Download presentation
Presentation is loading. Please wait.

1
Chronic Renal Failure: Pathophysiological and clinical considerations
腎臟科 陳右明醫師 (三)
")
2
OUTLINES I. INTRODUCTION: II. Definition of CKD(CRD) and ESRD
III. Pathophysiology of Chronic Renal Disease IV. Stages of Chronic Renal Disease V. Pathophysiology and Biochemistry of Uremia VI. Clinical and Laboratory Manifestations of Chronic Renal Failure and Uremia 1). Fluid, Electrolyte, and Acid-Base Disorders: 2). Endocrine-Metabolic Disturbances 3). Neuromuscular Disturbances 4). Cardiovascular and Pulmonary Disturbances 5). Dermatologic Disturbances 6). Gastrointestinal Disturbances 7). Hematologic and Immunologic Disturbances VII. Evaluation and Management of Patients with Chronic Renal Disease
. Fluid, Electrolyte, and Acid-Base Disorders: 2). Endocrine-Metabolic Disturbances. 3). Neuromuscular Disturbances. 4). Cardiovascular and Pulmonary Disturbances. 5). Dermatologic Disturbances. 6). Gastrointestinal Disturbances. 7). Hematologic and Immunologic Disturbances. VII. Evaluation and Management of Patients with Chronic Renal Disease.")
3
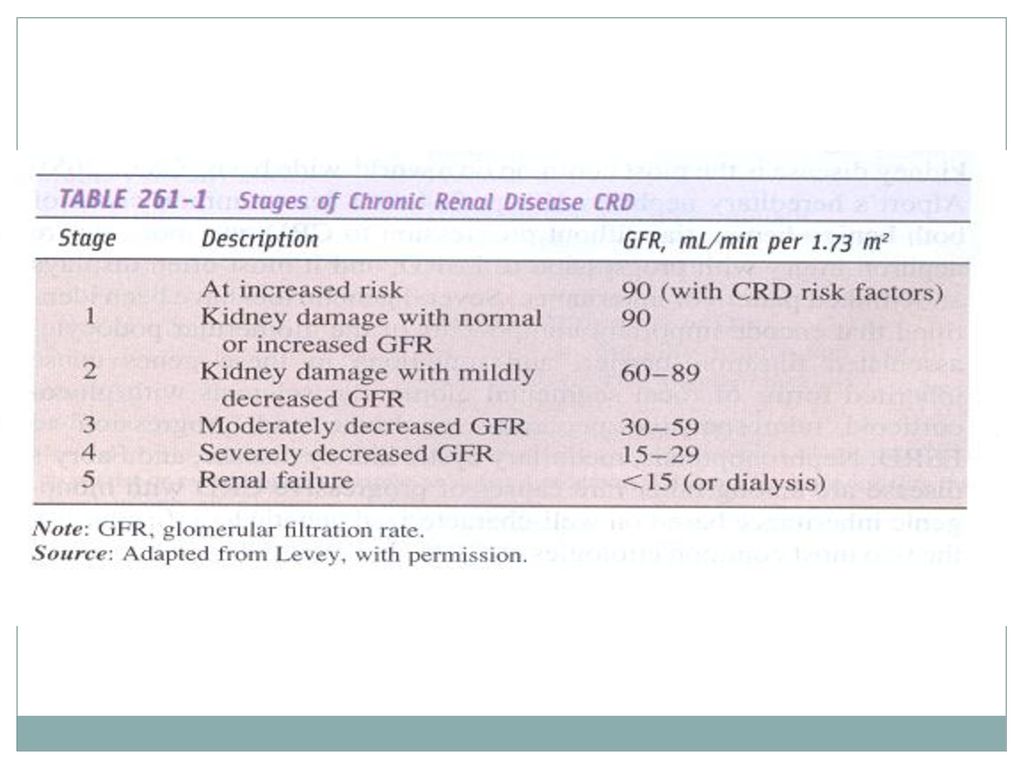
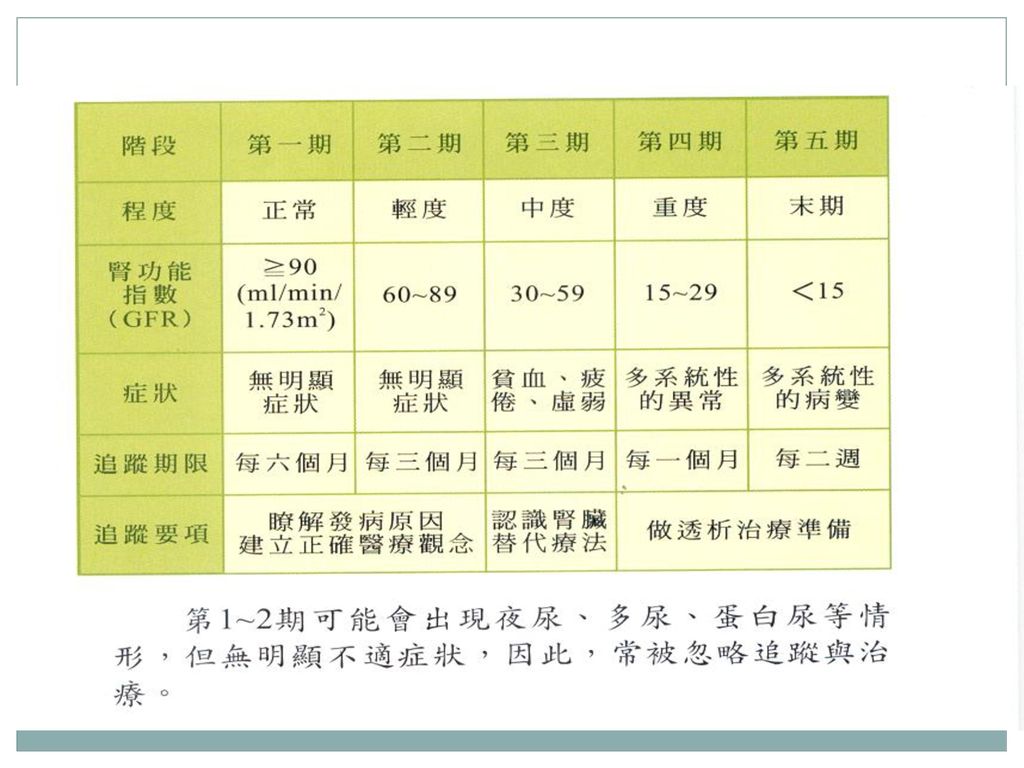
Introduction-1 由於國人飲食習慣與生活習慣不當、不當用藥、馬兜鈴酸、重金屬以及各種有毒物質的影響,加上人口老化、健康照護改善,高齡人口目逐年增加,以致於目前有超過五萬名尿毒症患者接受透析治療。而值得注意的是,目前這些已接受治療的尿毒症患者只是冰山之一角,據臨床經驗與資料顯示,粗估國人目前約有二百萬人已罹患慢性腎臟病。 腎臟病是一個隱形殺手,往往到了末期才產生明顯症狀,因此許多民眾已罹患“慢性腎臟病”卻渾然不知。慢性腎臟病(CKD)分為五期,前二期除了尿液及抽血檢驗外,臨床上並無明顯症狀, 進入慢性腎臟病(CKD)第三、四期的病患,再不注意健康維護,下一階段就是進入第五期的末期腎衰竭需洗腎階段,因此提醒您應該隨時注意自己是否已有「準尿毒症狀態」,所謂「準尿毒症狀態」的臨床表現,簡單來講就是「泡水高貧倦」-泡泡尿(蛋白尿)、水腫、高血壓、貧血與倦怠等五症狀,如果發現有上述五項症狀,而且原因不明,應該立即找腎臟專科醫師,進行詳細的腎臟功能檢查。
分為五期,前二期除了尿液及抽血檢驗外,臨床上並無明顯症狀, 進入慢性腎臟病(CKD)第三、四期的病患,再不注意健康維護,下一階段就是進入第五期的末期腎衰竭需洗腎階段,因此提醒您應該隨時注意自己是否已有「準尿毒症狀態」,所謂「準尿毒症狀態」的臨床表現,簡單來講就是「泡水高貧倦」-泡泡尿(蛋白尿)、水腫、高血壓、貧血與倦怠等五症狀,如果發現有上述五項症狀,而且原因不明,應該立即找腎臟專科醫師,進行詳細的腎臟功能檢查。")
4
Introduction-2 另外,針對洗腎的六大高危險群-糖尿病、高血壓、老年人(>65歲)、蛋白尿、有腎臟病家族史、長期服用藥物者,如果現在還沒有腎臟功能不良的警訊出現,也應該「每三個月檢查尿液,血壓及血肌酐酸等三項」我們簡稱為「護腎檢查三三制」,可以提早發現問題,確保健康。 至於腎臟保健方面,飲食應該三少:少糖、少鹽、少油,同時要三多:多吃蔬菜、纖維、常喝水,生活習慣要四不一沒有:不熬夜、不憋尿、不隨便服來路不明的藥物、不抽菸,同時避免鮪魚肚,因為鮪魚肚代表可能罹患糖尿病,糖尿病又是引發尿毒症的主要原因之一。國內尿毒症發生率居高不下,可能與社會進步、糖尿病人口增加,及國人愛吃藥習慣有關,長期服用止痛藥或服用含有馬兜鈴酸的中藥,都會引發腎病變造成尿毒症。 隨著醫療的進步,新藥的研發,目前已知有藥物可以延緩慢性腎臟病之進程。如果你是六大腎臟病高危險群﹙糖尿病、高血壓、老年人、蛋白尿、有腎臟病家族史、長期服用藥物者﹚的朋友,若是能夠早期發現腎功能的變化,並提早做治療,可以避免步向「洗腎(透析治療)」之路,希望預防勝於治療的腎臟保健觀念,真正落實於我們的生活之中。
」之路,希望預防勝於治療的腎臟保健觀念,真正落實於我們的生活之中。")
5
Definition of CRD (CKD)
Definition: CRD (CKD) is a pathophysiologic process with multiple etiologies, resulting in the inexorable attrition of nephron number and function and frequently leading to end-stage renal disease (ESRD). ESRD: an irreversible loss of endogenous renal function, patient permanently depends upon renal replacement therapy [ dialysis(HD and PD) or transplantation], to avoid life-threatening uremia.
 is a pathophysiologic process with multiple etiologies, resulting in the inexorable attrition of nephron number and function and frequently leading to end-stage renal disease (ESRD). ESRD: an irreversible loss of endogenous renal function, patient permanently depends upon renal replacement therapy [ dialysis(HD and PD) or transplantation], to avoid life-threatening uremia.")
6
Pathophysiology of CRD (CKD)
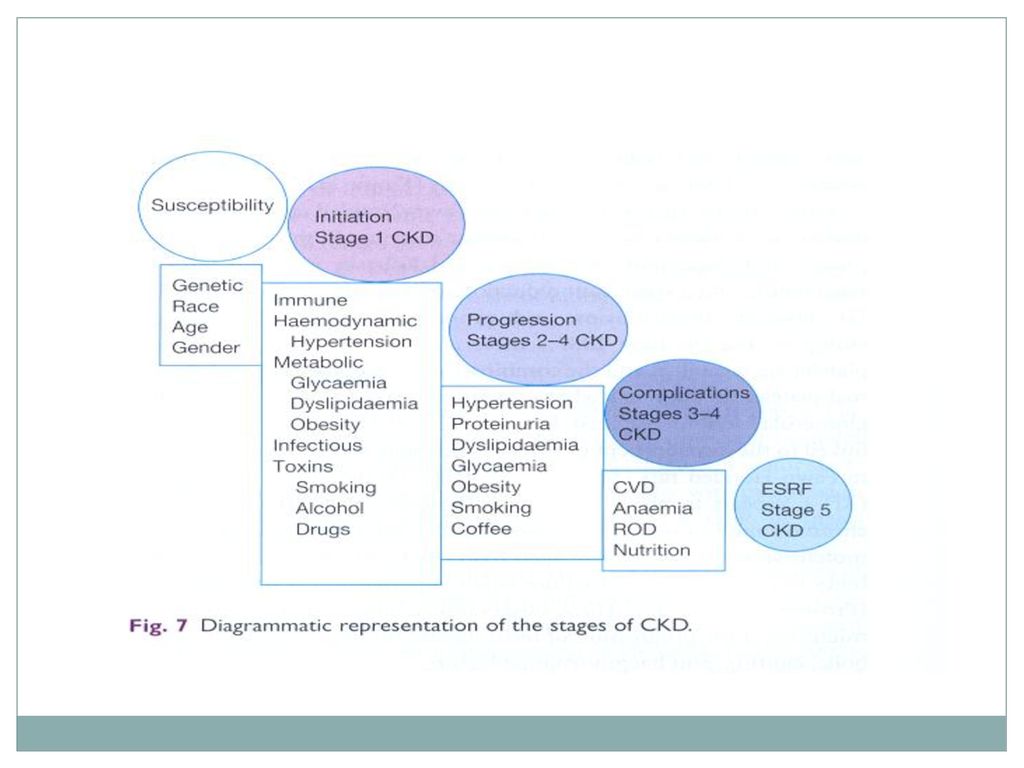
Initiating mechanisms to the underlying etiology long term reduction of renal mass causes structural and functional hypertrophy of surviving nephrons mediated by vasoactive molecules, cytokines, and growth factors initially to adaptive hyperfiltration mediated by in glomerular capillary pressure and flow maladaptive predispose to sclerosis of the remaining viable nephron population

7
Pathophysiology of CRD (CKD)
Increased intra-renal activity of the renin-angiotensin axis plays an important role on the pathophysiology of CRD. Definition of CRD: pathophysiologic process described above last more than 3 months. Factors that increase the risk for CRD: family history of heritable renal disease, hypertension, diabetes, autoimmune disease, older age, past episode of acute renal failure, and current evidence of kidney damage with normal or even increased GFR

8
Pathophysiology of CRD (CKD)
Albuminuria: a key adjunctive tool for monitoring nephron injury and response to therapy in many forms of CRD. Measurement of albumin-to-creatinine ratio in a spot first morning urine sample: Persistence of > 17 mg albumin per gram of creatinine (alb./Cr:>17mg/gm) in adult males and 25 mg albumin per gram of creatinine (alb./Cr:>25mg/gm) in adult females usually signifies chronic renal damage.
 in adult males and 25 mg albumin per gram of creatinine (alb./Cr:>25mg/gm) in adult females usually signifies chronic renal damage.")
11
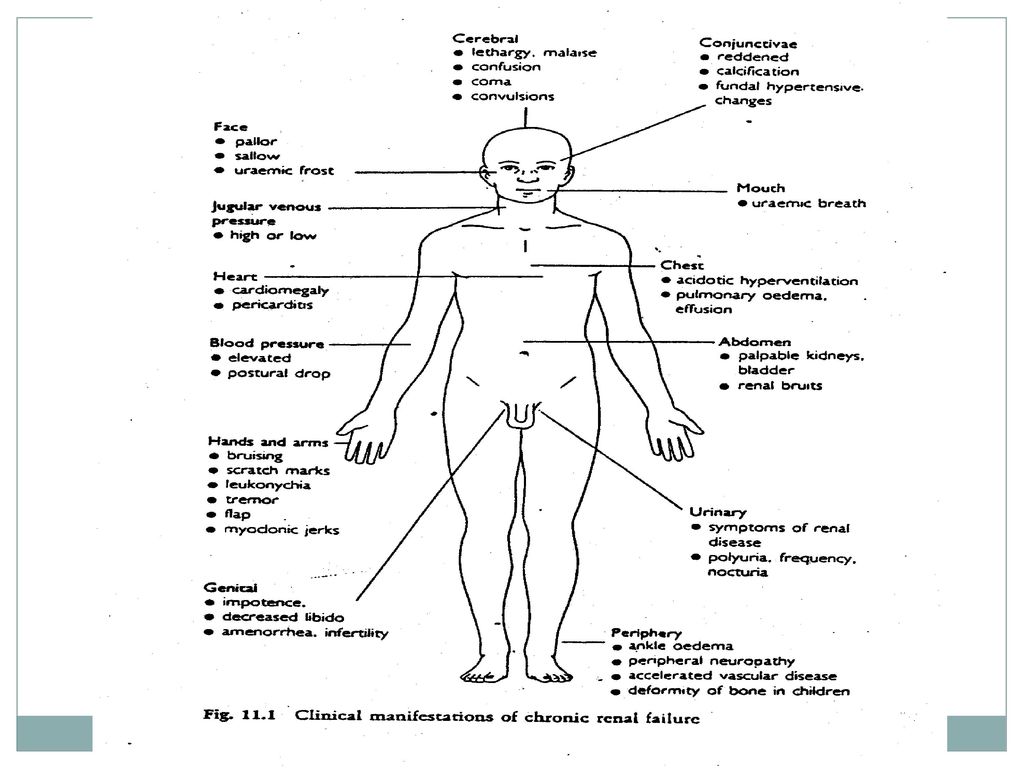
「泡水高屏見」 在初期腎功能喪失不多時,病患本身不會有任何不適,甚至抽血檢驗腎功能(肌酸酐)也不見得有異常,因此早期發現腎臟的疾病可藉由尿液檢查。如果小便有泡沫且久久不能散去,尿液常規證實有蛋白尿時即可診斷腎臟疾病,除了蛋白尿外,常見腎臟疾病的症狀有: 水腫:以下肢、眼瞼水腫為主,甚至全身浮腫也有可能,體重在短時間內急遽增加,小便量可能會減少。 高血壓:百分之三十的早期腎功能衰竭的病人有高血壓的症狀,所以高血壓的病人一定要檢查腎功能及蛋白尿以排除腎性高血壓。 貧血:腎功能衰退至正常的三分之一時,輕度貧血就會出現,若衰退至正常的四分之一時,嚴重貧血即可導致食慾不振、疲倦、無力等症狀。 疲倦:大多數疲倦的病人都以為是肝臟機能不佳而求診肝膽腸胃科,經過肝臟超音波、胃鏡、大腸鏡、抽血檢驗肝指數均正常,最後才診斷是慢性腎衰竭、貧血而轉診至腎臟內科醫師。 總之,慢性腎衰竭的症狀千奇百怪,但民眾可以記住一口訣:泡(蛋白尿)、水(水腫)、高(高血壓)、屏(貧血)、見(倦,疲倦),亦即「泡水高屏見」,就可以掌握腎臟是否出了問題,以期盡早診斷和治療。
、水(水腫)、高(高血壓)、屏(貧血)、見(倦,疲倦),亦即「泡水高屏見」,就可以掌握腎臟是否出了問題,以期盡早診斷和治療。")
14
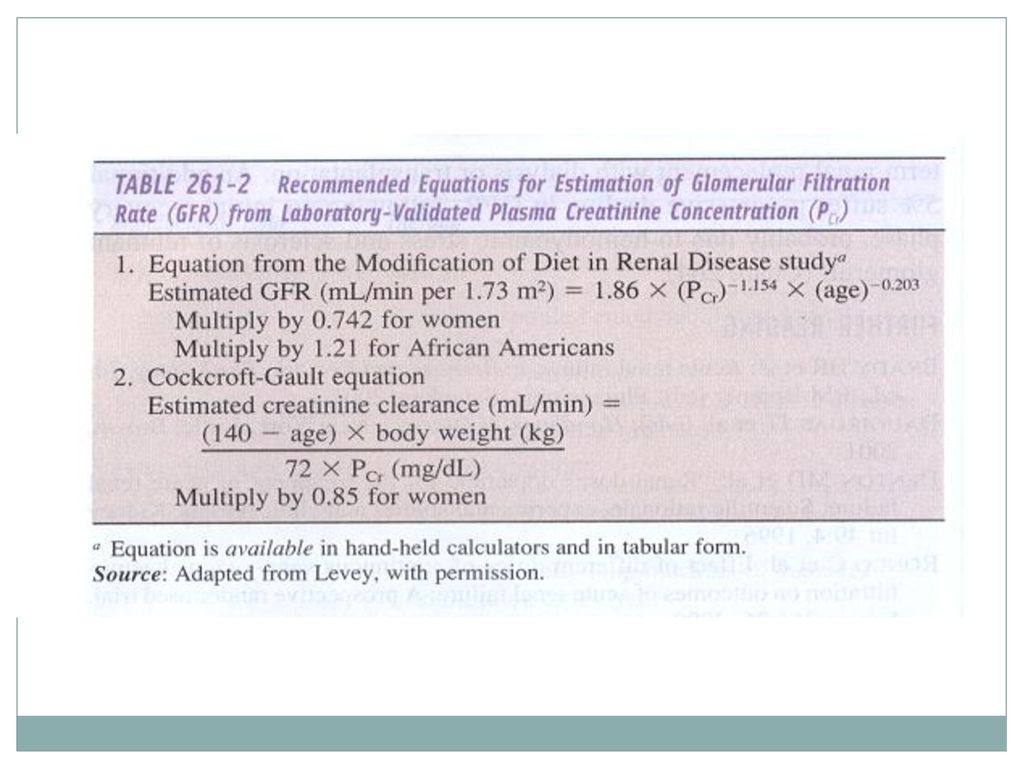
CCr = Cr (U) x urine amount(one day)
1440 x Cr (P)
")
15
Pathophysiology of CRD (CKD)
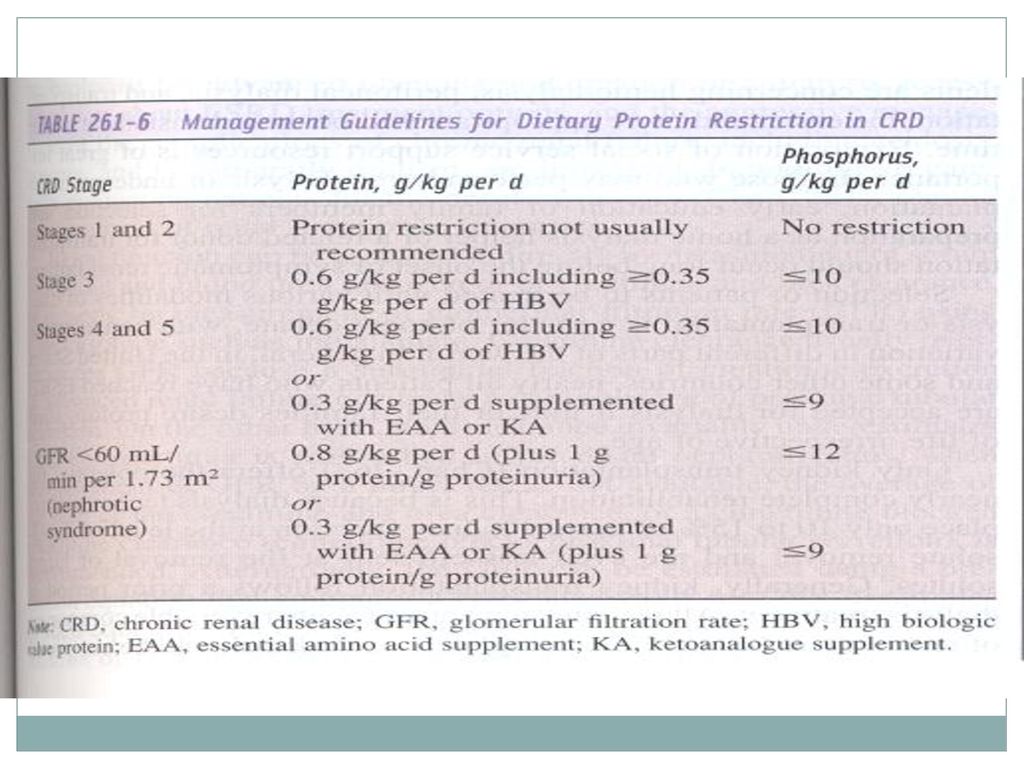
Stages 3 and 4 of CRD: anemia, loss of energy, decreasing appetite, disturbances in nutritional status, abnormalities in calcium and phosphate metabolism accompanied by metabolic bone disease, abnormalities in sodium, water, potassium, and acid-base homeostasis. Stage 5(GFR<15 mL/min): severe disturbances in their daily activities, sense of well-being, nutritional status, water and electrolyte homeostatis
: severe disturbances in their daily activities, sense of well-being, nutritional status, water and electrolyte homeostatis.")
16
Pathophysiology and Biochemistry of Uremia
Azotemia: retention of nitrogenous waste products Uremia: more advanced stages of CRD when the complex, multiorgan system derangements become clinically manifest. Middle molecules: a molecular mass of 500~12000 Da; are believed to contribute to mortality and morbidity in uremic subjects.

17
Pathophysiology and Biochemistry of Uremia
Uremic syndrome: two sets of abnormalities: The accumulation of products of protein metabolism. The loss of other renal functions, such as fluid and electrolyte homeostasis and hormonal abnormalities.

18
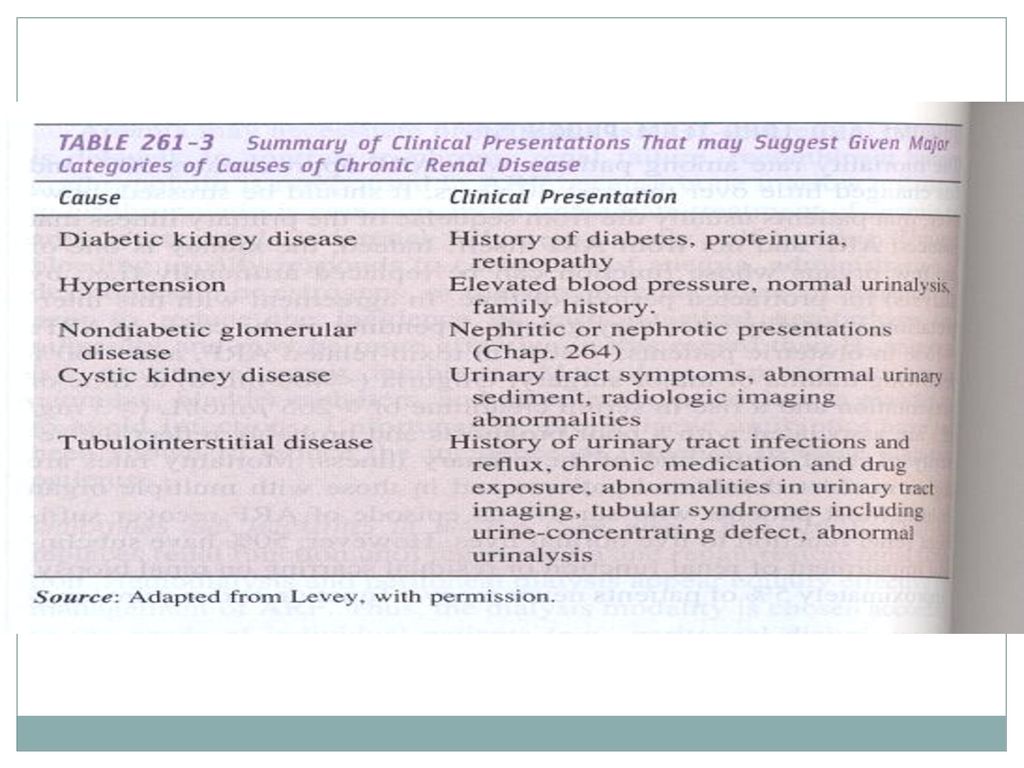
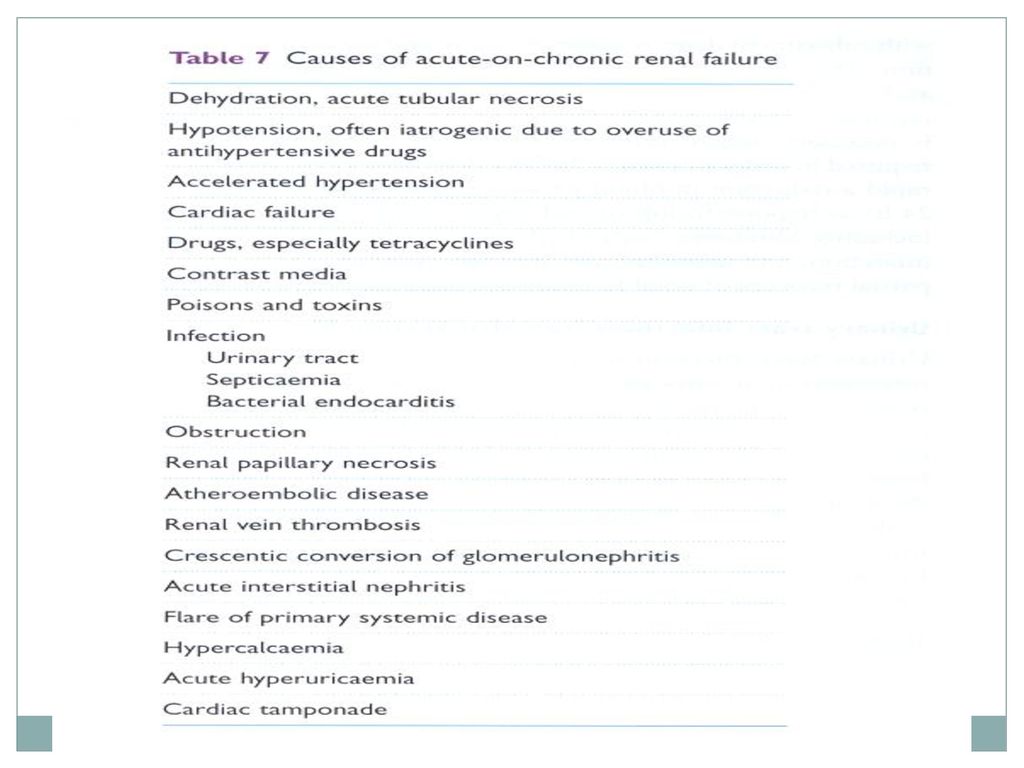
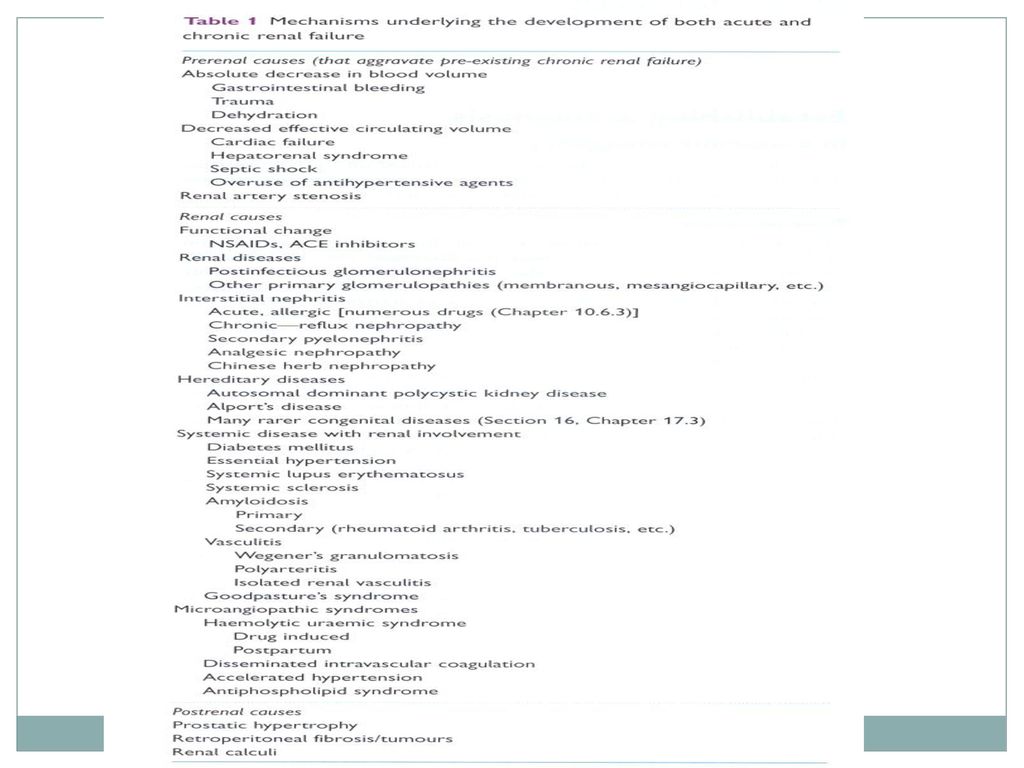
Causes of chronic kidney diseases

22
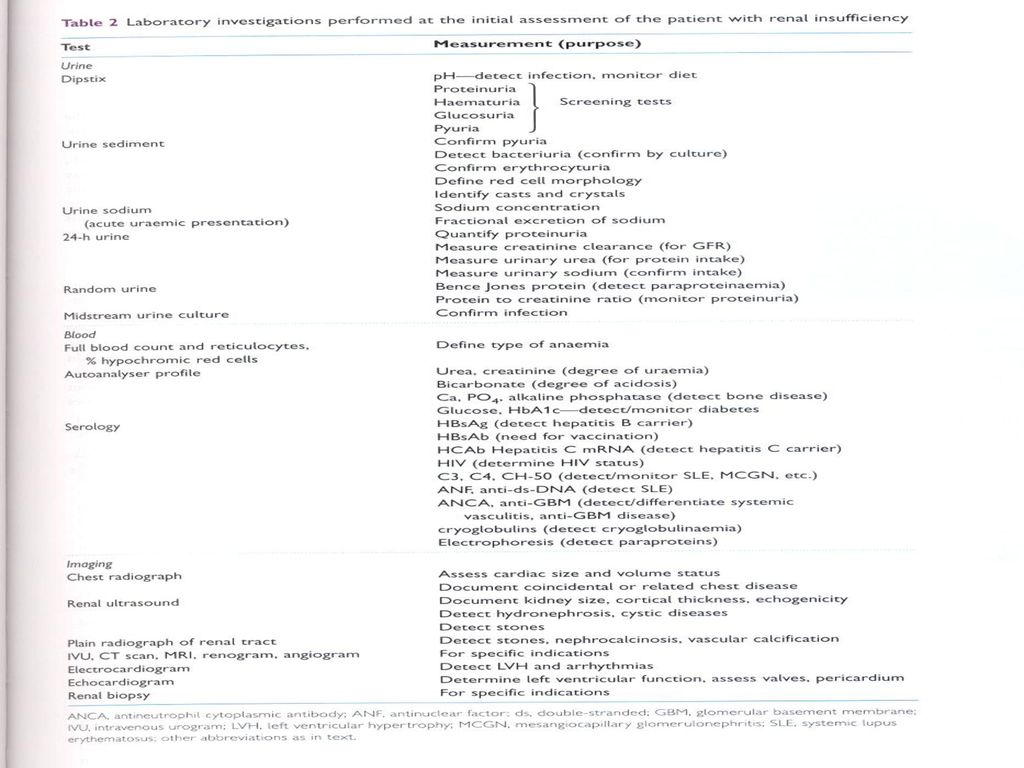
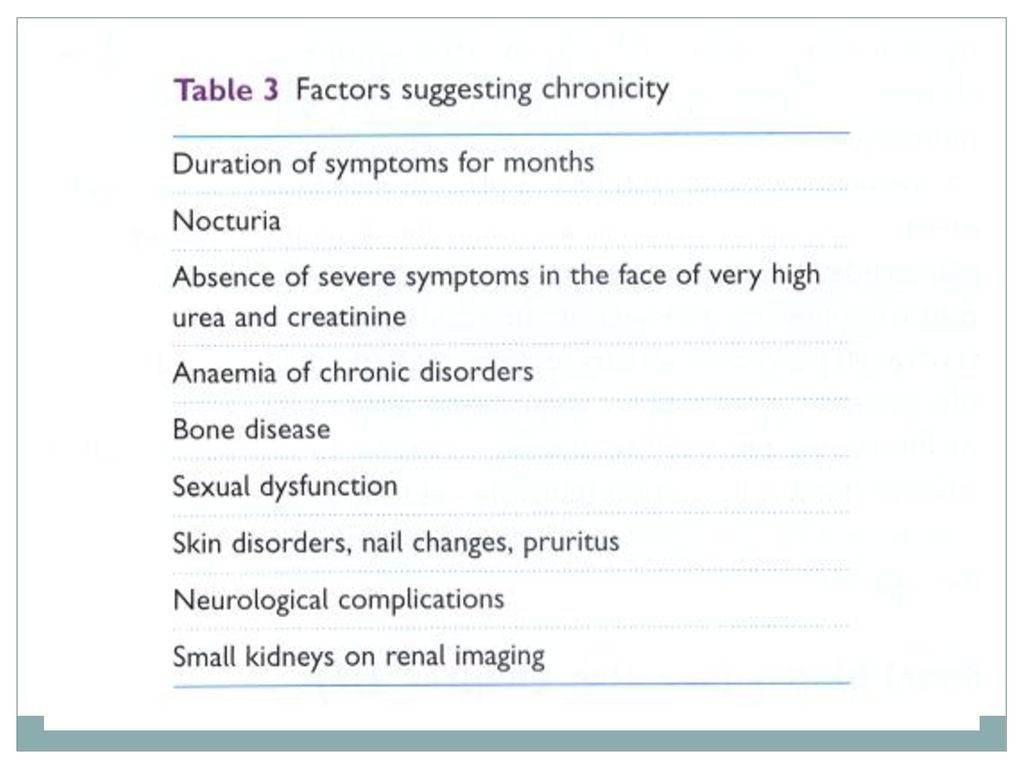
Laboratory investigations of CKD

24
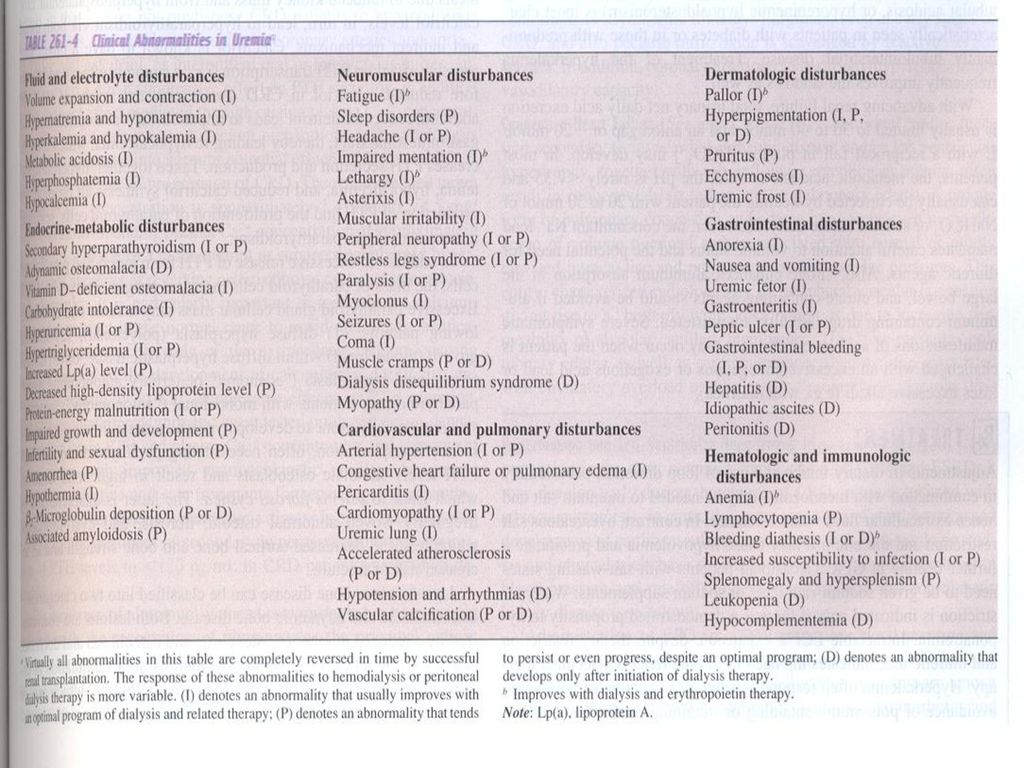
Clinical and Laboratory Manifestations of CRF and Uremia
Fluid, Electrolyte, and Acid-Base disorders: Endocrine-metabolic disturbances: Neuromuscular disturbances: Cardiovascular and pulmonary disturbances: Dermatologic disturbances: Gastrointestinal disturbances: Hematologic and Immunologic disturbances:

27
Fluid, Electrolyte, and Acid-Base disorders:
Volume expansion and contraction Hypernatremia and hyponatremia Hyperkalemia and hypokalemia Metabolic acidosis Hyperphosphatemia Hypocalcemia

28
Hyperkalemia Clinical situations cause hyperkalemia: Constipation
Augmented dietary intake Protein catabolism Hemolysis Hemorrhage Transfusion of stored red blood cells Metabolic acidosis Following the exposure to a variety of medications that inhibit K+ entry into cells or K+ secretion in the distal nephron(beta-blockers, ACEI, ARB, NSAID, K+-sparing diuretics, etc)
")
29
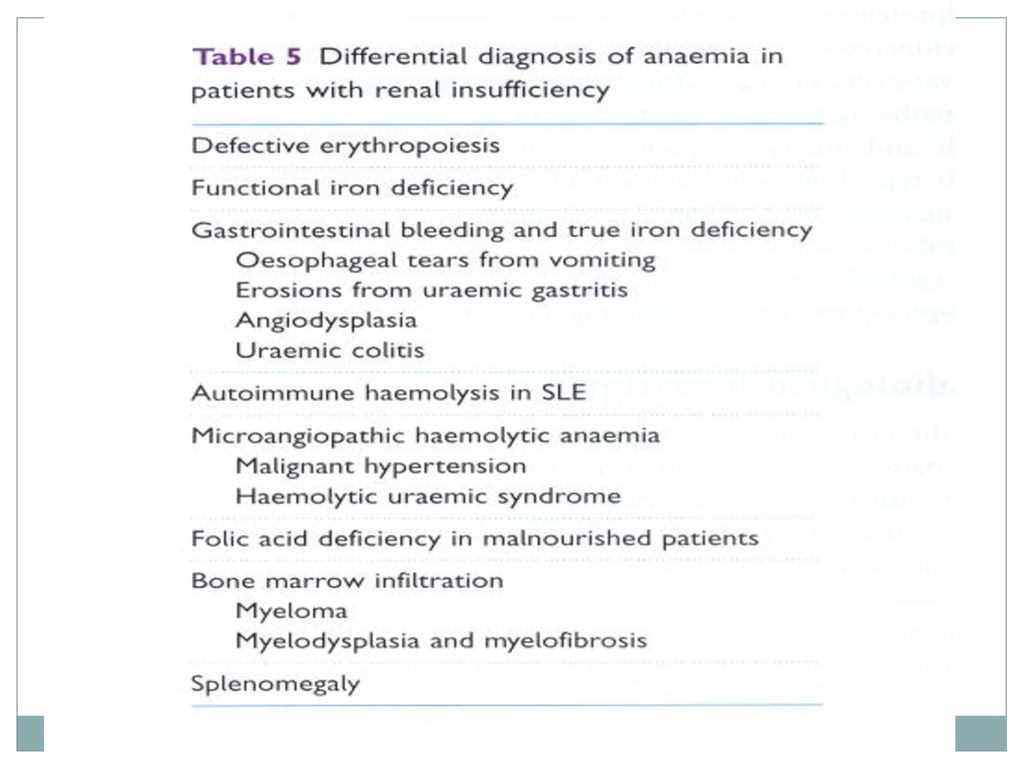
Hematologic and Immunologic disturbances:
Anemia Lymphocytopenia Bleeding diathesis Increased susceptibility to infection Splenomegaly and hypersplenism Leukopenia Hypocomplementemia

32
Evaluation of Patients with CRD
Initial approach: History and Physical Examination Laboratory Investigations Imaging Studies Renal Biopsy Establishing the Diagnosis and Etiology of CRD

34
Management of Patients with CRD

36
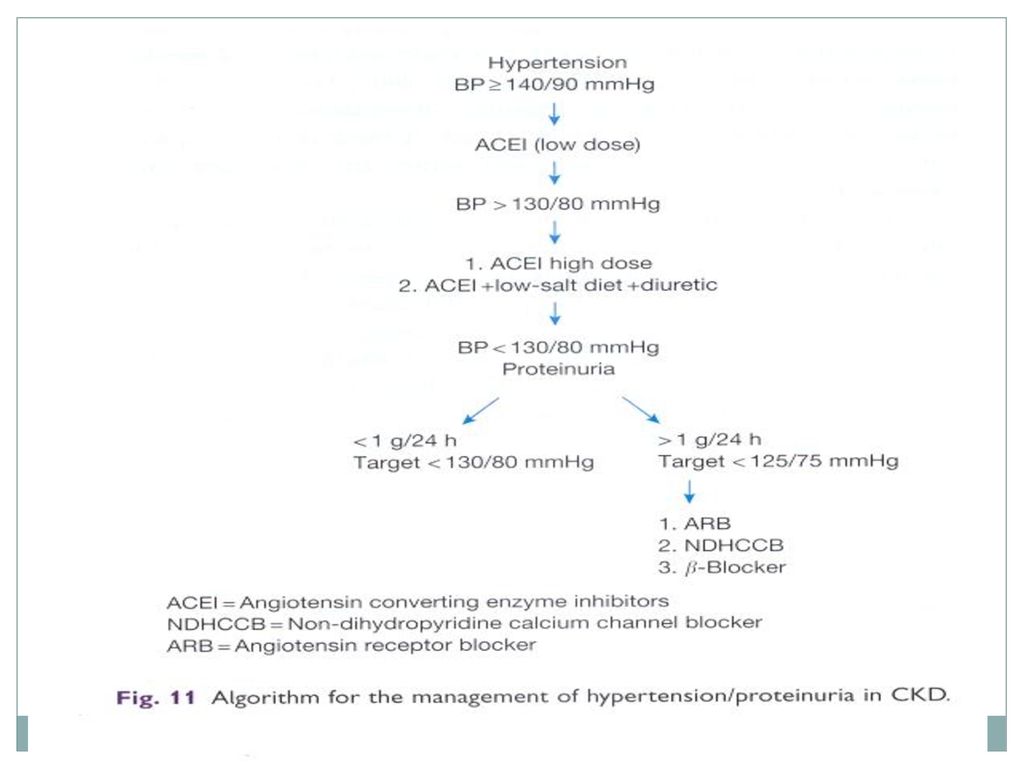
Slowing the progression of CKD

37
Slowing the progression of CKD
No smoking, no alcohol Use of ACEI, ARB etc On low salt, low protein diet Avoid nephrotoxic agents and unnecissary drugs Obesity reduce body weight to IBW Control BP Control sugar Control dyslipidemia Pentoxifyllin use[slow down(prevent) renal fibrosis] Ketosteril use(reduce urea production, reduce urea to kidney burden, improve nutrition status, and improve immunity) Kremezin(spherical active charcoal)
 renal fibrosis] Ketosteril use(reduce urea production, reduce urea to kidney burden, improve nutrition status, and improve immunity) Kremezin(spherical active charcoal)")
38
Kremezin® Spherical Adsorptive Carbon for Chronic Kidney Disease

39
Difference between Kremezin® and Activated Charcoal

40
External Observation of GI-tract (服用後的腸胃道表面)
Conventional diet (普通食物) Kremezin® 5 % diet Medicinal charcoal 5 % diet (藥用活性碳)
41
Decrease of IS level by AST-120
Indoxyl Sulfate N H OH OSO3H CH2CHCOOH Indoxyl Liver Kidney Tryptophan NH2 Indole AST-120 GI-tract Excreted with Feces Indoxyl sulfate(indican, MWt:213) is synthesized in the liver from indole absorbed from the intestines. Indole is produced in the large intestines from dietary-derived tryptophane by intestinal bacteria such as E.coli. Indoxyl sulfate is normally excreted into the urine at an amount of approximately 60mg/day primarily by proximal tubular secretion through the organic anion secretory pathways, and partly by glomerular filtration.However, indoxyl sulfate markedly accumulates in the uremic serum due to its reduced renal clearance. An oral adsorbent,AST-120, adsorbs indole, and the other indolic and phenolic metabolites in the intestines, and stimulates their excretion into feces, thus suppressing indole absorption from the intestines.Consequently, the oral sorbent reduces the production of indoxyl sulfate in the liver accompanied by a reduction in the serum and urine levels of indoxyl sulfate. Niwa,T.et al Kidney Int 52 Suppl.62 :S23, 1997
 is synthesized in the liver from indole absorbed from the intestines. Indole is produced in the large intestines from dietary-derived tryptophane by intestinal bacteria such as E.coli. Indoxyl sulfate is normally excreted into the urine at an amount of approximately 60mg/day primarily by proximal tubular secretion through the organic anion secretory pathways, and partly by glomerular filtration.However, indoxyl sulfate markedly accumulates in the uremic serum due to its reduced renal clearance. An oral adsorbent,AST-120, adsorbs indole, and the other indolic and phenolic metabolites in the intestines, and stimulates their excretion into feces, thus suppressing indole absorption from the intestines.Consequently, the oral sorbent reduces the production of indoxyl sulfate in the liver accompanied by a reduction in the serum and urine levels of indoxyl sulfate. Niwa,T.et al Kidney Int 52 Suppl.62 :S23,")
42
Main Know Uremic Retention Solutes
Kremezin can adsorb uremic toxins that has molecular weight ranged from 100 to 1000 among these retention solutes. Especially, the ability of adsorbing a water-soluble, ionic compounds is enhanced. Meanwhile, Kremeizn can not adsorb compounds with high molecule, for example, hormone, digestive enzyme, etc. Vanholder R et al., Kidney Int (2003) 63:S6-S10
 63:S6-S10.")
43
Effect of Indoxyl Sulfate on Serum Creatinine in Uremic Rats
4 (mg/dL) 3 2 1 6 (weeks) Mean+SE *p<0.05 as compared with control Serum Creatinine Indoxyl sulfate administered: n=10 50mg/kg twice/week p.o. Control: n=10 * Duration of Administration (5/6 nephrectomized rats) Indoxyl sulfate has been characterized as one of the uremic toxins that appear to be causally related to the deterioration of renal function. Administration of IS or indole, a precursor of IS, to nephrectomized rats resulted in decreased renal function and increased glomerular sclerosis in the remnant kidney (Niwa et al. 1994). Furthermore, IS stimulated genes related to renal fibrosis, such as TGF-β1, TIMP-1, and pro-α1(I) collagen (Miyazaki et al. 1997). Niwa, T. et al: J Lab Clin Med, 124(1), p96,1994
 (weeks) Mean+SE. *p<0.05 as compared with control. Serum Creatinine. Indoxyl sulfate administered: n=10 50mg/kg twice/week p.o. Control: n=10. * Duration of Administration. (5/6 nephrectomized rats) Indoxyl sulfate has been characterized as one of the uremic toxins that appear to be causally related to the deterioration of renal function. Administration of IS or indole, a precursor of IS, to nephrectomized rats resulted in decreased renal function and increased glomerular sclerosis in the remnant kidney (Niwa et al. 1994). Furthermore, IS stimulated genes related to renal fibrosis, such as TGF-β1, TIMP-1, and pro-α1(I) collagen (Miyazaki et al. 1997). Niwa, T. et al: J Lab Clin Med, 124(1), p96,1994.")
44
Evaluation Methods for Japanese Phase III
1/sCr Slope (Phase III) 1/sCr Slope sCr HD before after Time Initiation of AST-120 Administration sCr Conc. with AST-120 without AST-120 before after Time Reciprocal sCr hyperbolic curve 10 1/10 As the evaluation methods we used the slope of reciprocal serum Cr and survival analysis. The changes in renal function were evaluated by plotting the reciprocal of the serum-creatinine level versus time, as reported by Mitch et al(Lancet 1976;2:1326).The slope of the regression line is substituted as the progression speed of renal failure. When plotting the serum Cr value versus time, it shows hyperbolical curve. Meanwhile, when plotting the reciprocal of the serum-creatinine level versus time , it shows linear curve. Progression of renal failure is considered to be rapid when the slope is negative and steep. If both slopes of regression lines are different , in other words, the slope becomes less steep, we can confirm an attenuation after Kremezin administration. So,we can acknowledge the progression is suppressed by Kremezin. Also, another evaluation is survival analysis by Kaplan-Meier Method for No-dialysis Rate. Koshikawa S. at.el. Kidney and Dialysis 23 : , 1987 Koide K. at.el. Clinical Evaluation 15 : ,1987
 1/sCr Slope. sCr. HD. before 0 after Time Initiation of AST-120 Administration. sCr Conc. with AST-120. without AST-120. before 0 after Time. Reciprocal sCr. hyperbolic curve /10. As the evaluation methods we used the slope of reciprocal serum Cr and survival analysis. The changes in renal function were evaluated by plotting the reciprocal of the serum-creatinine level versus time, as reported by Mitch et al(Lancet 1976;2:1326).The slope of the regression line is substituted as the progression speed of renal failure. When plotting the serum Cr value versus time, it shows hyperbolical curve. Meanwhile, when plotting the reciprocal of the serum-creatinine level versus time , it shows linear curve. Progression of renal failure is considered to be rapid when the slope is negative and steep. If both slopes of regression lines are different , in other words, the slope becomes less steep, we can confirm an attenuation after Kremezin administration. So,we can acknowledge the progression is suppressed by Kremezin. Also, another evaluation is survival analysis by Kaplan-Meier Method for No-dialysis Rate. Koshikawa S. at.el. Kidney and Dialysis 23 : , Koide K. at.el. Clinical Evaluation 15 : ,1987.")
46
Case # 1 秦XX A case of 70 y/o female p’t (Non-DM) Underlying diseases:
Obstructive uropathy on D-J chronically Chronic glomerulonephritis with unspecified pathological lesion in kidney. Chronic renal failure Iron deficiency anemia, unspedified Unspecified obstructive defect of renal pelvis and ureter Acute cystitis Anemia in end-stage renal disease Internal hemorrhoids without mention of complication Hemorrhage of gastrointestinal tract, unspecified 46 46

47
Kremezin 1 pc(2g)*tid. since May 1, 2008 Scr Kremezin 47
*tid. since May 1, 2008 Scr Kremezin 47")
49
Managing Other Complications of Chronic Renal Failure:
Uremic Symptomatology Medication Dose Adjustment Preparation for Renal Replacement Therapy Patient Education and Adjustment

50
零極限 夏威夷傳統療法: 四句話 「我愛你,對不起,請原諒我,謝謝你。」 願「愛」、「懺悔」與「感恩」帶來零極限的最高境界!!!

Similar presentations

 Regulate fluid, electrolyte Acid-base balance 調整血壓:經由腎素體系進行調節。>")


. 病因( Etiologe ) Primery Glomerular Diseases (60%) Hypertensive Nephrosclerosis Diabetic Glomerulosclerosis >")
 病理生理学系 Department of Pathophysiology 高远生.>")


,在一 定时间内(至少> 1 月) 药物调整的基础上血压 仍在目标水平之上 或服用 4 种或 4.>")



.>")


 河南中医学院第一附属医院 杜正光>")

>")

