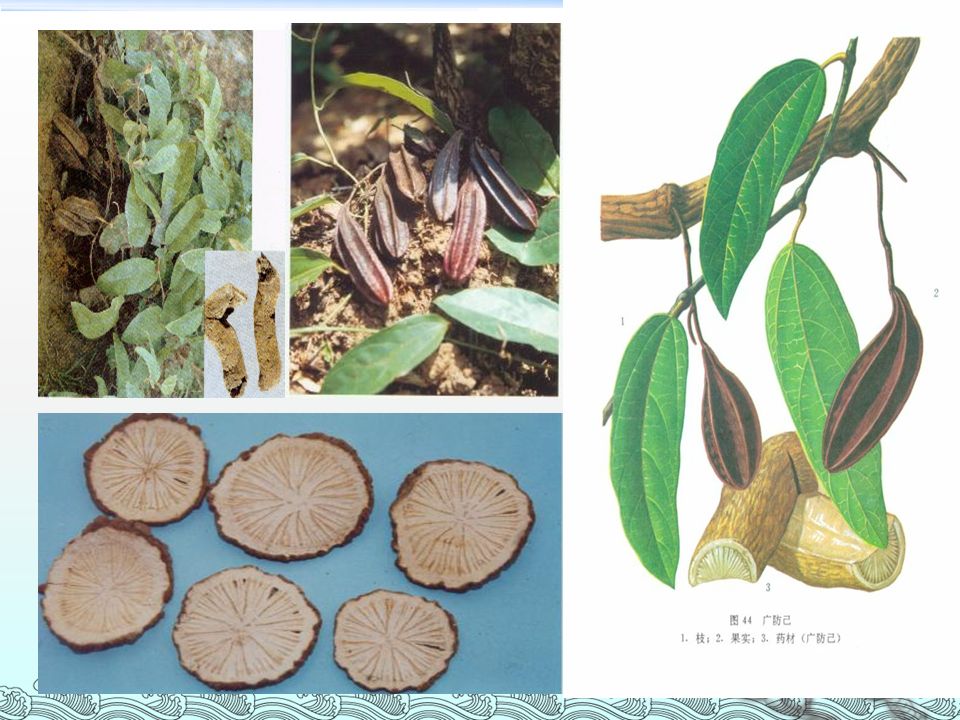
歷史 1993 年, 比利時醫師 Vanherweghem 於 Lancet 期刊中發表 : 有多名年輕女性因為吃 了某減肥診所開的減肥藥後發生急性腎衰 竭的案例,開始引起大家重視。 減肥藥中誤用了「廣防己」來取代「漢防 己」。 廣防己中所含的「馬兜鈴酸」 就是造成腎 衰竭的禍首。

23
中草藥腎病變 馬兜鈴酸已經被證實會造成間質性腎炎及 腎衰竭。 在過去許多研究中,大家習慣將這些因為 服用含中藥減肥藥而造成腎功能異常的病 例稱作「中草藥腎病變」 。 由於目前研究已經確定致病的元兇是其所 含的馬兜鈴酸成分,因此又有人建議將中 草藥腎病變改稱為「馬兜鈴酸腎病變」。

24
臨床表徵 女性為多,腎衰竭的症狀並不明顯,半數 以上病患血壓正常 與其他疾病引起的腎衰竭相比,中草藥腎 病變病患的貧血發生較早且較嚴重。 蛋白尿輕微,尿液沉渣檢查無明顯異常。

25
臨床表徵 即使停用中草藥,腎功能損害仍持續進展 腎功能的惡化速度與用藥時間長短成正比, 與停藥到發病診斷的時間間隔成反比。 病人從開始服用減肥藥到腎衰竭接受洗腎 治療,平均時間約 5-20 個月。

26
泌尿細胞上皮癌 馬兜鈴酸造成上皮細胞癌症特點是 : (1) 主要發生於「上泌尿道」。 (2) 潛伏期相當短。 (3) 可能在沒有發生腎衰竭之前便罹患癌 症。 高達 46% 的人有上泌尿道變形細胞癌。 這些癌症患者平均服用減肥藥的時間是 15 個月 馬兜鈴酸累積劑量與其是否會造成癌症有關。
 主要發生於「上泌尿道」。 (2) 潛伏期相當短。 (3) 可能在沒有發生腎衰竭之前便罹患癌 症。 高達 46% 的人有上泌尿道變形細胞癌。 這些癌症患者平均服用減肥藥的時間是 15 個月 馬兜鈴酸累積劑量與其是否會造成癌症有關。")
27
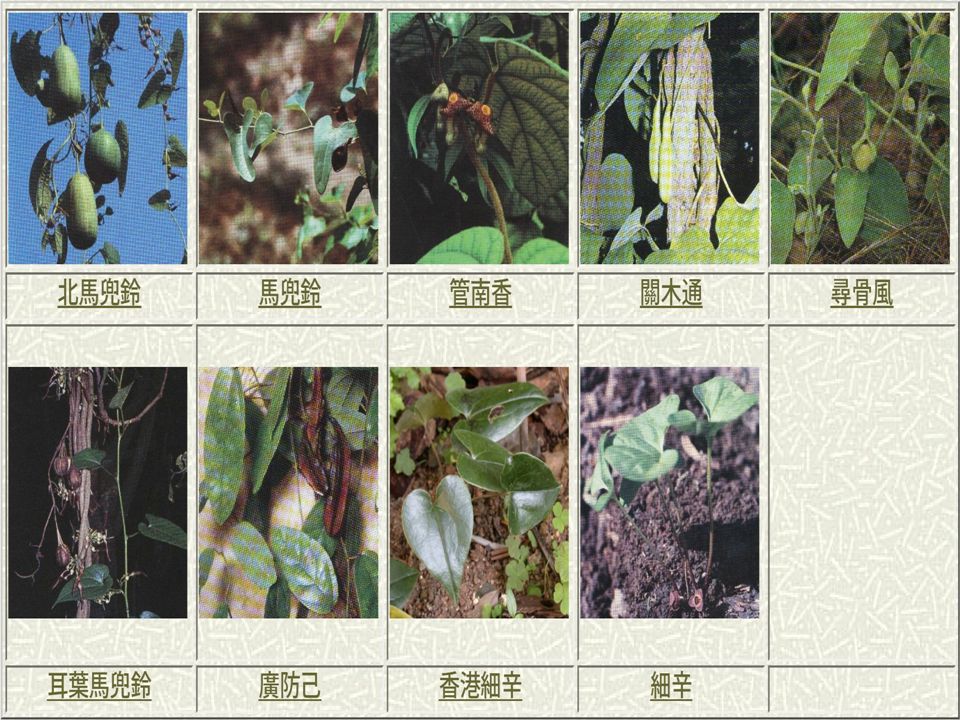
哪些中藥含有馬兜鈴酸 ? 馬兜鈴酸是馬兜鈴屬 (Aristolochia) 植物的主 要成分,常見臺灣市售中藥材中含馬兜鈴 酸成份的有「廣防己」、「關木通」、 「馬兜鈴」、「天仙藤」、「青木香」、 「細辛」 、 「威靈仙」 。 行政院衛生署已於 92 年 11 月 4 日公告禁用這 些藥材。
 植物的主 要成分,常見臺灣市售中藥材中含馬兜鈴 酸成份的有「廣防己」、「關木通」、 「馬兜鈴」、「天仙藤」、「青木香」、 「細辛」 、 「威靈仙」 。 行政院衛生署已於 92 年 11 月 4 日公告禁用這 些藥材。.")
29
對腎臟有害的方劑 含木通 : 八正散、八味帶下方、甘露消毒丹、 辛夷散、泌尿煎、消風散、疏鑿引、當歸四逆 湯、過期飲、導赤散、龍膽瀉肝湯、變製心氣 飲。 含防己 : 上中下通用痛風丸、小續命湯、防己 黃耆湯、疏經活血湯。 含馬兜鈴 : 補肺阿膠散。 含細辛 : 獨活寄生湯、九味羌活湯、川芎茶調 散、小青龍湯、辛夷散、金沸草散、苓甘薑味 辛夏仁湯、麻黃附子細辛湯。

30
其他各國行動 1994 年,法國率先禁售含馬兜鈴酸的中藥, 接下來英國、比利時、澳大利亞、奧地利、 西班牙、美國、埃及等多國亦陸續對含有 馬兜鈴酸的中草藥發出禁令。 2003 年底,台灣地區衛生署中醫委員會正 式宣布禁用含馬兜鈴酸的馬兜鈴、關木通、 天仙藤、青木香和廣防己等五種藥材及製 劑,因此有 69 種中藥製品也必須在藥店禁 售。

31
現今衛生署規定 禁止進口及銷售含馬兜鈴酸的藥材,包括馬兜 鈴屬的關木通、青木香、馬兜鈴、尋骨風、廣 防己,及細辛屬包括細辛全草(除根部外)等。 細辛藥材,只可用根部入藥,成人一日常用量 不可超過 1 錢或 3 克。細辛藥材應以水煎煮後服 用,時間不應少於 60 分鐘;不應磨粉內服。細 辛的藥用品種必須為馬兜鈴科品種北細辛、漢 城細辛及華細辛。 細辛藥材應在中醫師指導下使用,而中藥材零 售商應從領有牌照的批發商購貨及按中醫師處 方配發細辛藥材。
等。 細辛藥材,只可用根部入藥,成人一日常用量 不可超過 1 錢或 3 克。細辛藥材應以水煎煮後服 用,時間不應少於 60 分鐘;不應磨粉內服。細 辛的藥用品種必須為馬兜鈴科品種北細辛、漢 城細辛及華細辛。 細辛藥材應在中醫師指導下使用,而中藥材零 售商應從領有牌照的批發商購貨及按中醫師處 方配發細辛藥材。")
32
結論 根據以上國內外的研究報告,雖然中草藥 用於治療疾病已有多年歷史,在很多疾病 治療中亦有很好的效果,但一樣存在一定 的毒副作用。 中草藥的使用存在許多問題,由於中草藥 多為植物的根或莖葉,常見同一中藥名稱 有若干不同種的植物的情形,但其中的毒 性作用並不相同;此外,中藥的產地和炮 製方法也可能影響中草藥的腎毒性。

33
含碘顯影劑引發之急性腎衰竭 Radiocontrast media-induced acute renal failure

34
定義 Acute decline in renal function following the administration of intravenous contrast medium in the absence of other causes An acute rise in serum creatinine from 24 to 48 hours after the contrast study Absolute increase of Cr > 0.5 mg/dL or relative increase 25 to 50% from baseline Serum creatinine generally peaks at 3 to 5 days and returns to baseline by 7 to 10 days JASN 2000;11:177-82

35
發生率 Mild, transient decrease in GFR occur in almost all patient Whether clinical significant ARF develops depends on presence of risk factors The incidence depends upon its definition and the characteristics of the study population Incidence: 3% (low risk) – 100% (with for risk factors)
 – 100% (with for risk factors)")
36
危險因子 for contrast nephropathy Preexisting renal impairment Diabetes mellitus Decrease in effective arterial volume dehydration congestive heart failure nephrosis cirrhosis High doses of contrast Concurrent use of nephrotoxic drugs nonsteroidal anti-inflammatory drugs angiotensin-converting enzyme inhibitors

37
臨床表現 Non-oliguria or oliguria? Low urine sodium concentration and FENa Urinalysis: Renal tubular epithelial cell casts, course granular brown cast, amorphous urate crystal Minimal proteinuria Persistent nephrogram (24-48 hours)
.")
38
預防 General consideration Identify high risk patients Absolute indication Correcting risk factors before contrast administration Lowest dose of contrast media Monitor renal function

39
預防 Fluid administration Nonionic and low-osmolality media Furosemide (?) Mannitol (?) Dopamine (?) Atrial natriuretic peptide (?) Calcium channel blocker Theophylline Hemodialysis N-acetylcysteine
 Mannitol ( ) Dopamine ( ) Atrial natriuretic peptide ( ) Calcium channel blocker Theophylline Hemodialysis N-acetylcysteine")
40
Acetylcysteine 的角色 2000 年 7 月 Tepel 發表於 NEJM 之報導指出,口服 投予 acetylcysteine ,不需要高深的技術卻似乎可 有效的改善顯影劑引起之腎病變。 實驗中 83 位接受電腦斷層檢查之慢性腎功能不良 患者(平均血清 creatinine(Scr) 濃度為 2.4 ± 1.3 mg/dl ),以非離子性、低滲透壓之 iopromide 為 顯影劑(其引起急性腎衰竭之可能性較高滲透壓 顯影劑來的低),患者隨機接受抗氧化劑 acetylcysteine ( 顯影劑給予之前一天及當天口服 600 mg 每天 2 次 ) 及 0.45% 食鹽水(顯影劑給予前 後 12 小時以 1ml/kg/hr 速率靜脈注射)或接受安慰 劑及生理食鹽水。結果 83 位中有十位 (12%) 在顯 影劑給予後 48 小時, Scr 濃度增加至少 0.5mg/dl ,其中 acetylcysteine 組:安慰劑組 =1/41 : 9/42 (2% : 21 %) 。
 濃度為 2.4 ± 1.3 mg/dl ),以非離子性、低滲透壓之 iopromide 為 顯影劑(其引起急性腎衰竭之可能性較高滲透壓 顯影劑來的低),患者隨機接受抗氧化劑 acetylcysteine ( 顯影劑給予之前一天及當天口服 600 mg 每天 2 次 ) 及 0.45% 食鹽水(顯影劑給予前 後 12 小時以 1ml/kg/hr 速率靜脈注射)或接受安慰 劑及生理食鹽水。結果 83 位中有十位 (12%) 在顯 影劑給予後 48 小時, Scr 濃度增加至少 0.5mg/dl ,其中 acetylcysteine 組:安慰劑組 =1/41 : 9/42 (2% : 21 %) 。")
41
Gadolinium 與系統性腎臟 纖維化病變 (Nephrogenic Systemic Fibrosis, NSF)
")
42
4 種顯影劑 衛生署指出,使用美格維斯造影注射液、得立顯 注射劑、摩立顯及麥林可歐得麥造影劑時,醫師 應審慎評估患者可能發生系統性腎臟纖維化病變 的風險。 美國食品藥物管理局日前發布含有 gadolinium 成 分顯影劑的藥品,應加註嚴重腎臟疾病患者、或 肝臟移植前後曾有嚴重腎功能不全、或慢性肝病 患者,使用含上述成分的磁振造影顯影劑時,可 能會發生系統性腎臟纖維化病變。 藥政處指出,系統性腎臟纖維化病變會發生皮膚 結締組織變厚,進而抑制行動能力,有可能導致 骨折,目前對於發生原因及治療方法未明。

43
Gadolinium (Gd) A rare earth element from the lathanide series Its seven unpaired electrons 擾亂 proton relaxation in water => ↓ T1 relaxation time,↑magnetic resonance signal intensity Gd in its unbound state is highly toxic It is a potent inhibitor of calcium channels and has considerable CV and neurologic toxicity
 A rare earth element from the lathanide series Its seven unpaired electrons 擾亂 proton relaxation in water => ↓ T1 relaxation time,↑magnetic resonance signal intensity Gd in its unbound state is highly toxic It is a potent inhibitor of calcium channels and has considerable CV and neurologic toxicity")
44
Nature Clinical Practice Nephrology 2007, Vol 3 (12), 654-668
,")
45
Weiss A S et al. (2007) A case of nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis Nat Clin Pract Nephrol 3: 111–115 doi:10.1038/ncpneph0373 Figure 1 Skin thickening, tightness and contractures are hallmarks of the clinical findings in nephrogenic fibrosing dermopathy
 A case of nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis Nat Clin Pract Nephrol 3: 111–115 doi: /ncpneph0373 Figure 1 Skin thickening, tightness and contractures are hallmarks of the clinical findings in nephrogenic fibrosing dermopathy.")
46
系統性腎臟纖維化病變的臨床表現 Progression: rapid in a subset of pts Increased risk of thrombosis: DVT, PE… Antiphospholipid and anticardiolipin Ab↑ Deficiencies of protein C, protein S and antithrombin III; presence of factor V Leiden Liver disease or post liver transplantation Involve fascia, subcutaneous tissue, and lungs, heart, kidneys, dura mater and testes…

47
治療 Often unsuccessful NSF can improve with recovery of renal function (after successful kidney tx or resolution of AKI) UV A1, plasmapheresis: 各 1 人 Extracorporeal photopheresis: 3 人 Sodium thiosulfate: 1 人 (ESRD under HD) IVIG: 1 人, PD, partial Physical therapy
 UV A1, plasmapheresis: 各 1 人 Extracorporeal photopheresis: 3 人 Sodium thiosulfate: 1 人 (ESRD under HD) IVIG: 1 人, PD, partial Physical therapy")
48
血液透析 Sequestration of Gd in interstitial or intracellular compartments would be erroneously interpreted as dialytic removal => 不準 Half-life of Gd during HD: 2.6± 0.4 hr Low-flux, 4hr, TIW => one HD session removed 65% of Gd Okada: 72.8%, 95.6%, 98.7%, 99.5%

49
Recommendations for Use of Gd FDA, Danish Medicine Agency (DMA), United Kingdom Medicines and Healthcare products Regulatory Agency (MHRA), and American College of Radiology (ACR) FDA: all Gd chelates are potentially linked to NSF DMA, MHRA: Gadodiamide: contraindicated in pts with GFR < 30 mL/min/1.73 m 2 Gadoversetamide, gadopentetate dimeglumine: 沒 建議
, United Kingdom Medicines and Healthcare products Regulatory Agency (MHRA), and American College of Radiology (ACR) FDA: all Gd chelates are potentially linked to NSF DMA, MHRA: Gadodiamide: contraindicated in pts with GFR < 30 mL/min/1.73 m 2 Gadoversetamide, gadopentetate dimeglumine: 沒 建議")
50
Recommendations for Use of Gd Standard Gd doses should not be exceeded Repeat doses should not be given in < 1 week

51
Recommendations for Use of Gd Most controversial issue: post-Gd HD? The most recent FDA update: prompt post- Gd dialysis only in pts who were already on HD (prompt ?) ACR: HD within 2 hrs of Gd administration in pts already on HD (no evidence) Broome: 3 pts developing NSF despite 3 consecutive daily HD!
 ACR: HD within 2 hrs of Gd administration in pts already on HD (no evidence) Broome: 3 pts developing NSF despite 3 consecutive daily HD!.")
52
Recommendations for Use of Gd CKD stage 3 or 4 pts, NSF after Gd administration 的 risk↑ Exposure > 1 次, liver graft recipients, MDRD overestimate true GFR… GFR 越低, risk 越高, ESRD 2.5% 應盡量 postpone any Gd-enhanced imaging procedures in AKI pts

53
治療慢性腎病的一般建議 治療原發性疾病 避免腎毒性藥物及中藥止痛藥 及早發現與治療高血壓 適當時機開始低蛋白質飲食 治療相關的併發症 53

54
謝謝聆聽 敬請指教 祝大家平安健康!

Similar presentations

 Regulate fluid, electrolyte Acid-base balance 調整血壓:經由腎素體系進行調節。>")
. 止痛剂肾病 NSAID-associated nephropathy Classic analgesic nephropathy.>")



. 病因( Etiologe ) Primery Glomerular Diseases (60%) Hypertensive Nephrosclerosis Diabetic Glomerulosclerosis >")
 病理生理学系 Department of Pathophysiology 高远生.>")






.>")



 河南中医学院第一附属医院 杜正光>")
