Download presentation
Presentation is loading. Please wait.

1
1 Preoperative Portal Vein Embolization for Hilar Cholangiocarcinoma - a Comparative Study 肝门部胆管癌术前门静脉栓塞的对比研究 作者姓名:易滨 1, 徐爱民 1, 赖俊雄 1,2, 曲增强 1, 程庆保 1, 刘辰 1, 罗祥基 1, 于勇 1, 邱应和 1, 王晓琰 1, 程红岩 1, 张柏和 1, 沈锋 1, 刘允怡 1,2, 吴孟超 1, 姜小清 1 作者单位: 1 东方肝胆外科医院,第二军医大学 2 医学系,香港中文大学 第一作者姓名及身份证号码:易滨 310110197404278619 通讯作者姓名:姜小清

2
根治性切除 是肝门胆管癌患者长期存活的唯一机 会;半肝 / 扩大的半肝切除是主要的手术方式。 门静脉栓塞术 能够诱导栓塞肝叶萎缩和对侧肝叶 增生;使未来残余肝( FLR )偏小的边缘候选患 者、被排除于肝切除之外的患者获得根治切除的 机会。 1 、研究背景
偏小的边缘候选患 者、被排除于肝切除之外的患者获得根治切除的 机会。 1 、研究背景")
3
2 、材料与方法 PVE group (n=16)Non-PVE group (n=33)P-value Sex Male Female 11 5 20 13 0.754 Age (years)54±855±110.705 Number of tumors*1 (range, 1-6)1 (range, 1-4)0.161 Size of the tumors (cm)*2.9 (range, 2.0-5.1)2.8 (range, 2.0-5.2)0.983 Bismuth-Corlette classification I II IIIa IIIb IV 0 2 0 14 0 4 19 10 <0.001 Preoperative biliary drainage (n) PTBD Endoscopic stenting Other methods None 13 1 2 0 14 2 0 17 0.002 Preoperative peak bilirubin level (μmol/L)303.5±173.3234.1±155.50.165 Preoperative biliruibin level (μmol/L)46.7±24.9132.0±123.00.009 Future liver remnant/Total liver volume (%) at presentation 40.3±7.456.6±5.0<0.001 Future liver remnant/Total liver volume (%) before surgery 43.1±7.056.6±5.0<0.001 Table 1. Patients Characteristics

4
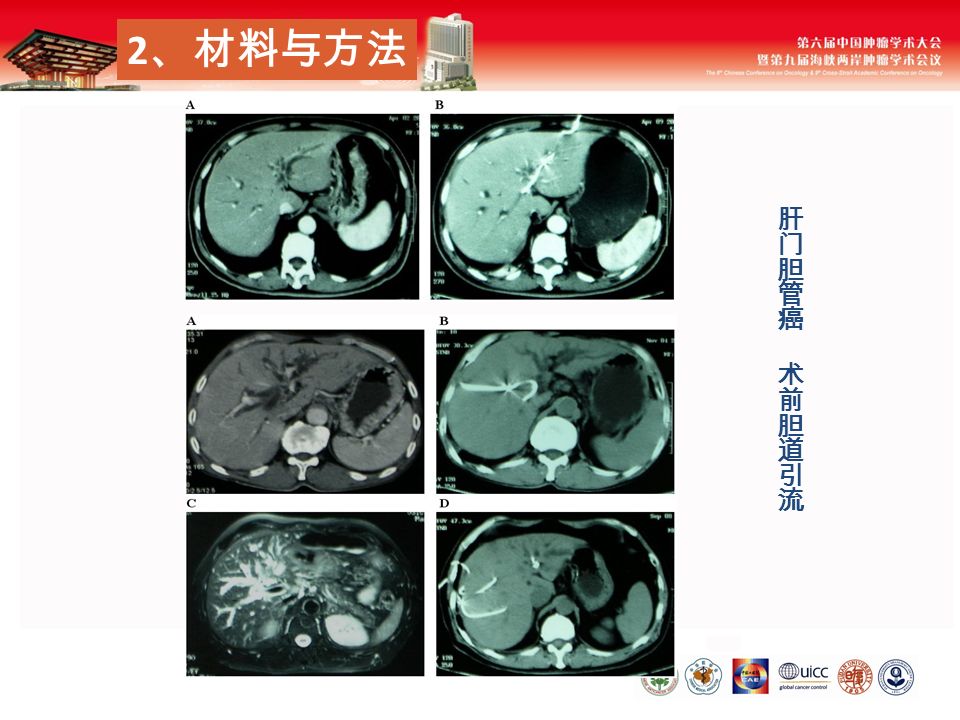
2 、材料与方法

6
器械: 19G 穿刺针、 5F 造影导管。采用同侧或 对侧路径法。栓塞材料:钢圈( MWCE-35-5-8, Cook, 美国)。栓塞目标:门静脉肝段分支,尽 可能达到预切除肝叶门静脉支的完全栓塞。 在 PVE 前、后进行血清学检查,评价肝功、生 化指标的变化。栓塞 / 非栓塞肝叶 CT 肝体积测定, 计算 FLR 体积 及 FLR/TLV 。 2 、材料与方法
。栓塞目标:门静脉肝段分支,尽 可能达到预切除肝叶门静脉支的完全栓塞。 在 PVE 前、后进行血清学检查,评价肝功、生 化指标的变化。栓塞 / 非栓塞肝叶 CT 肝体积测定, 计算 FLR 体积 及 FLR/TLV 。 2 、材料与方法")
7
PVE 前 PVE 后 门静脉造影 2 、材料与方法

8
Figure 1. Management Flow Chart Jan. 2007 ~ Mar. 2009

9
3 、结果 ——PVE 并发症 PVE 并发症: 3 例( 18.8 %)。 16 例均成功,无 靶静脉再通、肝脏坏死。 胆漏: 1 例,经皮腹腔置管引流,不影响手术。 钢圈移位: 2 例,均不影响手术。
。 16 例均成功,无 靶静脉再通、肝脏坏死。 胆漏: 1 例,经皮腹腔置管引流,不影响手术。 钢圈移位: 2 例,均不影响手术。")
10
3 、结果 ——PVE 前后肝功能 Table 3. Liver function profile after PVE TimingValueP-value Total bilirubin (μmol/L) Before PVE Day 3 Day 7 Day 14 83.7±40.7 80.3±37.8 67.5±35.9 53.5±31.2 0.194 0.010 0.001 The data after PVE did not have statistic difference in ALT, AST, γ- GT and ALP. PVE 后 2 周 非栓塞肝叶体积 有统计学差异 ( 892±278cm3 vs 958±285cm3 , P<0.001 ) 体积增加 66±36 cm3 ,肝增生速度 5.1±2.7cm3/d 非栓塞肝 / 全肝体积 有统计学差异 ( 48.5±12.6% vs 51.8±12.4% , P<0.001 ) 体积比增加 3.3 ± 2.6%
 Before PVE Day 3 Day 7 Day ± ± ± ± The data after PVE did not have statistic difference in ALT, AST, γ- GT and ALP. PVE 后 2 周 非栓塞肝叶体积 有统计学差异 ( 892±278cm3 vs 958±285cm3 , P<0.001 ) 体积增加 66±36 cm3 ,肝增生速度 5.1±2.7cm3/d 非栓塞肝 / 全肝体积 有统计学差异 ( 48.5±12.6% vs 51.8±12.4% , P<0.001 ) 体积比增加 3.3 ± 2.6%.")
11
PVE 后 2 周 未来残余肝体积 有统计学差异 ( 744±198cm3 vs 802±216cm3 , P<0.001 ) 体积增加 59±38 cm3 ,肝增生速度 4.6±3.0cm3/d 未来残肝 / 全肝体积 有统计学差异 ( 40.3±7.4% vs 43.1±7.0% , P<0.001 ) 体积比增加 2.8±2.1% 3 、结果 ——PVE 前后肝体积
 体积增加 59±38 cm3 ,肝增生速度 4.6±3.0cm3/d 未来残肝 / 全肝体积 有统计学差异 ( 40.3±7.4% vs 43.1±7.0% , P<0.001 ) 体积比增加 2.8±2.1% 3 、结果 ——PVE 前后肝体积")
12
PVE 后 2 周 栓塞肝叶体积 有统计学差异 ( 953±300cm3 vs 899±300cm3 , P=0.038 ) 体积减少 55±96 cm3 ,肝萎缩速度 3.7±6.9cm3/d 栓塞肝叶 / 全肝体积 有统计学差异 ( 51.5±12.6% vs 48.2±12.4% , P<0.001 ) 体积比减少 3.3±2.6% 3 、结果 ——PVE 前后肝体积
 体积减少 55±96 cm3 ,肝萎缩速度 3.7±6.9cm3/d 栓塞肝叶 / 全肝体积 有统计学差异 ( 51.5±12.6% vs 48.2±12.4% , P<0.001 ) 体积比减少 3.3±2.6% 3 、结果 ——PVE 前后肝体积")
13
3 、结果 PVE group (n=13)Non-PVE group (n=33)P-value Type of hepatectomy* (n) Extended right hepatectomy Right hepatectomy Extended left hepatectomy Left hepatectomy Concomitant procedure (n) Portal vein resection with reconstruction Hepatic artery resection with reconstruction Pancreatoduodenectomy 62504006250400 4 2 5 22 9 4 0 0.001 1.000 0.313 --- Duration of operation (minutes)447±57395±830.043 Blood loss (ml)1462±11061070±8310.198 Blood transfusion (unit)11±58±58±50.108 Number of patients with complications (n) Complications (n) Prolonged hyperbilirubinemia Bleeding Bile leakage Hepaticojejunostomy leakage Intra-abdominal collection/abscess Reoperation (n) 9 (69.2%) 2 1 2 0 5 0 21 (63.6%) 4 5 2 0 12 1 1.000 Hospital mortality (n)0 (0%)3 (9.1%)0.548 Length of post-operative hospital stay (days)40±1929±290.203 Surgical margins (n) R0 R1 12 1 26 7 0.409 Table 2. Operative details and outcomes

15
3 、结果 Figure 3. Overall Survival - PVE group (with intention-to-treat analysis) vs. Non PVE group. P=0.244; PVE group (hepatectomy only) vs. Non PVE group. P=0.844
 vs. Non PVE group. P=")
16
Abulkhir A, Limongelli P, Healey AJ, et al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg, 2008;247(1):49-57. 4 、讨论 —PVE 的安全性
: 、讨论 —PVE 的安全性.")
17
在 SBD 基础上, TB 可作为反映 FLR 功能的良好 指标。 PVE 后 TB 持续下降, PVE 后 7d 差异既有 统计学意义。 PVE 能够促进 FLR 功能的代偿和体积的增生。 PVE 组耐受了更大范围的肝切除,而术后并发 症发生率和死亡率并不比非 PVE 组高。 4 、讨论 — 本组 PVE 促进肝再生的效果 TimingValueP-value Total bilirubin (μmol/L) Before PVE Day 3 Day 7 Day 14 83.7±40.7 80.3±37.8 67.5±35.9 53.5±31.2 0.194 0.010 0.001 Table 3. Liver function profile after PVE

18
5 、结论 本研究的结果显示: 对于未来残余肝偏小的肝门部胆管癌患者, 其可能是根治手术的边缘患者或被排除于手 术之外,而门静脉栓塞能够提供安全的、可 能是根治性的大部肝切除机会。

19
Thank You Expo China Pavilion 2010

Similar presentations


. What Is Cirrhosis? 肝硬化是一种慢性疾病,可由多种原因 引起,肝细胞弥漫性变性坏死,继而出 现纤维组织增生;肝细胞结节状再生 ; 这 三种改变反复交错进行,结果肝小叶结 构和血液循环途径逐渐被改建,致使肝 脏变形、变硬而形成肝硬变,早期可无.>")







,皮肤、巩膜、黏膜、 体液及其它组织黄染,临床出现黄疸 血清中总胆红素浓度增高达 34.2 mol/L 以上 (2.0mg/dl ),皮肤、巩膜、黏膜、 体液及其它组织黄染,临床出现黄疸.>")
>")
正常粪便的观察 1. 量与次数 排便是人体基本生理需要,每日排便量与食 物 的种类、数量及消化器官的功能有关。一般成人每日排便 1 ~ 2 次(婴幼儿 3 ~ 5 次),平均量 100 ~ 300g 。 2. 形状与颜色 正常粪便柔软成形,呈黄褐色,婴儿的粪 便呈黄色或金黄色。粪便的颜色也因摄入的食物和药物.>")







