Download presentation
Presentation is loading. Please wait.

1
慢性病毒性肝炎治疗—— 现状与展望 复旦大学附属华山医院 邬祥惠
慢性病毒性肝炎治疗—— 现状与展望 复旦大学附属华山医院 邬祥惠 Slide 2. HCV 感染:流行病学与自然病程

2
乙型肝炎研究的大事记 1965 Blumberg等发现“澳大利亚”抗原 1970 Dane等发现HBV的病毒颗粒
Kaplan发现HBV病毒颗粒中含DNA聚合酶 Summers用限制性内切酶技术阐明分子结构 制备血源性乙肝疫苗、HBIG 干扰素用于治疗慢性乙型肝炎 Rizzetto小组肝细胞核内发现抗原 发展了嗜肝病毒科 Summers阐明了HBV的复制过程 重组乙肝疫苗问世 开始拉米夫定临床试验 拉米夫定上市 PEG -干扰素用于慢性乙肝的治疗

4
HBV分子病毒学 嗜肝DNA病毒科,基因长3.2kb 4个开放读码框架:Pre-S/S、Polymerase Precore/core、X
Core promoter和Precore区变异 X蛋白与肝癌的发生有关 cccDNA是HBV复制的模板 大多数抗病毒药物对cccDNA的作用小或无作用

5
病毒清除与血清转换 慢性HBV感染可以分为三个连续性的阶段 在免疫清除期,可能最终出现乙肝病毒e抗原(HBeAg)血清转换
(I) 免疫耐受期; (ii) 免疫清除期; (iii)后期 在免疫清除期,可能最终出现乙肝病毒e抗原(HBeAg)血清转换 血清转换一般伴有临床缓解 病毒的清除是减轻或阻止肝损和疾病进展的关键因素。 慢性HBV感染可以分为三个连续性的阶段:(i)免疫耐受期;(ii) 免疫清除期;以及(iii)后期。 在免疫清除期,可出现肝炎发作,而且可以并发失代偿肝病。肝炎发作或加重系由于I类组织相容性抗原(HLA)限制性的细胞毒T淋巴细胞(CTL)针对肝细胞表面HBV抗原免疫应答,导致肝细胞调亡。最终可出现乙肝病毒e抗原(HBeAg)血清转换,即e抗原消失,出现抗e抗原抗体(抗-HBe)。血清转换一般伴有临床缓解.然而HBeAg转阳或HBeAg阴性而HBV DNA阳性肝炎可引起乙肝再度活动3。当前对亚太地区HBeAg阴性、HBVDNA阳性肝炎的自然史尚未曾进行深入的研究,但可以见到这些肝炎患者出现病情活动或疾病进展4。肝炎发作时的肝小叶改变的严重程度、范围、持续时间以及频度可用于判断疾病的结局以及HBV的清除3。 但尽管如此,病毒的清除仍是减轻或阻止肝损和疾病进展的关键因素。
 免疫耐受期; (ii) 免疫清除期; (iii)后期. 在免疫清除期,可能最终出现乙肝病毒e抗原(HBeAg)血清转换. 血清转换一般伴有临床缓解. 病毒的清除是减轻或阻止肝损和疾病进展的关键因素。 慢性HBV感染可以分为三个连续性的阶段:(i)免疫耐受期;(ii) 免疫清除期;以及(iii)后期。 在免疫清除期,可出现肝炎发作,而且可以并发失代偿肝病。肝炎发作或加重系由于I类组织相容性抗原(HLA)限制性的细胞毒T淋巴细胞(CTL)针对肝细胞表面HBV抗原免疫应答,导致肝细胞调亡。最终可出现乙肝病毒e抗原(HBeAg)血清转换,即e抗原消失,出现抗e抗原抗体(抗-HBe)。血清转换一般伴有临床缓解.然而HBeAg转阳或HBeAg阴性而HBV DNA阳性肝炎可引起乙肝再度活动3。当前对亚太地区HBeAg阴性、HBVDNA阳性肝炎的自然史尚未曾进行深入的研究,但可以见到这些肝炎患者出现病情活动或疾病进展4。肝炎发作时的肝小叶改变的严重程度、范围、持续时间以及频度可用于判断疾病的结局以及HBV的清除3。 但尽管如此,病毒的清除仍是减轻或阻止肝损和疾病进展的关键因素。")
6
HBV and HCV Characteristics
Double stranded DNA virus Hepadnaviridase 4 open reading frames High viremia High infectivity Integrates into host genome No cytotoxicity HCV Single stranded RNA virus Flavivirus 1 open reading frame Low viremia Low infectivity No integration into host genome Cytotoxicity (?) HBV and HCV characteristics Although HBV and HCV share the same target organ (liver) the viruses have different characteristics, with HBV having a more complex structure than HCV. HBV is also more infectious than HCV, associated with greater viremia, and has the ability to integrate into the host genome, making it more difficult to treat. Hoofnagle JH, di Bisceglie AM.The treatment of chronic viral hepatitis. N Engl J Med 1997;336:
 HBV and HCV characteristics. Although HBV and HCV share the same target organ (liver) the viruses have different characteristics, with HBV having a more complex structure than HCV. HBV is also more infectious than HCV, associated with greater viremia, and has the ability to integrate into the host genome, making it more difficult to treat. Hoofnagle JH, di Bisceglie AM.The treatment of chronic viral hepatitis. N Engl J Med 1997;336:")
7
乙型肝炎的流行病学现状 在亚洲、非洲、中东和太平洋岛屿,HBV的慢性携带率可达10%~20%, HBV感染大多数在婴、幼儿期获得

8
不同人群HBV 血清标志物的流行率(%) 人群 HBsAg 所有标志物 出生于流行区者 13 70~85 男性同性恋(MSM) 6 35~85 注射毒品(IDU) 7 60~80 透析病人 3~10 20~80 HIV感染者 8~11 89~90 孕妇 0.4~1.5 家庭内/性接触 3~6 30~60

9
HBV感染的途径与血清学类型 1型:围产期感染,在亚洲和大洋洲,50%HBV感染者 属此类型-免疫耐受期长,血清转换晚
2型:儿童期获得性感染(接触传播),主要见于南 部非洲、阿拉斯加及地中海地区-HBeAg血 清转换发生于青春期前后 3型:成人期获得性HBV感染(性传播)主要见于发 达国家
,主要见于南. 部非洲、阿拉斯加及地中海地区-HBeAg血. 清转换发生于青春期前后. 3型:成人期获得性HBV感染(性传播)主要见于发. 达国家.")
10
World prevalence of HBV carriers Annual incidence of primary HCC
Geographic Distribution of HBV Carriers and Incidence of Hepatocellular Carcinoma (HCC) World prevalence of HBV carriers Annual incidence of primary HCC Geographic distribution of HBV carriers and incidence of HCC HBV prevalence varies around the world; the most endemic regions being Asia, the Pacific and sub-Saharan Africa. A significant correlation between the prevalence of HBV and incidence of hepatocellular carcinoma can be observed. HBV is the single most important cause of primary liver cancer. Yu MC, Yuan JM, Govindarajan S, Ross RK. Epidemiology of hepatocellular carcinoma. Can J Gastroenterol 2000;14:703-9. HBs Ag carriers prevalence <1% 1-10% >10% poorly documented Cases/100,000 population poorly documented
 World prevalence of HBV carriers. Annual incidence of primary HCC. Geographic distribution of HBV carriers and incidence of HCC. HBV prevalence varies around the world; the most endemic regions being Asia, the Pacific and sub-Saharan Africa. A significant correlation between the prevalence of HBV and incidence of hepatocellular carcinoma can be observed. HBV is the single most important cause of primary liver cancer. Yu MC, Yuan JM, Govindarajan S, Ross RK. Epidemiology of hepatocellular carcinoma. Can J Gastroenterol 2000;14: HBs Ag carriers prevalence. <1% 1-10% >10% poorly documented. Cases/100,000 population poorly documented.")
11
HBV感染的自然史-血清学变化 在亚洲和大洋洲,HBeAg的清除率为每年8%~12% 亚洲儿童HBeAg的清除率较低(ALT多正常)
在Alaska, HBV携带者5年的HBeAg清除率为45%,10年的清除率为80% 在意大利和中国台湾,ALT升高儿童的3年的HBeAg清除率为50%, 5年为70% HBsAg的清除率为每年0.5%

12
HBV感染的自然史-临床转归 就诊的HBsAg携带者肝硬化的发生率为每年2%~3%
发生肝硬化的危险因素: HBeAg+, 年龄, ALT 肝硬化患者发生失代偿的危险因素为:HBeAg+,对干扰素无应答 代偿性肝硬化患者的5年生存率为84% ,10年为68% 代偿性肝硬化患者中,HBeAg阴性者的5年生存率(97%)高于HBeAg阳性者(72%) 失代偿性肝硬化患者的5年生存率仅为14% 自发的或治疗后HBeAg转阴者均失代偿, 存活率
高于HBeAg阳性者(72%) 失代偿性肝硬化患者的5年生存率仅为14% 自发的或治疗后HBeAg转阴者均失代偿, 存活率")
13
慢性乙型肝炎治疗的目的 阻止病毒复制 减轻肝脏炎 症坏死病变 改善长期临床预后 阻止肝脏损害的进展 发展到肝硬化 预防乙型肝炎病毒
(HBV)相关的 肝细胞癌发生 延长生存期 减轻肝脏炎 症坏死病变
相关的. 肝细胞癌发生. 延长生存期. 减轻肝脏炎. 症坏死病变.")
14
认识误区 ●见“阳”色变,转“阴”欲望强 ●只求降酶 ●滥用药 ●“慢乙肝无特效药” ●只治疗、不复查、不随访 ●跟着“广告”走

15
抗病毒治疗的疗效评估标准 应答类别 生化学应答(BR): ALT降至正常范围
病毒学应答(VR): HBV-DNA下降到非扩增法无法检测水平(105COPIES/ml),治疗前HBeAg(+)病人HBeAg转(-) 组织学应答(HR):与治疗前肝活检比较, 肝组织学活动指数下降2个点以上 完全应答(CR): 满足生化和病毒应答标准 治疗评价时间 治疗中(on-therapy): 治疗期间 维持(maintained): 保持在整个疗程 治疗结束(end of treatment): 疗程结束 治疗结束后 (Off-therapy): 治疗中断以后 持久应答 (SR-6): 治疗中断后6个月 持久应答 (SR-12): 治疗中断后12个月
: HBV-DNA下降到非扩增法无法检测水平(105COPIES/ml),治疗前HBeAg(+)病人HBeAg转(-) 组织学应答(HR):与治疗前肝活检比较, 肝组织学活动指数下降2个点以上. 完全应答(CR): 满足生化和病毒应答标准. 治疗评价时间. 治疗中(on-therapy): 治疗期间. 维持(maintained): 保持在整个疗程. 治疗结束(end of treatment): 疗程结束. 治疗结束后 (Off-therapy): 治疗中断以后. 持久应答 (SR-6): 治疗中断后6个月. 持久应答 (SR-12): 治疗中断后12个月.")
16
HBV DNA的检测 何种方法最合适尚不能肯定 >105/mL作为诊断标准是人为的界限 低水平 HBV DNA的意义不明
最低检测水平为105~106的方法(非扩增法)即可满足需要
即可满足需要.")
17
几种HBVDNA定量检测方法的比较 敏感性(检测限) 方法 pg/mL copies/mL Branched DNA 2.1 7×105
(Bayer) Liquid hybridization ×105 (Abbot) Hybrid capture ×105 (Digene) Amplicor-Monitor ×102 (Roche) Molecular Beacon - <50 1pg HBV DNA= copies(~3×105 基因组当量)
 Liquid hybridization ×105 (Abbot) Hybrid capture ×105 (Digene) Amplicor-Monitor ×102 (Roche) Molecular Beacon - <50. 1pg HBV DNA= copies(~3×105 基因组当量)")
18
治疗原则 抗病毒药物应用 免疫调节剂 抗病毒药物联合免疫调节剂 改善肝功能及抗肝纤维化药物

19
抗病毒药物 干扰素 核苷类似物 中药 重组干扰素 拉米夫定(Lamivudine) 苦参素 复合干扰素 阿德福韦 (Adefovir)
干扰素 核苷类似物 中药 重组干扰素 复合干扰素 长效干扰素 拉米夫定(Lamivudine) 阿德福韦 (Adefovir) 恩替卡韦 (Entecavir) 苦参素 苦参碱 氧化苦参碱 叶下珠等
 阿德福韦 (Adefovir) 恩替卡韦 (Entecavir) 苦参素. 苦参碱. 氧化苦参碱. 叶下珠等.")
20
抗乙肝病毒新的靶位和治疗方法 小分子抑制剂 小分子干扰RNA 免疫调节剂 DNA多聚酶抑制剂 IL-12, IL-18 核酶, 反义核酸,
干扰肽, 治疗性疫苗 IL-12, IL-18 LAM, ADV, ETV, LY582563,MIV-210 -胸腺素 病毒包装抑制剂 树突状细胞 AT-61, AT-130, Bay

21
拉米夫定治疗慢性乙型肝炎疗效 国内 304例 3年疗效结果: HBeAg 转阴率(转换率) 第1年 18% (14%)
国内 304例 3年疗效结果: HBeAg 转阴率(转换率) 第1年 18% (14%) 第2年 36% (22%) 第3年 42% (34%) ALT复常率 68% (3年随访) YMDD变异发生率 71%
 第1年 18% (14%) 第2年 36% (22%) 第3年 42% (34%) ALT复常率 68% (3年随访) YMDD变异发生率 71%")
22
拉米夫定(贺普丁) 核苷类似物 2’3’-二脱氧3’-硫代胞嘧啶的左旋镜像体 与核苷相互作用的人体蛋白质只对右旋镜像体构型有高度选择性
Slide 1 贺普丁是一种胞嘧啶衍生物,和绝大多数核苷类似物一样,它通过抑制病毒核酸合成发挥抗病毒作用 多数核苷能以互为镜像体的两种形式存在。自然界存在的核苷多为右旋体,而贺普丁则为纯左旋体,即它是以与天然核苷完全相反的构型存在的。与核苷相互作用的人体蛋白质对右旋镜像体构型具有高度的选择性,而不能与左旋镜像体的贺普丁发生相互作用 这种差异与贺普丁的临床疗效及安全性密切相关。贺普丁左旋体的细胞毒性远低于其右旋体 一种低毒性,高效,选择性的HBV复制的抑制剂

23
拉米夫定:临床药理 可被迅速良好吸收(Tmax约1小时, Cmax1.1-1.5mg/ml)。 生物利用度(F)=80~85%
口服100mg,每日一次,可使贺普丁血药浓度保持在使乙肝病毒复制减少50%的水平(IC50) Slide 4 贺普丁口服制剂的绝对生物利用度约为80~85%,服用后0.5~1.5小时既达到血浆高峰浓度 贺普丁口服100mg每日一次能保证血药浓度始终不低于抑制HBV的最低浓度 约70%贺普丁在尿中以原形排泌 不到10%的贺普丁在肝脏代谢,因此不同程度肝功能损害病人可安全服用贺普丁 贺普丁蛋白结合率低,安全性好,发生药物间相互作用的可能性小
 Slide 4. 贺普丁口服制剂的绝对生物利用度约为80~85%,服用后0.5~1.5小时既达到血浆高峰浓度. 贺普丁口服100mg每日一次能保证血药浓度始终不低于抑制HBV的最低浓度. 约70%贺普丁在尿中以原形排泌. 不到10%的贺普丁在肝脏代谢,因此不同程度肝功能损害病人可安全服用贺普丁. 贺普丁蛋白结合率低,安全性好,发生药物间相互作用的可能性小.")
24
拉米夫定:临床药理 经肾脏以原形排出 经肝脏代谢极少,肝功能受损对拉米夫定的药代动力学无显著影响,对于肝功能下降的病人,无需减少剂量
临床上无明显的药物间相互作用 食物对其临床药理特点(生物利用度)没有影响 中度至重度肾功能不全需减少用药量 Slide 5 贺普丁极小部分经肝脏代谢,故对肝功能下降病人无需调整剂量,而在肾功能不全时要调整剂量。
没有影响. 中度至重度肾功能不全需减少用药量. Slide 5. 贺普丁极小部分经肝脏代谢,故对肝功能下降病人无需调整剂量,而在肾功能不全时要调整剂量。")
25
乙肝病毒的复制 拉米夫定的抑制作用 拉米夫定 有感染性的 HBV毒粒 有感染性的 HBV毒粒 胞浆膜 肝细胞 HBsAg的囊膜 抗原成分
部分双链 的DNA 逆转录 Slide 3 右侧2条直线代表贺普丁参与DNA链复制过程, 直接抑制病毒复制 左侧2条虚线是代表贺普丁因为抑制了部分双链DNA的形成从而间接抑制病毒的过程 内质网 (-)-DNA 有包膜的 前基因组 A(n) cccDNA 转录 mRNA 细胞浆 细胞核 翻译
-DNA. 有包膜的. 前基因组. A(n) cccDNA. 转录. mRNA. 细胞浆. 细胞核. 翻译.")
26
HBeAg+ CHB With ALT Elevation
治疗1年的HBeAg血清转换率16%~18% (n=731) 组织学改善率为49%~56% 治疗时间延长, HBeAg血清转换率增加 治疗2、3、4年的HBeAg血清转换率分别为27%、33%、47% 治疗前ALT水平是最重要的预测因子,ALT正常、1~2倍、2~5倍、5倍以上者HBeAg血清转换率分别为2%、9%、21%、47%
 组织学改善率为49%~56% 治疗时间延长, HBeAg血清转换率增加. 治疗2、3、4年的HBeAg血清转换率分别为27%、33%、47% 治疗前ALT水平是最重要的预测因子,ALT正常、1~2倍、2~5倍、5倍以上者HBeAg血清转换率分别为2%、9%、21%、47%")
27
拉米夫定耐药的定义 抗病毒治疗过程中血清HBV DNA水平升高,即表型耐药
HBV多聚酶基因出现选择性变异,即基因型耐药(Genotypic resistance) 指1896位置变异? 注意点: 依从性 治疗前不是优势毒株 在数据库中,与参照序列比较,是新的变异
 指1896位置变异? 注意点: 依从性. 治疗前不是优势毒株. 在数据库中,与参照序列比较,是新的变异.")
28
Lamivudine Resistance
基因型耐药率 1年:14%~32%;2年:38% 3年:49%; 年:66% 耐药后继续拉米夫定治疗,仍有一定的疗效 耐药后部分病人病情加重 HBeAg-CHB的耐药率差别很大 1年:0%~27% 2年:10%~56%

29
HBV多聚酶模型 核苷酸结合槽 Explanation:
Through computer assisted modelling, it has been possible to develop a 3- dimensional structural model of HBV DNA polymerase and the active binding site containing the YMDD motif. The YMDD (the amino acid sequence tyrosine-methionine-aspartate-aspartate) motif lies within the nucleotide binding pocket of the HBV DNA polymerase. Genetic sequencing shows that spontaneous mutation of the HBV genome causes 3 groups of changes in and near the YMDD motif. Protein modelling suggests that these changes disrupt interactions between lamivudine triphosphate and the HBV polymerase but the polymerase protein remains functional.
 motif lies within the nucleotide binding pocket of the HBV DNA polymerase. Genetic sequencing shows that spontaneous mutation of the HBV genome causes 3 groups of changes in and near the YMDD motif. Protein modelling suggests that these changes disrupt interactions between lamivudine triphosphate and the HBV polymerase but the polymerase protein remains functional.")
30
Antiviral Response to Interferon and Lamivudine Therapy

31
第三代核苷类药物 ADEFOVIR ENTECAVIR

32
cccDNA的定量分析及ADV的抑制作用(一)
目的:1、建立检测方法 2、cccDNA的自然变化 3、ADV对cccDNA的影响 方法:病例 1、48例HBeAg+慢性乙肝 2、15例HBeAg-慢性乙肝 3、11例非活动性HBsAg携带者 4、6例急性乙肝恢复期,抗HBs+ 荧光定量PCR方法检测ccc DNA和总DNA

33
cccDNA的定量分析及ADV的抑制作用(二)
结果:1、cccDNA检测范围0.001拷贝/cell 2、 HBeAg+ 组cccDNA平均水平是HBeAg-的 100 倍( 1.0拷贝/cell对0.01拷贝/cell) 3、 HBeAg+ 组细胞内总HBV DNA是HBeAg- 组的121倍(114.9拷贝/cell对0.95拷贝/cell 4、急性乙肝恢复期患者cccDNA极少(0.006 拷贝/cell) 5、HBsAg携带者cccDNA平均水平为0.044拷贝/cell 6、ADV治疗48周,细胞内总HBV DNA下降61倍, cccDNA下降11.5倍 7、 HBeAg血清转换者的基线cccDNA低于未发生 转换者 8、 治疗48后HBeAg血清转换者的cccDNA水平与 HBsAg携带者相似
 3、 HBeAg+ 组细胞内总HBV DNA是HBeAg- 组的121倍(114.9拷贝/cell对0.95拷贝/cell. 4、急性乙肝恢复期患者cccDNA极少( 拷贝/cell) 5、HBsAg携带者cccDNA平均水平为0.044拷贝/cell. 6、ADV治疗48周,细胞内总HBV DNA下降61倍, cccDNA下降11.5倍. 7、 HBeAg血清转换者的基线cccDNA低于未发生. 转换者. 8、 治疗48后HBeAg血清转换者的cccDNA水平与. HBsAg携带者相似.")
34
cccDNA的定量分析及ADV的抑制作用(三)
结论:1、cccDNA是肝内HBV复制的可靠标志 2、ADV可显著降低cccDNA水平 3、 cccDNA下降的速度比血清和肝内 HBV DNA慢 4、cccDNA水平可作为抗病毒治疗疗效 的检测指标 5、 cccDNA水平可作为慢性乙肝预后的 独立的预测因子 Betina Werle, 法国

35
拉米夫定治疗失败者再用entecavir治疗
目的:了解entecavir对拉米夫定治疗无效或有YMDD变异者的疗效 方法:181例拉米夫定治疗无效或有YMDD变异者(87%)分为4组, 分别接受 entecavir 0.1mg、0.5mg、1mg和拉米夫定100mg治 疗,监测ALT、 HBV DNA水平和YMDD变异 结果:1、4组48周的ALT复常率分别为43%、59%、68%和6%(p<0.001) 2、4组48周的HBV DNA水平(Log10)分别下降2.87、4.46、5.11和1.41(p<0.001) 3、无新的变异发现 4、无明显副作用 结论:1、拉米夫定治疗无效或有YMDD变异者再用entecavir ,仍有明显 疗效 2、 entecavir 1mg为最佳剂量 Ting-Tsung Chang, 台湾
分为4组, 分别接受 entecavir 0.1mg、0.5mg、1mg和拉米夫定100mg治. 疗,监测ALT、 HBV DNA水平和YMDD变异. 结果:1、4组48周的ALT复常率分别为43%、59%、68%和6%(p<0.001) 2、4组48周的HBV DNA水平(Log10)分别下降2.87、4.46、5.11和1.41(p<0.001) 3、无新的变异发现. 4、无明显副作用. 结论:1、拉米夫定治疗无效或有YMDD变异者再用entecavir ,仍有明显. 疗效. 2、 entecavir 1mg为最佳剂量. Ting-Tsung Chang, 台湾.")
36
Dose ranging - Change in HBV DNA (Quantiplex™) - 4 week treatment
Treatment-naive and IFN/LVD pre-treated Treatment 1 2 3 4 5 6 7 Weeks -3 -2 -1 Mean change log HBV DNA Placebo 0.05 mg ETV 0.1 mg ETV 1.0 mg ETV 0.5 mg ETV 8

37
Dose ranging - Change in HBV DNA (PCR) - 24 week treatment
Nucleoside-naïve and interferon-pre treated 0.1 and 0.5 ETV vs. LVD, p=0.0001; 0.5 vs. 0.1 ETV, p=0.018 AI

38
Phase II - Change in HBV DNA (PCR) Lamivudine-resistant patients
-0.9 -1.4 -1 -1.8 100mg LVD -2 -2.8 Mean Change in Log10 HBV DNA 0.1mg ETV -3 -3.7 -4.4 -4 0.5mg ETV -4.2 -5 1.0mg ETV -5.0 -6 B/L Weeks Group: Number at Risk LVD: ETV 0.1: ETV 0.5: ETV 1.0: AI

39
LdT国际多中心临床试验:中期结果分析 目的:评价LDT(Telbivudine)的疗效和安全性 方法:1、5个国家或地区的104病例入选
2、随机、双盲分5组,治疗52周,即 LdT(600mg/d)、 LdT(400mg/d) LdT(600mg/d)+Lam(100mg/d) LdT(400mg/d)+Lam(100mg/d) Lam(100mg/d) 结果:1、治疗12周后HBV DNA下降情况(Log) LDT600:4.64; LdT400: 4.34; LdT400+Lam:4.97; LdT600+Lam:5.05; Lam:3.87 2、治疗12周后, 52%含LdT组患者的HBV DNA水 平降至4Log以下;Lam仅为20% 结论:LdT的抗病毒作用优于Lam Ching-Lung Lai, Hong kong
、 LdT(400mg/d) LdT(600mg/d)+Lam(100mg/d) LdT(400mg/d)+Lam(100mg/d) Lam(100mg/d) 结果:1、治疗12周后HBV DNA下降情况(Log) LDT600:4.64; LdT400: 4.34; LdT400+Lam:4.97; LdT600+Lam:5.05; Lam: 、治疗12周后, 52%含LdT组患者的HBV DNA水. 平降至4Log以下;Lam仅为20% 结论:LdT的抗病毒作用优于Lam. Ching-Lung Lai, Hong kong.")
40
L-脱氧胸腺嘧啶 ( LdT, Telbivudine)
在体内转变为LdT三磷酸(LdT-TP)而发挥作用 细胞内的LdT-TP浓度可达27.7 μM(LdT 10 μM,24h) 对HBV和DHBV的体外中位数有效浓度(EC50)分别为: 0.19μM和0.18 μM 细胞内HBV复制中间体的EC50:0.29 μM 细胞内半衰期:14h LdT可抑制HBV、WHV和DHBV的DNA聚合酶,IC50分别为0.46、1.0和0.24 μM LdT对人DNA聚合酶无抑制作用 对病毒DNA聚合酶抑制的机理仍不清楚
而发挥作用. 细胞内的LdT-TP浓度可达27.7 μM(LdT 10 μM,24h) 对HBV和DHBV的体外中位数有效浓度(EC50)分别为: 0.19μM和0.18 μM. 细胞内HBV复制中间体的EC50:0.29 μM. 细胞内半衰期:14h. LdT可抑制HBV、WHV和DHBV的DNA聚合酶,IC50分别为0.46、1.0和0.24 μM. LdT对人DNA聚合酶无抑制作用. 对病毒DNA聚合酶抑制的机理仍不清楚.")
41
I/II临床试验 入选对象:HBeAg+慢性乙肝患者 分组:7组,每组7例,LdT与安慰剂的比例为6:1, 疗程4周
剂量25、50、100、200、400、800mg/d 无SAE发生 在400和800mg组,HBV DNA下降3.6~4 log,优于其它核苷类似物的1.5~2.9log(包括lamivudine, adefovir, entecavir) 停药后HBV DNA恢复至治疗前水平
 停药后HBV DNA恢复至治疗前水平.")
42
IIb期随机、双盲国际多中心临床试验 入选对象:HBeAg+慢性乙肝患者107例
LdT400或600mg/d、Lam100mg/d治疗52周,随访16周,分为5组 12周结果 HBV DNA下降4.34 (400mg)和4.64 log (600mg), lamivudine组3.87 log 联合组分别下降4.97 log 和5.05 log 含LdT组,ALT复常率高 剂量600mg/d最为适合 试验结果仍在分析中
和4.64 log (600mg), lamivudine组3.87 log. 联合组分别下降4.97 log 和5.05 log. 含LdT组,ALT复常率高. 剂量600mg/d最为适合. 试验结果仍在分析中.")
43
长效干扰素 (Peginterferon)
二期临床试验 例CHB患者治后: HBeAg 转阴率 37% (18/49,90ug/周 /24周) 35%(16/46,180mg/周/24周) 29%(14/48,270mg/周/24周) 对照组(IFN-à2a) HBeAg转阴率 25% (13/51)
 35%(16/46,180mg/周/24周) 29%(14/48,270mg/周/24周) 对照组(IFN-à2a) HBeAg转阴率 25% (13/51)")
44
蛋白的聚乙二醇化 聚乙二醇化(PEG)蛋白1: 新蛋白的特征依赖1,2: 延长血浆半衰期 降低清除率 降低免疫原性
结合位点 Slide 44. Protein Pegylation Pegylation prolongs the plasma half-life of protein drugs (from 3- to 486-fold) and renders them less immunogenic. Since pegylated proteins are surrounded by an attached polyethylene glycol (PEG) moiety, they are less rapidly metabolized by the body's enzymes than are unmodified proteins and remain in the host longer to perform their therapeutic activity. The size of the PEG moiety is of particular importance, since larger pegylated molecules can provide more sustained drug exposure, thus eliminating critical peak-to-trough fluctuations and optimizing suppression of HCV infection.1 Additional enhancements conferred by pegylation include improved solubility, decreased proteolysis, reduced kidney clearance, and beneficial alterations in distribution and absorption.2,3 Pegylation of therapeutic proteins or peptides is generally accomplished by means of establishing a covalent bond between an amino or sulfhydryl group on the parent compound and a chemically reactive group (ie, carbonate, ester, aldehyde, tresylate) on the PEG moiety. The characteristics of the resulting molecule depend on the structure of the PEG moiety (eg, size, linear or branched, linkage bond strength) and the site of attachment to the parent compound.1 In HCV-infection therapy, pegylation of conventional IFN has enhanced its pharmacokinetic profile and therapeutic efficacy. For example, pegylation of the IFN alfa-2a molecule augments its terminal half-life from 5.1 hours (IFN alfa-2a) to 77 hours (PEGASYS® [peginterferon alfa-2a (40KD)], Hoffmann-La Roche) in healthy adults,4,5 thus permitting less frequent dosing. Additionally, compared with conventional IFN alfa-2a, PEGASYS® exhibits reduced renal clearance, and its pharmacokinetics are not affected in patients with renal impairment.5,6 Currently, two pegylated formulations of IFN have been developed for the treatment of CHC— PEGASYS® and PEG-Intron™ (peginterferon alfa-2b [12KD], Schering). 1. Hoffmann-La Roche. Roche Facets. PEGASYS. 2. Delgado C et al. Clin Rev Ther Drug Carrier Syst. 1992;9: Kozlowski A et al. BioDrugs. 2001;15: ROFERON®-A. PDR ®. 56th ed Perry CM, Jarvis B. Drugs. 2001;61: Martin P et al. Hepatology. 2000;32(suppl):370A. 1. Delgado C et al. Clin Rev Ther Drug Carrier Syst. 1992;9: Hoffmann-La Roche. Roche Facets.
 and renders them less immunogenic. Since pegylated proteins are surrounded by an attached polyethylene glycol (PEG) moiety, they are less rapidly metabolized by the body s enzymes than are unmodified proteins and remain in the host longer to perform their therapeutic activity. The size of the PEG moiety is of particular importance, since larger pegylated molecules can provide more sustained drug exposure, thus eliminating critical peak-to-trough fluctuations and optimizing suppression of HCV infection.1 Additional enhancements conferred by pegylation include improved solubility, decreased proteolysis, reduced kidney clearance, and beneficial alterations in distribution and absorption.2,3. Pegylation of therapeutic proteins or peptides is generally accomplished by means of establishing a covalent bond between an amino or sulfhydryl group on the parent compound and a chemically reactive group (ie, carbonate, ester, aldehyde, tresylate) on the PEG moiety. The characteristics of the resulting molecule depend on the structure of the PEG moiety (eg, size, linear or branched, linkage bond strength) and the site of attachment to the parent compound.1. In HCV-infection therapy, pegylation of conventional IFN has enhanced its pharmacokinetic profile and therapeutic efficacy. For example, pegylation of the IFN alfa-2a molecule augments its terminal half-life from 5.1 hours (IFN alfa-2a) to 77 hours (PEGASYS® [peginterferon alfa-2a (40KD)], Hoffmann-La Roche) in healthy adults,4,5 thus permitting less frequent dosing. Additionally, compared with conventional IFN alfa-2a, PEGASYS® exhibits reduced renal clearance, and its pharmacokinetics are not affected in patients with renal impairment.5,6. Currently, two pegylated formulations of IFN have been developed for the treatment of CHC— PEGASYS® and PEG-Intron™ (peginterferon alfa-2b [12KD], Schering). 1. Hoffmann-La Roche. Roche Facets. PEGASYS. 2. Delgado C et al. Clin Rev Ther Drug Carrier Syst. 1992;9: Kozlowski A et al. BioDrugs. 2001;15: ROFERON®-A. PDR ®. 56th ed Perry CM, Jarvis B. Drugs. 2001;61: Martin P et al. Hepatology. 2000;32(suppl):370A. 1. Delgado C et al. Clin Rev Ther Drug Carrier Syst. 1992;9: Hoffmann-La Roche. Roche Facets.")
45
多次注射平均浓度——时间曲线 PEG-Intron™ PEGASYS® 180 mg qw 1200 30 1000 25 800 20
周一 周二 周三 周四 周五 周六 周日 0.5 mg/kg qw 1.0 mg/kg qw 1.5 mg/kg qw 30 1000 25 800 20 浓度 (pg/mL) 600 浓度 (ng/mL) 15 400 Slide 45. Mean Concentration-Time Profiles of Multiple-Dose Injections The graph on the left depicts the mean concentration-time curves after multiple doses of PEG-Intron™ (peginterferon alfa-2b [12KD]) 0.5, 1.0, and 1.5 g/kg administered weekly. As illustrated in the graph, wide fluctuations in serum concentration occurred during the course of the weekly dosing interval for all doses shown. The peak-to-trough ratio was 1:100. The mean terminal half-life for the three doses was 34.2, 37.1, and 33.9 hours, respectively. Maximum concentration occurred at 22, 16, and 19 hours, respectively; serum concentrations of PEG-Intron™ were no longer measurable at 84, 148, and 160 hours postdose, respectively, indicating insufficient bioavailability and diminished antiviral coverage prior to administration of the next dose.1 Illustrated on the right is the mean time-concentration curves after multiple doses of PEGASYS® (peginterferon alfa-2a [40KD]) 180 g given weekly.2 At the time of injection (0 hours), the concentration of the agent maintained from previous doses is sufficient to provide sustained systemic exposure during the full 7-day dosing interval.2,3 1. Glue P et al. Clin Pharmacol Ther. 2000;68: Modi MW. AASLD Annual Meeting Modi MW et al. Hepatology. 2000;32(suppl):394A. 10 200 5 24 48 72 96 120 144 168 24 48 72 96 120 144 168 时间(小时) 时间(小时) Adapted from Glue P et al. Clin Pharmacol Ther. 2000;68: Modi MW. AASLD Annual Meeting
 600. 浓度 (ng/mL) Slide 45. Mean Concentration-Time Profiles of Multiple-Dose Injections The graph on the left depicts the mean concentration-time curves after multiple doses of PEG-Intron™ (peginterferon alfa-2b [12KD]) 0.5, 1.0, and 1.5 g/kg administered weekly. As illustrated in the graph, wide fluctuations in serum concentration occurred during the course of the weekly dosing interval for all doses shown. The peak-to-trough ratio was 1:100. The mean terminal half-life for the three doses was 34.2, 37.1, and 33.9 hours, respectively. Maximum concentration occurred at 22, 16, and 19 hours, respectively; serum concentrations of PEG-Intron™ were no longer measurable at 84, 148, and 160 hours postdose, respectively, indicating insufficient bioavailability and diminished antiviral coverage prior to administration of the next dose.1. Illustrated on the right is the mean time-concentration curves after multiple doses of PEGASYS® (peginterferon alfa-2a [40KD]) 180 g given weekly.2 At the time of injection (0 hours), the concentration of the agent maintained from previous doses is sufficient to provide sustained systemic exposure during the full 7-day dosing interval.2,3. 1. Glue P et al. Clin Pharmacol Ther. 2000;68: Modi MW. AASLD Annual Meeting Modi MW et al. Hepatology. 2000;32(suppl):394A 时间(小时) 时间(小时) Adapted from Glue P et al. Clin Pharmacol Ther. 2000;68: Modi MW. AASLD Annual Meeting")
46
PEGASYS® 药物动力学 (聚乙二醇化 α - 2a 干扰素 [40KD])
周一 周二 周三 周四 周五 周六 周日 30 25 PEG-IFN -2a (40KD) 180 mg qw 20 15 平均浓度(ng/mL) 10 5 Slide 46. Pharmacokinetics of PEGASYS® (Peginterferon Alfa-2a [40KD]) PEGASYS® (peginterferon alfa-2a [40KD]) is associated with antiviral coverage that is sustained throughout the weekly dosing interval. After one sc injection of PEGASYS® 180 g, the serum drug level reaches a maximum concentration of 14.2 ng/mL (bottom curve).1 Unlike the drug concentration-time curve for nonpegylated IFNs2 (see Slide 35), serum concentrations of PEGASYS® are constant and sustained throughout the week. Until steady state is reached (5 to 9 weeks), serum concentrations more than double and are constant and sustained throughout the week.3 After steady state is reached, further drug accumulation does not occur (the amount of PEGASYS® eliminated from the body equals the amount entering via administration). The concentration-time curve for the week 9 injection (not shown) would be similar to that for the week 48 injection (top curve).3 Once the entire treatment course with PEGASYS® 180 g once weekly has been completed, the serum concentration levels slowly descend4; complete elimination of the drug occurs within 50 to 60 days posttreatment (not shown, see Slide 40 [Metabolic Fate of PEGASYS® (Peginterferon Alfa-2a [40KD]): Metabolism and Excretion via Urine and Bile]).3 1. Algranati NE et al. AASLD Annual Meeting Koslowski A et al. BioDrugs. 2001;15: Modi MW. AASLD Annual Meeting Modi MW et al. Hepatology. 2000;32(suppl):394A. 24 48 72 96 120 144 168 时间(小时) 首剂注射后1 达到稳态后2 1. Algranati NE et al. AASLD Annual Meeting Modi MW. AASLD Annual Meeting
![PEGASYS® 药物动力学 (聚乙二醇化 α - 2a 干扰素 [40KD])](http://slidesplayer.com/slide/11505300/62/images/46/PEGASYS%C2%AE+%E8%8D%AF%E7%89%A9%E5%8A%A8%E5%8A%9B%E5%AD%A6+%28%E8%81%9A%E4%B9%99%E4%BA%8C%E9%86%87%E5%8C%96+%CE%B1+-+2a+%E5%B9%B2%E6%89%B0%E7%B4%A0+%5B40KD%5D%29.jpg "周一. 周二. 周三. 周四. 周五. 周六. 周日 PEG-IFN -2a (40KD) 180 mg qw 平均浓度(ng/mL) Slide 46. Pharmacokinetics of PEGASYS® (Peginterferon Alfa-2a [40KD]) PEGASYS® (peginterferon alfa-2a [40KD]) is associated with antiviral coverage that is sustained throughout the weekly dosing interval. After one sc injection of PEGASYS® 180 g, the serum drug level reaches a maximum concentration of 14.2 ng/mL (bottom curve).1 Unlike the drug concentration-time curve for nonpegylated IFNs2 (see Slide 35), serum concentrations of PEGASYS® are constant and sustained throughout the week. Until steady state is reached (5 to 9 weeks), serum concentrations more than double and are constant and sustained throughout the week.3 After steady state is reached, further drug accumulation does not occur (the amount of PEGASYS® eliminated from the body equals the amount entering via administration). The concentration-time curve for the week 9 injection (not shown) would be similar to that for the week 48 injection (top curve).3. Once the entire treatment course with PEGASYS® 180 g once weekly has been completed, the serum concentration levels slowly descend4; complete elimination of the drug occurs within 50 to 60 days posttreatment (not shown, see Slide 40 [Metabolic Fate of PEGASYS® (Peginterferon Alfa-2a [40KD]): Metabolism and Excretion via Urine and Bile]) Algranati NE et al. AASLD Annual Meeting Koslowski A et al. BioDrugs. 2001;15: Modi MW. AASLD Annual Meeting Modi MW et al. Hepatology. 2000;32(suppl):394A 时间(小时) 首剂注射后1. 达到稳态后2. 1. Algranati NE et al. AASLD Annual Meeting Modi MW. AASLD Annual Meeting")
47
聚乙二醇化干扰素:药物动力学特征 2–5 无限 77 » 40 清除半衰期,h1,3,4,7 1.5-2.0 100 峰/ 谷比值6 50
4.6 2.3 吸收半衰期, h2-5 80 1,540 11,800–16,170 清除率,mL/h1-3 6–14† 80* 31–98 分布容积,L1,2 PEGASYSÒ PEG-Intron™ IFN 药物动力学参数 Slide 47. Pegylated Interferons: Pharmacokinetic Properties The pharmacokinetics of conventional IFNs differ significantly from those of pegylated IFNs (PEG-IFNs). In addition, PEG-IFN pharmacokinetics differ based on the type of pegylation employed, principally the size and nature of the PEG molecule attached. In the case of PEGASYS® (peginterferon alfa-2a [40KD]), the use of a 40-KD PEG molecule results in a molecular entity with a low volume of distribution, reduced clearance, and an increased half-life.1-6 1. Perry CM, Jarvis B. Drugs. 2001;61: Glue P et al. Clin Pharmacol Ther. 2000;68: PEG-Intron™. PDR ®. 56th ed INTRON® A. PDR ®. 56th ed Reddy KR. Ann Pharmacother. 2000;34: Hoffmann-La Roche. PEGASYS®. Monograph. *根据患者体重而改变 †不随患者体重改变 Perry CM, Jarvis B. Drugs. 2001;61: Glue P et al. Clin Pharmacol Ther. 2000;68: PEG-Intron™. PDR ®. 56th ed ROFERON®-A. PDR ®. 56th ed Reddy KR Ann Pharmacother. 2000;34: Hoffmann-La Roche. PEGASYS® Monograph. 7. INTRON® A. PDR ®. 56th ed
. In addition, PEG-IFN pharmacokinetics differ based on the type of pegylation employed, principally the size and nature of the PEG molecule attached. In the case of PEGASYS® (peginterferon alfa-2a [40KD]), the use of a 40-KD PEG molecule results in a molecular entity with a low volume of distribution, reduced clearance, and an increased half-life Perry CM, Jarvis B. Drugs. 2001;61: Glue P et al. Clin Pharmacol Ther. 2000;68: PEG-Intron™. PDR ®. 56th ed INTRON® A. PDR ®. 56th ed Reddy KR. Ann Pharmacother. 2000;34: Hoffmann-La Roche. PEGASYS®. Monograph. *根据患者体重而改变. †不随患者体重改变. Perry CM, Jarvis B. Drugs. 2001;61: Glue P et al. Clin Pharmacol Ther. 2000;68: PEG-Intron™. PDR ®. 56th ed ROFERON®-A. PDR ®. 56th ed Reddy KR Ann Pharmacother. 2000;34: Hoffmann-La Roche. PEGASYS® Monograph. 7. INTRON® A. PDR ®. 56th ed")
48
初步结论(一) PEG-IFN a-2a (40KD) (PEGASYS®) 每周用药一次在治疗 HBeAg+ 的慢性乙型肝炎过程中有良好的依从性 剂量为 180 µg 时,与常规 a-2a 干扰素相比降低 HBeAg 的速度和幅度大,降低 HBV DNA水平的程度大 PEG-IFN a-2a (40KD) 单一治疗具有良好的耐受性
 单一治疗具有良好的耐受性.")
49
初步结论(二) 治疗前的 HBeAg 和 HBV DNA 水平低可预示 PEG-IFN a-2a (40KD)治疗有效
PEG-IFN a-2a (40KD) 对难治性疾病的治疗较常规 a-2a 干扰治疗有效: 治疗前 ALT 水平低 治疗前 HBV DNA 水平低 (存在肝硬化或向肝硬化转变) 大规模、III 期、多中心临床试验的结果正在总结 I don’t know if it is accepted that cirrhosis is a predictor per se of non-response. Can we have univariate and/or multivaraite analysis to indicate which of those is most important and to give figures for gender and age, the former of which may be predictive.
 对难治性疾病的治疗较常规 a-2a 干扰治疗有效: 治疗前 ALT 水平低. 治疗前 HBV DNA 水平低. (存在肝硬化或向肝硬化转变) 大规模、III 期、多中心临床试验的结果正在总结. I don’t know if it is accepted that cirrhosis is a predictor per se of non-response. Can we have univariate and/or multivaraite analysis to indicate which of those is most important and to give figures for gender and age, the former of which may be predictive.")
50
免疫耐受形成机制 HBV野生株诱导的免疫耐受 HBV突变株的免疫逃避 HBVS基因突变 HBV前C区基因突变 HBVC基因突变

51
Immunogenic Complex Constructed by using
Hepatitis B Vaccine with Human Anti-HBs Ig

52
TABLE STATUS OF PATIENTS BEFORE AND AFTER HBVAC-HBIG TREAMENT
Number of Patients Positive For HBV-DNA HBeAg Anti-Hbe HBsAg Anti-HBs Before Treament After Treament 1 month 3 month 4 month 5 month 6 month

53
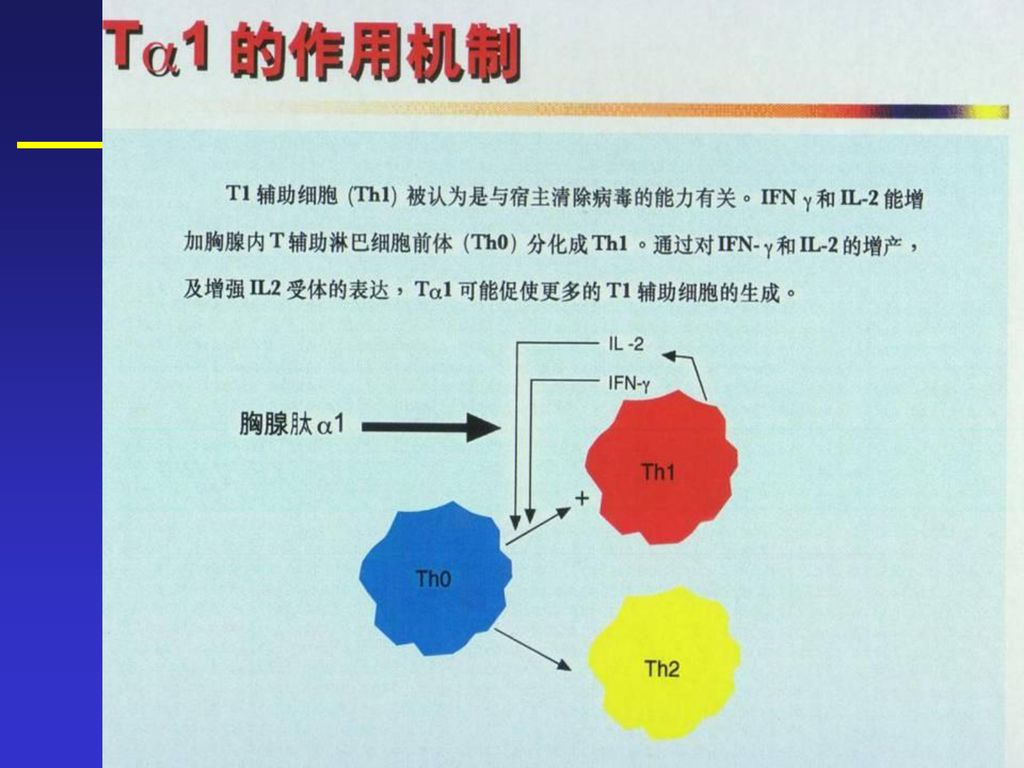
Thymosin -1(Thymalfasin)
5 10 Ac— Ser Asp Ala Ala Val Asp Thr Ser Ser Glu Ile Thr Originally isolated from thymus The peptide responsible for reconstitution of immune function in thymectomized animal models Non-glycosylated, N-terminal acetylated, 28 amino acids Highly conserved sequence(identical in human, ovine, bovine, avian, murine, porcine) Comprises the N-terminus of prothymosin(113 amino acids) Circulates at approximately 1 ng/ml(0.3nM) Thr Lys Asp Leu Lys Asn Glu Ala Glu Glu Val Val Glu Lys Lys Glu 28 25 20
 Comprises the N-terminus of prothymosin(113 amino acids) Circulates at approximately 1 ng/ml(0.3nM) Thr. Lys. Asp. Leu. Lys. Asn. Glu. Ala. Glu. Glu. Val. Val. Glu. Lys. Lys. Glu")
54
Thymosin 1(Thymalfasin)-Animal Models
Infectious disease Hepatitis Woodchuck Reduction in viral DNA Influenza Mouse Increase in survival Candida, listeria Mouse Resistance to infection Cancer B16 melanoma Mouse Decrease in tumor size, Lewis lung carcinoma Mouse increase in survival, Friend erythroleukemia Mouse decrease in metastases Colorectal cancer Rat Vaccine Enhancement Influenza Mouse Increase in cytotoxic activity Tetanus Mouse Increase in specific antibody

56
单用T1治疗慢乙肝(CHB)的荟萃分析 完全反应=ALT复常+DNA阴转或eAg+DNA同时阴转 在治疗毕随访6-12月评估
1. Hepatology(1991), vol. 14, No Hepatology(1991), A1990 2. Gastroenterology(1995), vol. 108, A Hepatology(1997), A1192 3. Hepatology(1998), vol. 27, No Unpublished 4. Hepatology(1996), vol. 24, No. 4
, vol. 14, No Hepatology(1991), A Gastroenterology(1995), vol. 108, A Hepatology(1997), A Hepatology(1998), vol. 27, No Unpublished. 4. Hepatology(1996), vol. 24, No. 4.")
57
联合应用日达仙及干扰素(IFN)的验证结果:
** 不能耐受IFN副作用者,单用T1为期一年

58
日达仙用于重型肝炎治疗的经验荟萃 上述文献中多数还提出,日达仙有助于降低重型肝火并发细菌感染,使用日达仙宜早不宜迟,疗效确切。
文献:千禧年全国日达仙肝火会议

59
抗病毒联合治疗 联合治疗优越性和理论依据 1、提高疗效; 2、阻止或延缓病毒耐药株产生; 3、防止停药后复发; 4、减少药物用量。

60
苦参素注射液是从绿色天然植物中药苦豆子中提取的生物碱,其中氧化苦参碱(oxymatrine)占98%以上,含有极少量槐果碱、槐胺碱和槐啶碱。
占98%以上,含有极少量槐果碱、槐胺碱和槐啶碱。")
61
近期研究发现Oxy具有直接的抗HBV作用
能抑制肝脏胶元活动度、防止肝硬化、阻断肝细胞凋亡和保护肝细胞等作用,均为治疗病毒性肝炎提供了充分的实验依据。

62
直接抗HBV作用 能抑制含HBV基因的2.2.15细胞分泌HBsAg和HBeAg,对二者的抑制率分别达93%及63%,并且细胞毒性低。

63
慢性乙型肝炎治疗的展望 联合/序贯治疗 小分子抑制剂 新型核苷类似物: LY582563、MIV-210
病毒包装的抑制剂: AT-61、AT-130 非核苷类抑制剂:Bay 、Bay Bay 基因治疗:基因沉默技术、DNA疫苗、核酶、 反义核酸等 免疫治疗:IL-12、IL-18;DC免疫;免疫复合 物疫苗

64
门冬氨酸钾镁 在肝病治疗中的机理和疗效探讨

65
镁的基础作用 是细胞内含量仅次于钾的主要阳离子 1、 Mg2+参与ATP生成及释放 2、 Mg2+是多种酶(300余个)的金属辅基
a. Na-K ATP酶。促进Na, K离子转运(3Na/2K) 静息电位、动作电位的基础 b. 其它多种与肝脏生化反应有关的酶
 静息电位、动作电位的基础. b. 其它多种与肝脏生化反应有关的酶.")
66
门冬氨酸钾镁的应用机理(1) 1、 激活和恢复毛细胆管膜上受胆汁酸抑制的Na+-K+ATP酶的活性 Mg++
胆汁郁积细胞功能

67
门冬氨酸钾镁的应用机理(2) 2、 激活三羧酸循环和苹果酸穿梭系统, 提供ATP
 2、 激活三羧酸循环和苹果酸穿梭系统, 提供ATP")
68
门冬氨酸钾镁的应用机理(2) 2、 激活三羧酸循环和苹果酸穿梭系统, 提供ATP
 2、 激活三羧酸循环和苹果酸穿梭系统, 提供ATP")
69
门冬氨酸钾镁的应用机理(3) 3、 促进鸟氨酸循环, 增加尿素合成, 解氨毒 鸟氨酸瓜氨酸 门冬氨酸 精氨酸代琥珀酸 草酰乙酸
鸟氨酸瓜氨酸 门冬氨酸 精氨酸代琥珀酸 草酰乙酸 尿素+H2O 精氨酸 延胡索酸

70
门冬氨酸钾镁的应用机理(4) 4、 激活核酸和蛋白质合成, 促进肝细胞再生和修复
 4、 激活核酸和蛋白质合成, 促进肝细胞再生和修复")
71
门冬氨酸钾镁的应用机理(5) 5、 激发肝糖原的合成和脂肪酸的-氧化, 保护肝细胞
 5、 激发肝糖原的合成和脂肪酸的-氧化, 保护肝细胞")
72
门冬氨酸钾镁的应用机理(6) 综合作用!
 综合作用!")
73
门冬氨酸钾镁 在治疗肝病中的临床应用 1、退黄疸 2、急性肝炎 3、慢性肝炎 4、肝硬化, 并发肝昏迷 5、脂肪肝

74
331例肝病治疗药物选择

75
黄胆型肝炎症状和生化改善(236例) (基本治疗:垂盆草糖浆,肝炎灵,Vit. C, 益肝灵)
 (基本治疗:垂盆草糖浆,肝炎灵,Vit. C, 益肝灵)")
76
黄胆型肝炎症状和生化改善(236例) (基本治疗:垂盆草糖浆,肝炎灵,Vit. C, 益肝灵)
 (基本治疗:垂盆草糖浆,肝炎灵,Vit. C, 益肝灵)")
77
谢谢!

Similar presentations
 28.1 2腦血管疾病9.3 3心臟疾病9.1 4糖尿病7.2 5事故傷害5.9 6肺炎4.0 7 慢性肝病及肝硬化 (5,049.>")
家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")





 基因结构: 基因结构: 5’- 非编码区5’- 非编码区 编码区 编码区 3’- 非编码区3’- 非编码区 HAV 疫苗研究近况.>")




>")


>")



