Download presentation
Presentation is loading. Please wait.

1
中心动脉压与血管功能 大连医科大学附属一院心内科 姜一农

2
1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究
内 容 1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究

3
1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究
内 容 1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究

4
动脉压相关因素 心搏量 末梢阻力 血管壁硬度 反射波

5
中心动脉压 主动脉顺应性(大血管硬度) 反射波 时间 幅度
 反射波 时间 幅度")
6
Aortic compliance and pulse pressure
Windkessel function Normal 60% Diastole Systole 60% 40% Decreased aortic compliance 50% Systole Diastole 50% 50% London and Guerin. Am Heart J 1999;138:

7
主动脉顺应性下降 大动脉顺应性降低,弹性降低,收缩压力在动脉内不能得到缓冲,使收缩压升高。 舒张期大血管弹性回缩减低,使舒张压降低。
结果:脉压增大

8
Augmentation and reflection wave
Incident wave Reflection wave McDonald’s fourth edition

9
Arterial pressure waveform and reflection wave
Systolic BP Augmentation Index Diastolic BP Arrival of reflection wave

10
反射波机制对中心动脉压的影响 脉搏波传导速度(PWV) --反射波速度 阻力微、小动脉—反射位点 动脉弹性--反射波幅度
心率--反射波在收缩期叠加的幅度

11
AI与主动脉压、脉压的测量

14
1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究
内 容 1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究

15
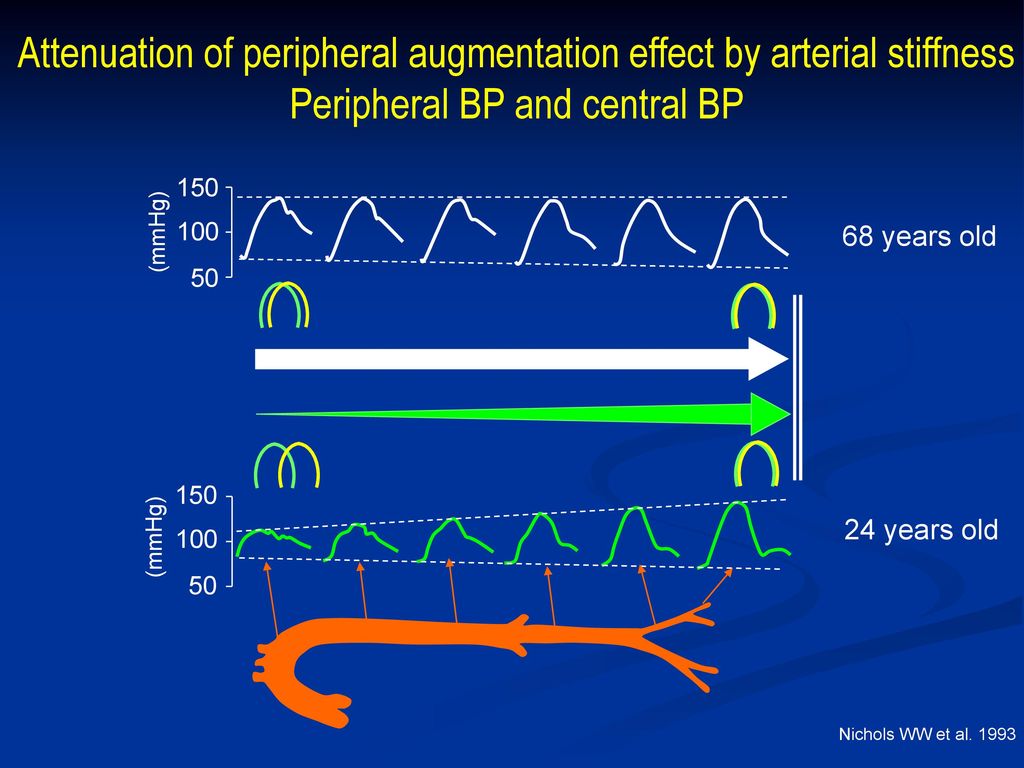
Attenuation of peripheral augmentation effect by arterial stiffness
Peripheral BP and central BP 150 (mmHg) 100 68 years old 50 150 24 years old (mmHg) 100 50 Nichols WW et al. 1993
 years old years old. (mmHg) Nichols WW et al")
16
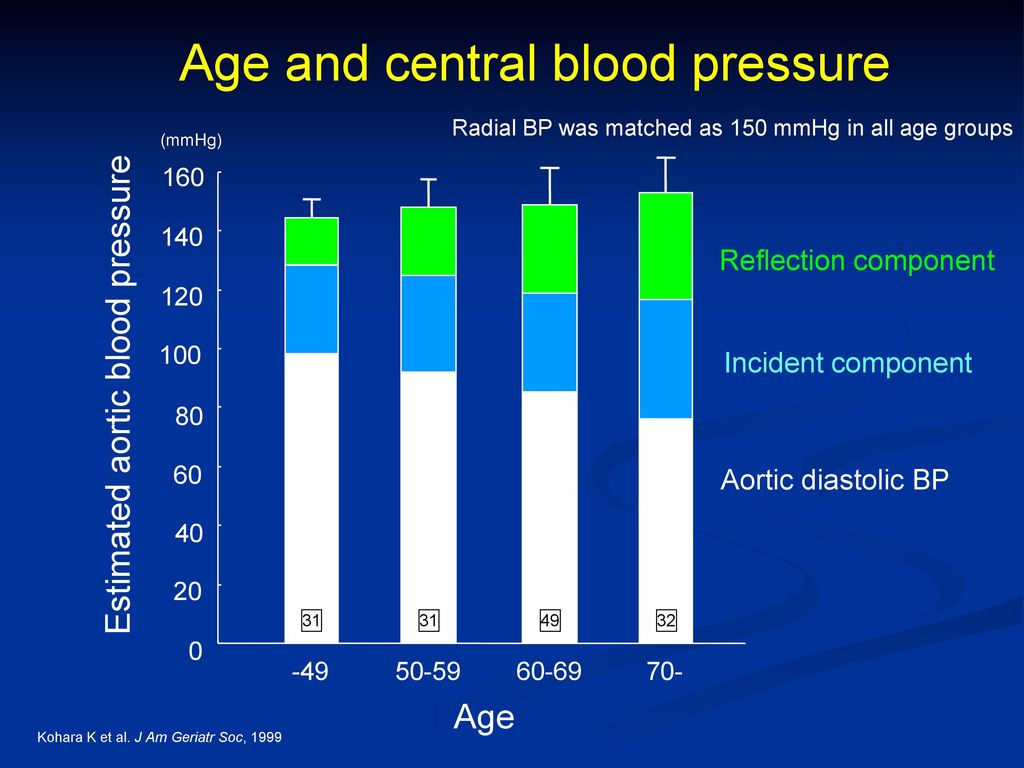
Estimated aortic blood pressure
Age and central blood pressure Radial BP was matched as 150 mmHg in all age groups (mmHg) 160 140 Reflection component 120 100 Incident component Estimated aortic blood pressure 80 60 Aortic diastolic BP 40 20 31 31 49 32 -49 50-59 60-69 70- Age Kohara K et al. J Am Geriatr Soc, 1999
 Reflection component Incident component. Estimated aortic blood pressure Aortic diastolic BP Age. Kohara K et al. J Am Geriatr Soc,")
17
Systolic hypertension
Arterial stiffness augmentation by reflection pressure wave Reduced compliance Impaired Windkessel function Central hypertension Systolic hypertension Wide pulse pressure

18
The Great Hemodynamic Divide
Mean Pressure Pulse Pressure Anatomy Heart, small arteries Aorta Physiology ↑ Cardiac output ↑ Stiffiness ↑ Peripheral resistance BP ↑ SBP ,↑ DBP ↑ SBP ↓ DBP Event ↑Risk ↑↑↑Risk

19
2662 patients, 63yrs, follow-up 3.4y
The Strong Heart Study Central Blood Pressure Better predicts Cardiovascular Events than Does Peripheral Blood Pressure 2662 patients, 63yrs, follow-up 3.4y Roman MJ, et al. AHA Sept. 2005

20
The Strong Heart Study: Cox regression analyses (校正年龄、性别、体重指数、吸烟、LDL-C、DM)
主动脉SBP和PP与CVD发生率独立相关,RR/10mmHg分别为1.07与1.10, p分别为0.043与0.009。 进一步校正颈动脉粥样硬化病变,主动脉PP仍然与CVD显著独立相关。

21
Reflection of pressure wave as risk factor
ESRD patients 1.0 PWV<9.4m/s 这些方法评价的动脉功能在各种高危人群中和终点事件关系如何来看机组流行病学调查数据 1.0 Augmentation index 1 群 Augmentation index 2 群 9.4≦PWV≦12.0m/s 0.75 0.75 Even free rate for cardiovascular accidents Survival rate for cardiovascular death 0.50 12.0m/s <PWV 0.50 Augmentation index 3 群 0.25 0.25 Augmentation index 4 群 35 70 105 140 35 70 105 140 Time (month) Time (month) Blacher et al. Circulation, 1999 London GM et al. Hypertension, 2001
 Time (month) Blacher et al. Circulation, London GM et al. Hypertension,")
22
中心动脉压和脉压升高对 心血管系统影响 左室后负荷增加,左室重构 冠状动脉灌注下降,储备功能下降, 心肌缺血
内皮损伤和功能紊乱,动脉硬化性疾病 进展

26
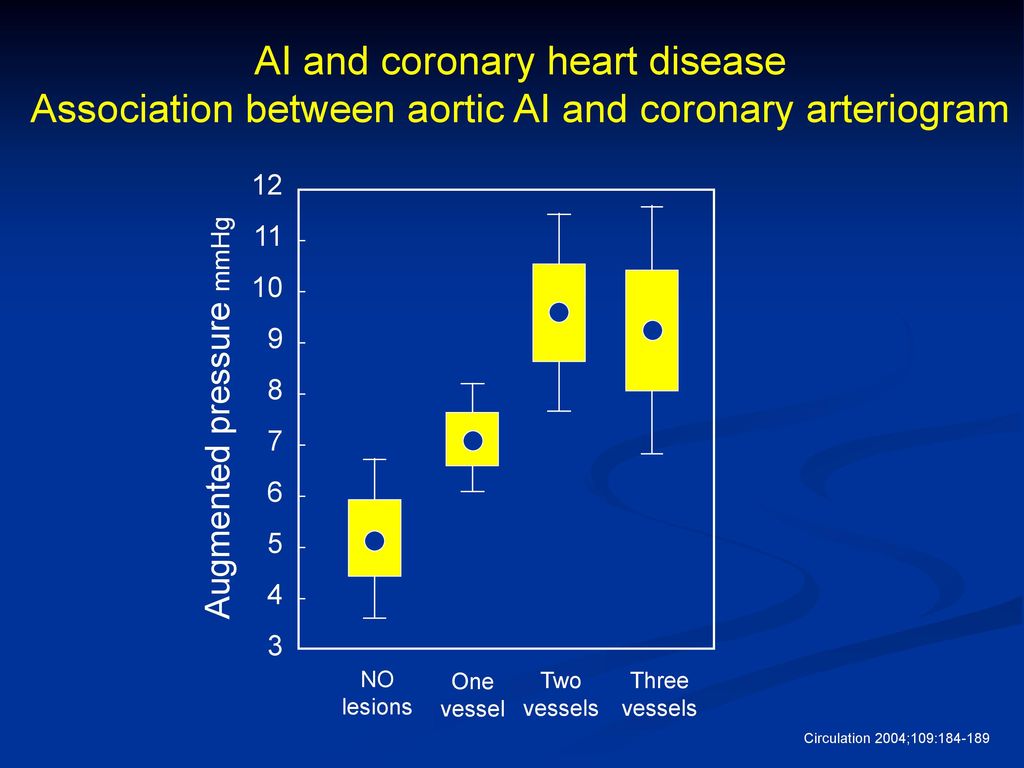
AI and coronary heart disease
Association between aortic AI and coronary arteriogram 12 11 10 9 8 7 6 5 4 3 Augmented pressure mmHg NO lesions One vessel Two vessels Three vessels Circulation 2004;109:

27
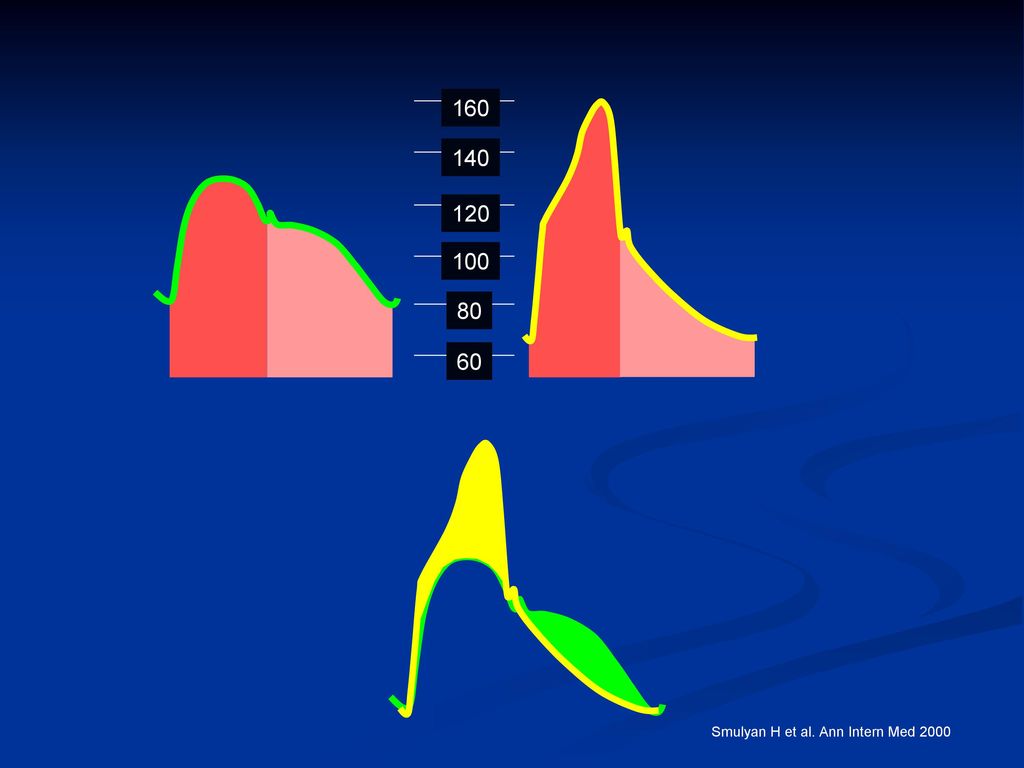
160 140 120 100 80 60 Smulyan H et al. Ann Intern Med 2000

28
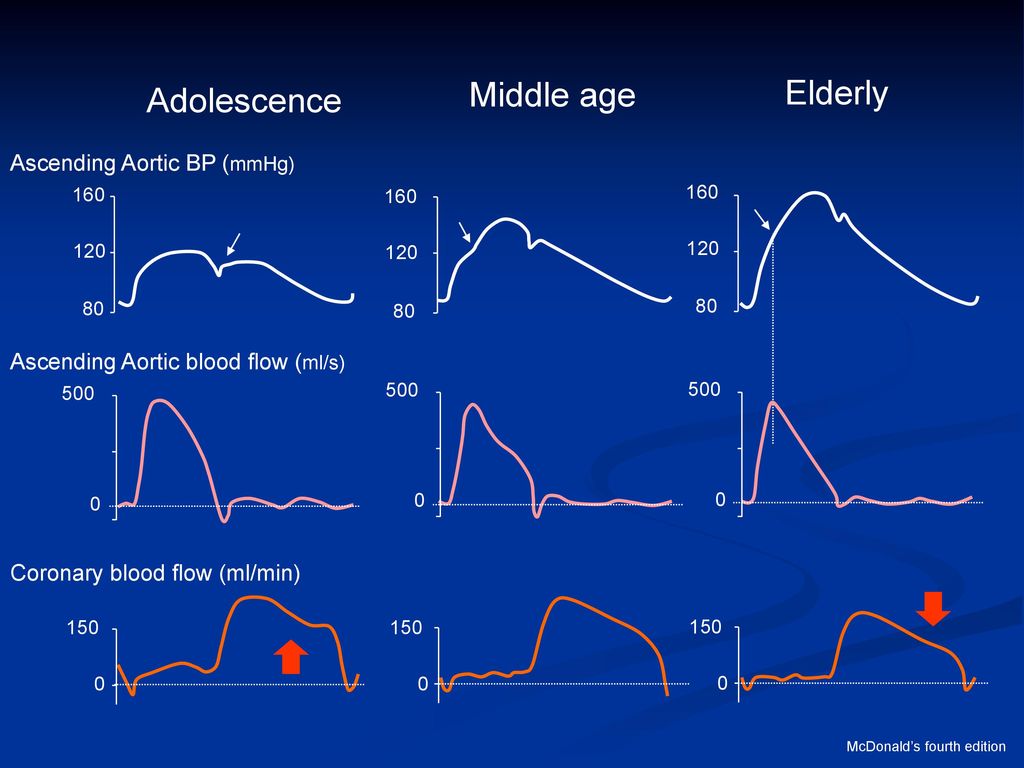
Middle age Elderly Adolescence Ascending Aortic BP (mmHg)
160 160 160 120 120 120 80 80 80 Ascending Aortic blood flow (ml/s) 500 500 500 Coronary blood flow (ml/min) 150 150 150 McDonald’s fourth edition
 Coronary blood flow (ml/min) McDonald’s fourth edition.")
29
吸烟对中心动脉压和周围动脉压的影响 Blood pressure (mmHg) Aortic AI (%) Brachial BP
Non-smoker (n=116) Smokers (n=41) * 140 2 130 1 120 * 110 -1 -2 100 Blood pressure (mmHg) Aortic AI (%) -3 90 -4 80 -5 70 -6 60 -7 * p<0.05 50 -8 Brachial BP Aortic BP Hypertension. 2003;41:
 Smokers (n=41) * * Blood pressure (mmHg) Aortic AI (%) * p< Brachial BP. Aortic BP. Hypertension. 2003;41:")
30
Hyperlipidemia and central BP
160 150 140 130 120 110 100 90 80 70 0.01 Peripheral BP Central BP Blood pressure (mmHg) * Control subjects (n=68) Hyperlipidemia (n=68) J Am Coll Cardiol 2002;39:1005
 * Control subjects. (n=68) Hyperlipidemia. (n=68) J Am Coll Cardiol 2002;39:1005.")
31
Glucose intolerance and arterial stiffness
The Hoorn Study Control Impaired glucose tolerance Type 2 DM 60 55 50 45 40 1.2 1.0 0.8 0.6 34 33 32 31 30 * * * * carotid artery to femoral artery (msec) Transmission time from Total arterial compliance (SV/carotid PP, ml/mmHg) Augmentation index (%) 243 129 256 120 74 125 261 170 188 Hypertension 43:176–181, 2004
 Transmission time from. Total arterial compliance. (SV/carotid PP, ml/mmHg) Augmentation index. (%) Hypertension 43:176–181,")
32
Effect of antihypertensive drugs on brachial BP and central BP
Diastolic BP on brachial artery was matched for 1 year 4 3 -0.2 -2 2 * -0.4 1 -4 Change in PWV (m/sec) Change in AI (%) Change in HR (bpm) -0.6 -1 -6 -0.8 -2 -3 -8 -1 -4 ** -1.2 -5 -10 Mean±SD. *p<0.05, ** p<0.001 vs atenolol. Perindopril / indapamide (n=204) atenolol (n=202) Asmar RG, et al. Hypertension. 2001;38:922
 Change in AI (%) Change in HR (bpm) ** Mean±SD. *p<0.05, ** p<0.001 vs atenolol. Perindopril / indapamide (n=204) atenolol (n=202) Asmar RG, et al. Hypertension. 2001;38:922.")
33
Effect of antihypertensive drugs double blind and cross-over study
170 32 elderly hypertensive patients (age 65-80) were treated for 4 weeks each drugs in double blind and cross-over fashion. 160 150 * * * * 140 * 130 peripheral central Blood pressure (mmHg) 120 * * * * * 110 100 90 80 * * 70 Ca channel blocker Placebo ACE inhibitor b-blocker diuretics Am J Hypertens 17:118–123, 2004
 were treated for 4 weeks each drugs in double blind and cross-over fashion * * * * 140. * 130. peripheral. central. Blood pressure (mmHg) 120. * * * * * * * 70. Ca channel. blocker. Placebo. ACE inhibitor. b-blocker. diuretics. Am J Hypertens 17:118–123,")
34
Effect of antihypertensive drugs on
AI and central BP AI Central BP diuretics ↓→ ↓ b-blocker ↑→ ↓→ ACE inhibitor/ARB ↓ ↓↓ Ca channel blocker ↓ ↓↓ 探讨各种药物作用机制,更合理地选择药物。

35
CAFÉ: 肱动脉和中心动脉收缩压 时间(年) 肱动脉收缩压 平均差异(AUC)=0.7mmHg 中心动脉收缩压
133.9 133.2 氨氯地平 阿替洛尔 P=.07 125.5 121.2 P<.0001 AUC 115 140 135 130 125 120 mm Hg 中心动脉收缩压 平均差异(AUC)=4.3mmHg 时间(年) 阿替洛尔 氨氯地平
=4.3mmHg. 时间(年) 阿替洛尔 氨氯地平")
36
CAFÉ: 血压对终点事件的影响 (未校正的多因素分析)
X2 P值 HR CI 肱动脉脉压的差值 21.0 <0.0001 1.21 中心动脉脉压的差值 17.8 1.20 中心动脉压 增强指数 7.10 0.008 1.22 P1 19.0 1.37 (经校正的多因素分析) X2 P值 HR CI 中心动脉脉压 的差值 3.91 0.048 1.11
 X2. P值. HR. CI. 中心动脉脉压. 的差值")
37
GREAT DEBATES IN HYPERTENSION: 2007ACC
Antihypertensive Therapy Should be Tailored to Measures of Arterial Stiffness Still not enough data to make this assertion. However, there is need to develop such data.

38
1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究
内 容 1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究
39
动脉血管功能改变 中、大动脉顺应性下降 舒缩功能下降 小动脉阻力增加,顺应性下降 储备能力下降 动脉血管痉挛

40
Methods for Detecting Vessel Disease
Pulse contour analysis (C1,C2) Pulse Wave Velocity (PWV) Aortic pressure augmentation (reflected waves), Pulse pressure Flow-mediated vasodilation Flow reserve Biopsy Urinary protein excretion
 Pulse Wave Velocity (PWV) Aortic pressure augmentation (reflected waves), Pulse pressure. Flow-mediated vasodilation. Flow reserve. Biopsy. Urinary protein excretion.")
41
乙酰胆碱试验 在基线期无严重的梗阻性缺损 给予乙酰胆碱后出现反常的血管收缩反应

42
血流介导的血管扩张(FMD)测量
测量")
43
动脉血管舒张功能 血管舒张 内皮依赖性舒张功能 (endothelium-dependent dilation, EDD)
非内皮依赖性舒张功能 (endothelium-independent dilatation, EID) 药物: 乙酰胆碱 生理性刺激: 反应性充血,FMD 硝普钠、 硝酸甘油等 内皮由来NO 外源NO 血管舒张
 药物: 乙酰胆碱. 生理性刺激: 反应性充血,FMD. 硝普钠、 硝酸甘油等. 内皮由来NO. 外源NO. 血管舒张.")
44
Survival without ischemic heart disease in hypertensive
patients with MA or normoalbuminuria (MONICA study) 100 <30mg/24h 95 90 P<0.003 Proportion without ischemic heart disease (%) 85 >30mg/24h 80 75 70 1 2 3 4 5 6 7 8 9 10 years (Jensen et al: Hypertension, 2000)
 100. <30mg/24h P< Proportion without ischemic heart disease (%) 85. >30mg/24h years. (Jensen et al: Hypertension, 2000)")
45
1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究 —— 我们的工作
内 容 1、中心动脉压机制与方法评价 2、中心动脉压的意义 3、血管功能指标和意义 4、血管功能指标临床研究 —— 我们的工作

46
24小时动态血压与动脉内皮功能相关性的研究 “非杓型”原发性高血压患者靶器官的损伤远较 “杓型”患者严重,心脑血管事件的发生率更高。动脉内皮功能的变化? 原发性高血压患者46名,“杓型”31名,“非杓型”15名 测定FMD(Flow mediated-dilation)
")
47
“杓型”和“非杓型”两组FMD比较 “非杓型”组 “杓型”组 FMD(%) 注:“杓型”和“非杓型”两组FMD比较,p<0.001
12 10 8 FMD(%) 6 4 2 “非杓型”组 “杓型”组 注:“杓型”和“非杓型”两组FMD比较,p<0.001
 非杓型 组. 杓型 组. 注: 杓型 和 非杓型 两组FMD比较,p<")
48
FMD与24hSBP的相关性 r=-0.438 FMD

49
FMD与年龄的相关性 r=-0.409 FMD

50
阿托伐他汀对血脂正常高血压患者血管内皮功能的影响
高血压病患者早期即有血管内皮功能失调。 他汀类药物对血脂正常高血压患者是否改善血管内皮功能?与剂量的关系?

51
阿托伐他汀对血脂正常高血压 患者FMD/ EID影响 FMD/EID(%) p<0.05 p<0.01 30 25 20
15 0周EID 4周后EID 10 5 normal ator10mg ator20mg

52
结 论 高血压病患者内皮功能失调表现为以内皮依赖性血管舒张反应减弱为特征。
结 论 高血压病患者内皮功能失调表现为以内皮依赖性血管舒张反应减弱为特征。 阿托伐他汀能改善血脂正常高血压患者血管内皮功能,可能具有剂量依赖性。

53
小 结 中心动脉压与脉压相关密切;与心血管事件相关性好;不同降压药对周围血压和中心动脉压降低不同,对评价不同降压药物作用有一定意义。
小 结 中心动脉压与脉压相关密切;与心血管事件相关性好;不同降压药对周围血压和中心动脉压降低不同,对评价不同降压药物作用有一定意义。 动脉功能评价方法多,不同侧面反映血管功能。有一定临床应用价值。

54
谢 谢

55
血管的重要性——VHP概念 Vascular disease Hypertension Prevention
作为一个整体来对待 近几年来,随着流行病学和循证医学证据的积累,血管在以高血压为代表的多种心血管疾病中的重要地位日益受到重视。

56
讨 论 高血压病患者表现为以内皮依赖性血管舒张反应减弱为特征的内皮功能失调
讨 论 高血压病患者表现为以内皮依赖性血管舒张反应减弱为特征的内皮功能失调 阿托伐他汀对内皮的保护功能非常明显,而且发生的非常早,独立于患者的脂质水平而存在,且可能剂量越大,患者的获益越大

58
结 论 “非杓型”原发性高血压患者较“杓型”的动 脉 内皮功能损伤重; 年龄、血清总胆固醇、 24小时平均收缩压是
结 论 “非杓型”原发性高血压患者较“杓型”的动 脉 内皮功能损伤重; 年龄、血清总胆固醇、 24小时平均收缩压是 影响动脉内皮功能变化的独立危险因素。

59
Center for Research Translation
RCE University Corporate Private VC Products Services R.O.I. Jobs Technology Base Funds Leads Newco Newco Seek Assess $$$$ Business Leads Funds Partnerships Joint Ventures NIH, Military D.H.S WHO Foreign Grants Contracts Contracts Meet National Needs

60
Example: UTMB, AptaMed, Ciphergen, DowPharma and GE Healthcare
UTMB Research Team CTD/ORT UTMB, AptaMed, Ciphergen, GE Healthcare Discovery Development Pre-Clinical Manufacture “Concept” IP Thioaptamers In biodefense “Confirm” Plan License AptaMed GLP studies Method Dev. Diagnostics Therapeutics Make cGMP Purify Package Regulatory IND test $$$ NationalStockpile Government (DARPA/NIH…)
")
61
Partnership: UTMB, AptaMed, and Ciphergen
Joint $6.3M NIAID Biodefense Proteomics Collaboratory funding Start-up AptaMed in Galveston Incubator New Ciphergen Diagnostics Division in Austin to serve Region New Ciphergen Satellite Facility in Galveston Incubator

62
Conclusions The bioterrorism threat is real The time for action is now
Preparedness can serve as a deterrent UTMB and the Gulf Coast are at the forefront of anti-bioterrorism and emerging diseases research Vision: new biodefense industry is developing - we can lead this effort Catalyst for biotechnology industry and jobs

63
谢谢!

Similar presentations

在中国获批的适应症是高血压 代文 ® (缬沙坦)及唐力 ® (那格列奈)未获批 IGT 适应症 DIO-PM016/01-3/2010 上海交通大学医学院附属瑞金医院心脏科 施仲伟.>")


家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")
,在一 定时间内(至少> 1 月) 药物调整的基础上血压 仍在目标水平之上 或服用 4 种或 4.>")

 卫生部疾病预防控制局 中国疾病预防控制中心.>")







 河南中医学院第一附属医院 杜正光>")



