Download presentation
Presentation is loading. Please wait.

1
肝癌治療新發展 李傑輝醫生 顧問醫生 名譽臨床副教授 香港中文大學肝膽胰外科 威爾斯親王醫院

2
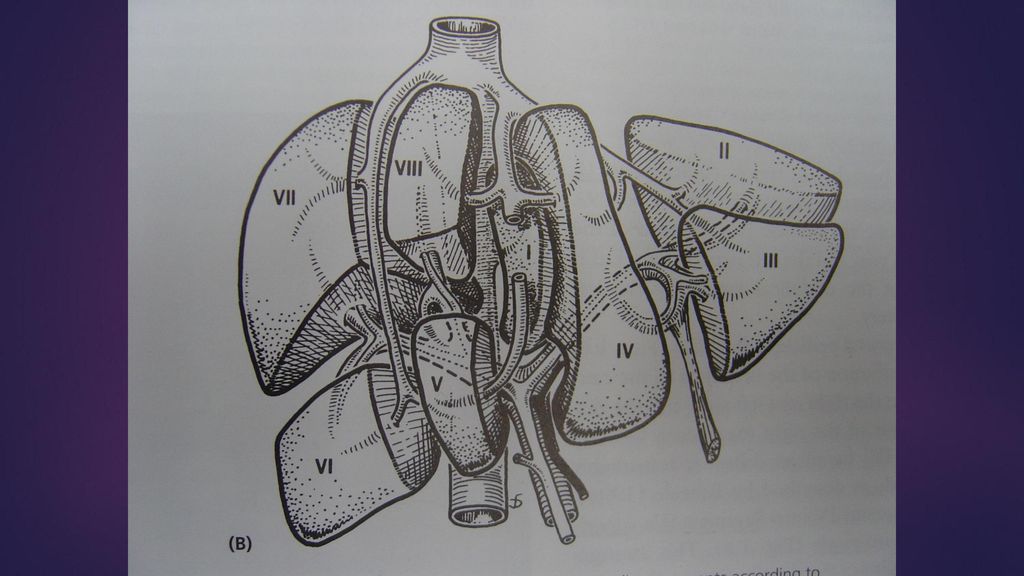
肝臟 位於右上腹 是人體最大的器官 它分為左葉和右葉 右葉的體積比左葉大 其主要功能是生產和儲備能量 肝臟可將食物中的碳水化合物(糖)和
脂肪轉化成能量,以應付身體的各種活動 肝臟同時會將糖份、維他命等養分儲存起來,以備不時之需。

3
肝癌 肝癌分為兩大類: 原發性肝癌 (肝細胞肝癌) 肝硬化是肝癌的主要高 危因素之一。 長期酗酒, 肝炎病毒 會增加肝硬化以至肝癌的風險
由於本港十分之一人口是乙型肝炎帶菌者,慢性乙型肝炎成為肝癌最常見的高危因素。
5
肝癌 轉移性肝癌 轉移性肝癌是由身體 其他部位擴散到肝臟 的腫瘤 幾乎所有部位的原位癌都有可能擴散到肝臟
可能性最高的是大腸、胰臟、胃、肺和乳房的腫瘤
6
什麼因素影響肝癌的治療 疾病分期 肝臟機能 總體健康狀況

7
肝細胞癌分期 肝外轉移:肺,骨,腹膜,腎上腺 主要血管侵潤:門靜脈,肝靜脈,下腔靜脈 侵入鄰近器官:橫隔膜,右腎上腺,胃,膽囊,結腸
腫瘤數量 腫瘤大小 腫瘤位置

8
肝臟機能 有或沒有肝硬化 門靜脈高壓症 肝硬化分期: 血小板下降 膽紅素 食道或胃靜脈曲張 血蛋白 彭脹 凝血指數 肝功能 腹水 質量 腦病
體積

9
病人的一般健康狀況 年齡 慢性疾病:心臟病,慢性肺病,糖尿病, 高血壓,腎功能衰竭,腦血管病 日常活動能力 吸煙史

10
治療肝細胞癌 根治性 肝臟部份切除術 肝臟移植(活肝/ 屍肝) 消融術治療 紓緩性 經肝臟動脈栓塞術 化學治療 症狀性
 消融術治療 紓緩性 經肝臟動脈栓塞術 化學治療 症狀性")
11
早期 中至晚期 肝臟切除 肝臟移植 局部燒融術 非手術治療 經動脈化療栓塞法 化療、標靶治療 紓緩治療

12
肝臟切除手術 外科手術是治療原發性肝癌的主要方法,這種手術稱為肝臟切除手術。
肝臟切除手術是把一部分的肝臟切除,但切除多少則視乎腫瘤的大小位置及有否入侵肝臟的血管等因素。 肝臟有自我修復的能力,一般來說,高達百分之六十至七十的肝臟是可以被切除而不會有後遺症的。 但是如果肝臟已經有肝硬化的病變切除的風險便相對提高。
13
肝臟切除術 重大手術 問題 :失血,肝衰竭,膽溜,感染等併發症 死亡率 < 5% 併發症發生率 :可高至 40%
5年存活率 :30-50% 腫瘤復發是常見的: 5年內可高至50%

14
腹腔鏡肝切除術 只可在個別適應症 小腫瘤 <5厘米 腫瘤位置 :在肝的 2,3,4b,5,6段 腫瘤沒有侵入主血管

16
Advantages of laparoscopic liver resection over open liver resection 腹腔鏡肝切除相對於剖腹肝切除的好處
Jan 2003 – Dec 2006 25 patients underwent laparoscopic liver resection腹腔鏡 肝切除were compared with 25 patients who underwent open hepatectomy剖腹肝切除in a pair-matched design ↓blood loss, ↓hospital stay, ↓requirement of analgesics止痛 藥, earlier return to oral diet進食 Lee KF et al. Hong Kong Med J 2007;13:

17
Laparoscopic liver resection for liver cancer 腹腔鏡肝切除用於肝癌
June March 2010 33 patients underwent laparoscopic hepatectomy for liver cancer During the same period, 50 patients with liver cancer who underwent open liver resection were recruited matching with tumor size, site and type of resection for comparison

18
Overall survival (Kalpan-Meier) 整體生存率
Survival Proportion LH OH 1 year survival 86.9% 98.0% 3 year survival 81.8% 80.6% 5 year survival 76.0% 76.1% Log rank test: P-value = (No significant difference)
")
19
Disease free survival (Kalpan-Meier) 無病生存率
Survival Proportion LH OH 1 year survival 78.8% 69.2% 3 year survival 51.0% 55.9% 5 year survival 45.3% Log rank test: P-value = (No significant difference)
")
20
Robotic liver resection 機械人肝臟切除
Advantages of robot: 3 dimensional image with magnification, instruments with 7 degrees of freedom, better ergonomics人體功效學for operating surgeon Limitation and drawbacks: lack of tactile sense觸覺, narrow operative field, lack of appropriate instruments, time for docking and undocking of machine, cost

21
肝臟移植 同時切除肝臟腫瘤及已病變的肝 缺點:高風險手術,長期服用抗排斥藥 問題:屍肝短缺和腫瘤在等候期增大及擴散 5年生存率達50-60%
復發率少於肝臟切除術 米蘭準則 (Milan criteria) 單一腫瘤:<5厘米 多發性腫瘤:數量<3 及每個腫瘤 <3厘米
 單一腫瘤:<5厘米. 多發性腫瘤:數量<3 及每個腫瘤 <3厘米.")
22
腫瘤局部消融術 無水酒精 激光 冷凍治療 高強度聚焦超聲波 射頻消融 微波消融 納米刀

23
局部消融療法 局部痲醉下的經皮治療 全身痲醉下腹腔鏡或剖腹 適合細腫瘤 < 5厘米,最理想 <3厘米 腫瘤數目少於3
不可以太近主要血管和主要膽管 在經皮的治療方式,不可以太近其他器 官或橫隔膜

24
局部消融術治療 死亡率<1% 併發症發生率<10% 在細小的腫瘤生存率可接近肝細胞癌切 除,但復發率較高

25
RF Heating Mechanism 射頻消融
Uses radiowaves at ~ 480 kHz. Heating mechanism: ionic agitation. Electrode A Electric field V E field RF probe = electrode B + + + + patient Tissue RF: alternating electric field (~ 400 kHz) Requires two electrodes: first electrode is the applicator tip, the other reference electrode a large area conductive pad placed on the patient’s skin. The RF generator produces a RF voltage between the two electrodes, establishing electric field lines within the patient's body between the two electrodes. The electric field pattern is governed essentially by electrostatic equations. RF current causes molecules and ions to oscillate to the electric field. Molecular friction between molecules produces heat. The mechanism of RF heating is frictional or resistive energy losses associated with this ionic current. RF heating is influenced principally by the dielectric properties of the tissue Applicator designs: Conventional monopolar electrodes Umbrella RF electrodes Multiple probes tissue ions that are attempting to follow the direction of the current get agitated. Due to natural high resistivity in the living tissue, ionic agitation produces frictional heat at the immediate vicinity of electrodes. Ion movement Efficiency limited by tissue conductivity. Organs differ greatly in conductivity at RF frequencies. 25
 Requires two electrodes: first electrode is the applicator tip, the other reference electrode a large area conductive pad placed on the patient’s skin. The RF generator produces a RF voltage between the two electrodes, establishing electric field lines within the patient s body between the two electrodes. The electric field pattern is governed essentially by electrostatic equations. RF current causes molecules and ions to oscillate to the electric field. Molecular friction between molecules produces heat. The mechanism of RF heating is frictional or resistive energy losses associated with this ionic current. RF heating is influenced principally by the dielectric properties of the tissue. Applicator designs: Conventional monopolar electrodes. Umbrella RF electrodes. Multiple probes. tissue ions that are attempting to follow the direction of the current get agitated. Due to natural high resistivity in the living tissue, ionic agitation produces frictional heat at the immediate vicinity of electrodes. Ion movement. Efficiency limited by tissue conductivity. Organs differ greatly in conductivity at RF frequencies. 25.")
26
Experience of RFA in PWH 射頻消融
May Feb 2006 79 patients with 110 liver tumors underwent percutaneous經皮(46.8%), laparoscopic腹腔鏡(8.9%) or open剖腹(44.3%) RFA Median tumor size: 2.4cm (0.5-8) Mortality: 0% Morbidity: 6.3% Complete ablation腫瘤完全消毀: 82.3% Intrahepatic recurrence肝內腫瘤復發: 52.3% with a mean FU 16 months (range ) Wong J et al. Asian J Surgery 2009;32:13-20
, laparoscopic腹腔鏡(8.9%) or open剖腹(44.3%) RFA. Median tumor size: 2.4cm (0.5-8) Mortality: 0% Morbidity: 6.3% Complete ablation腫瘤完全消毀: 82.3% Intrahepatic recurrence肝內腫瘤復發: 52.3% with a mean FU 16 months (range ) Wong J et al. Asian J Surgery 2009;32:")
27
MW Heating Mechanism 微波消融
Effective and consistent heating in all soft tissue organs. Faster, bigger, more repeatable ablations than RF. Heating mechanism: coupling to water dipole. + + - H H O E field O + H H - + + Dipole interaction: dipoles (water molecule) oscillate in electric field 27
 oscillate in electric field. 27.")
28
Experience of MWA in PWH 微波消融
March October 2010 24 patients with liver cancer received either laparoscopic腹腔鏡(N=15) or open剖腹MVA (N=9) Median tumor size: 3.5cm (0.6-6cm) Mortality: 0% Morbidity: 16.7% Complete ablation腫瘤完全消毀: 98.5% Intrahepatic recurrence肝內腫瘤復發: 20.8% with a median FU of 7.1 months ( months)
 or open剖腹MVA (N=9) Median tumor size: 3.5cm (0.6-6cm) Mortality: 0% Morbidity: 16.7% Complete ablation腫瘤完全消毀: 98.5% Intrahepatic recurrence肝內腫瘤復發: 20.8% with a median FU of 7.1 months ( months)")
29
IRE DEVICE

30
Percutaneous procedure
USG/CT scan guidance CT measurements
31
總結 現代的肝癌治療有賴不同專科的會診以 達到最佳的治療方案,包括肝膽外科、X 光介入科、腫瘤科以及肝內科
方案可能結合不同治療方式,如手術切除 加射頻消融 手術傾向微創化 治療方案個人化

Similar presentations



家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")


: 特定吸收率 ( 人體組織吸收行動電話或其他無 線裝置所發出之電磁輻射的速率.>")













