Download presentation
Presentation is loading. Please wait.

1
Department of Arrhythmias, Lund University Hospital, Sweden
房颤病人磁导航下肺静脉前庭部消融 Antrum Ablation under Stereotaxis System in Patients with Atrial Fibillation Shiwen Yuan, MD, PhD, FESC Department of Arrhythmias, Lund University Hospital, Sweden

2
磁导航系统和X线机位于工作位置

3
磁导航射频消融技术: 使用磁场力精确操纵极柔软的导管进行心脏标测和消融治疗的一项成熟的技术 全球28个国家, >60000? 例的临床应用 在国内:10家医院, > 170 例的临床应用 主要特点: 1. 安全,并发症低 2. 射线量低 3 . 学习曲线短 4. 导管操纵精确,可用于各种心律失常的消融治疗 5 .在房颤,房速,室速,心脏外科术后病人等复杂心律失常的治疗中最具优势

4
Lund大学附属医院于2011年9月13日开始使用磁导航
2012年8月升级为Epoch,双V-drive臂系统 两年半的时间里共在磁导航下500多例手术

5
肺静脉前庭部消融 (Antrum ablation)
肺静脉电隔离-Primary endpoint ( 在 2007和2012的两个版本HRS/EHRA/ECAS的专家共识文件中被认定为Cornerstone) 主要依据: Bordeaux的早期经验:肺静脉内的快速触发灶 Hamborg的经验:所有复发病例都有心房至肺静脉传导的再通,再隔离明显增加成功率 双侧肺移植长期无房颤 大约15年世界范围PVI的临床经验: 60-80%的治愈率
 主要依据: Bordeaux的早期经验:肺静脉内的快速触发灶. Hamborg的经验:所有复发病例都有心房至肺静脉传导的再通,再隔离明显增加成功率. 双侧肺移植长期无房颤. 大约15年世界范围PVI的临床经验: 60-80%的治愈率.")
6
Focal triggers/driver tachycardias within the PVs
Diagram of the Sites of 69 Foci Triggering Atrial Fibrillation in 45 Patients. Note the clustering in the pulmonary veins, particularly in both superior pulmonary veins Haissaguerre et al. N Engl J Med 1998; 39:659-66).
.")
7
挑战PVI方法作为金标准的临床资料 莱比锡经验 (外科线性消融,瘢痕区导管线性消融) CFAE消融 GP消融 PV外的房速灶, Rotors PV前庭部放射状线消融(国内文章) 房颤消融后PV传导再通与房颤复发无明显关系(国内文章)
 房颤消融后PV传导再通与房颤复发无明显关系(国内文章) .")
8
非PVI方法有效的证据: 莱比锡经验:无PVI,仅外科线形消融有效率>90% (95-97%) Kottkamp et al. JACC 2002, 40 (3): 475–480 近年来在会议报告,使用导管贯穿消融左房瘢痕区,不隔离肺静脉,房颤治愈率高达100%
: 475–480. 近年来在会议报告,使用导管贯穿消融左房瘢痕区,不隔离肺静脉,房颤治愈率高达100% .")
9
非PVI方法有效的证据: (A) failure of external and internal cardioversion (B) Voltage mapping with intracardiac recordings before and after ablations. CFAE largely on the posterior LA, annulus, and septum. (C+D) The atrial activation was 115 ms earlier than the P wave and ablation here terminated AF. CFAE-ablation:Nademanee K, et al. J Am Coll Cardiol 2004; 43:
 failure of external and internal cardioversion (B) Voltage mapping with intracardiac recordings before and after ablations. CFAE largely on the posterior LA, annulus, and septum. (C+D) The atrial activation was 115 ms earlier than the P wave and ablation here terminated AF. CFAE-ablation:Nademanee K, et al. J Am Coll Cardiol 2004; 43:")
10
非PVI方法有效的证据: PVI+Rotor 消融明显好于单纯PVI (82.4% vs. 44.9%)
(A) failure of external and internal cardioversion (B) Voltage mapping with intracardiac recordings before and after ablations. CFAE largely on the posterior LA, annulus, and septum. (C+D) The atrial activation was 115 ms earlier than the P wave and ablation here terminated AF. PVI+Rotor 消融明显好于单纯PVI (82.4% vs. 44.9%) Narayan et al. J Am Coll Cardiol 2012; 60(7):
 failure of external and internal cardioversion (B) Voltage mapping with intracardiac recordings before and after ablations. CFAE largely on the posterior LA, annulus, and septum. (C+D) The atrial activation was 115 ms earlier than the P wave and ablation here terminated AF. PVI+Rotor 消融明显好于单纯PVI (82.4% vs. 44.9%) Narayan et al. J Am Coll Cardiol 2012; 60(7):")
11
非PVI方法有效的证据: 肺静脉前庭部放射线装消融 (86%, n=42 vs. 59%, n=44) Zhao et al. Circ Arrhythm Electrophysiol. 2013; 6(2):310-7. .

12
非PVI方法有效的证据: 房颤消融后32例中有29例(90.6%)PV传导再通, 但无临床房颤复发。 传导再通发生率和复发组没有明显区别。 No recurrence with re-conduction: 29 of 32 (90.6%), 10/32 (31.2%) in all 4 veins, no significant differences with patients with recurrence Conclusion: sustained PV isolation may not be required for freedom from clinical recurrence of AF. Jiang RH et al. Heart Rhythm 2014; 11:969
, 10/32 (31.2%) in all 4 veins, no significant differences with patients with recurrence. Conclusion: sustained PV isolation may not be required for freedom from clinical recurrence of AF. Jiang RH et al. Heart Rhythm 2014; 11:969.")
13
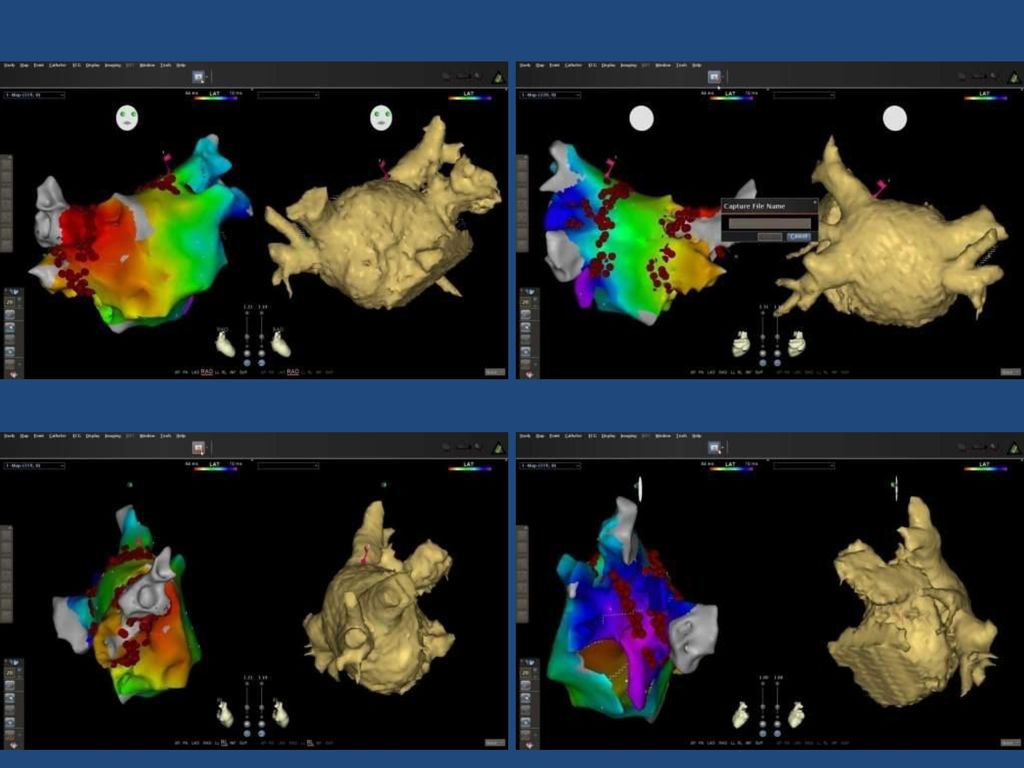
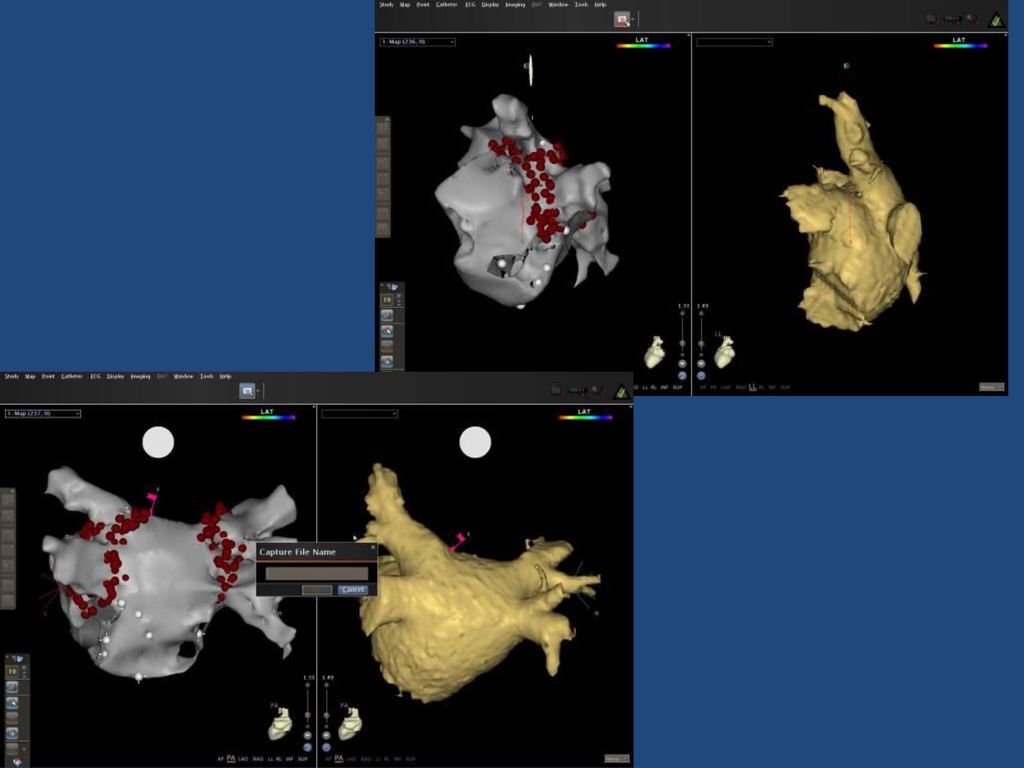
肺静脉前庭部消融 Antrum ablation
我们的设想和目标:通过肺静脉前庭部宽带消融 消除/阻断/损伤 肺静脉前庭区的触发灶,折返环,神经节, Marshall韧带。。。

14
肺静脉前庭部消融 Antrum ablation, 具体做法
参照CT/MR3维图像,用自动标测功能准确重建肺静脉前庭部解剖 常规使用 V-drive, (术中无照影) 肺静脉前庭部消融,以消融带上和消融区内无电信号为终点。早期使用Lasso在线验证,现停用。不做起搏验证。 持续房颤病人:肺静脉前庭部消融 + roof line + CFAE-消融 二次手术 (Redo cases): 肺静脉前庭部细致标测 (Condensed mapping) 补充前庭部消融,消融带上/内无信号为终点 Roof line CFAE-消融 (自发或诱发房颤)
 肺静脉前庭部消融,以消融带上和消融区内无电信号为终点。早期使用Lasso在线验证,现停用。不做起搏验证。 持续房颤病人:肺静脉前庭部消融 + roof line + CFAE-消融. 二次手术 (Redo cases): 肺静脉前庭部细致标测 (Condensed mapping) 补充前庭部消融,消融带上/内无信号为终点. Roof line. CFAE-消融 (自发或诱发房颤)")
15
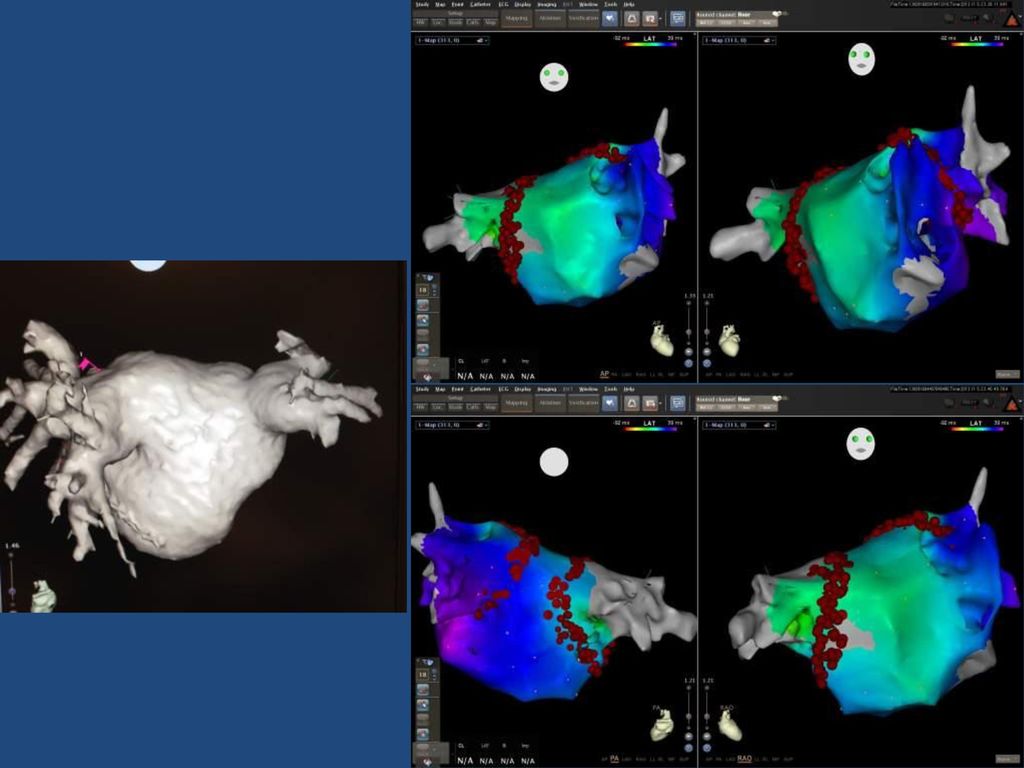
肺静脉前庭部消融 Antrum ablation
RF输出:前壁35-45W, 后壁30-35W, 视信号减低速度调整。 女性一般均减少5W。 冷盐水灌流:2 ml / 17 ml 每个消融点停留15-30秒,信号消失或减低>75%后移动 信号不消失时加强输出,并在消融点前后左右加强 左心耳和肺静脉间嵴部(ridge)双线(心耳侧+肺静脉侧),其余部位宽消融线约5-10 mm,上下肺静脉间点/线消融
双线(心耳侧+肺静脉侧),其余部位宽消融线约5-10 mm,上下肺静脉间点/线消融.")
16
左心耳和左侧肺静脉之间是一个尖锐狭长的界嵴, 其间有强大和错综复杂的肌纤维束,ligment of marshall, 神经结等等和房颤发生/持续有关的重要结构。
Ho SY et al, Circ arrhythm electrophysiol 2012; 5:220-8

17
肺静脉前庭部消融 Antrum ablation
肺静脉前庭部有错综复杂的肌纤维连接,在上下肺静脉之间肌纤维走向有大更变异。*植物神经节 Ho SY et al, Circ arrhythm electrophysiol 2012; 5:220-8

18
肺静脉前庭部消融 Antrum ablation
肺静脉前庭部错综复杂的肌纤维走向 ,在左心耳和左侧肺静脉之间有强大的肌束。 Ho SY et al, Circ arrhythm electrophysiol 2012; 5:220-8

23
Afib 4 Afib case 4

24
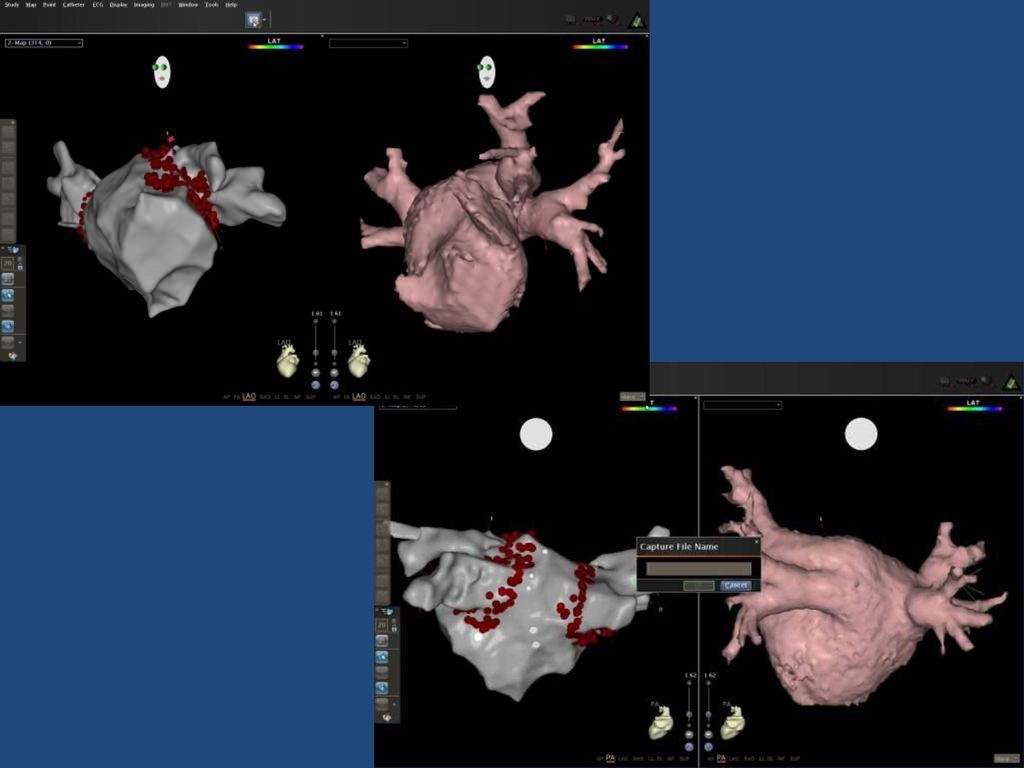
Redo case

25
Redo 2

26
Redo 3

27
对比观察 2013年以来有随访资料的磁导航手术125例 (阵发房颤95,持续16,长期持续3, 房颤+房速12)
消融带及消融区内无信号为终点 同期的手动消融83例(阵发房颤52,持续18,长期持续8, 房颤加房速5) CARTO+Lasso, 肺静脉电隔离为终点 随访时间平均 /- 4.9 月 不包括二次手术病例 (两组随访期内二次手术手41例, 26例有随访资料) 治愈:停药下长时间Holter无房颤,无症状 临床治愈: 未停药下无房颤,或Holter有短阵房颤但病人无感知 改善: AF↓80%, 病人症状改善 ≥ 8 (共11级) 无效
 CARTO+Lasso, 肺静脉电隔离为终点. 随访时间平均 /- 4.9 月. 不包括二次手术病例. (两组随访期内二次手术手41例, 26例有随访资料) 治愈:停药下长时间Holter无房颤,无症状. 临床治愈: 未停药下无房颤,或Holter有短阵房颤但病人无感知. 改善: AF↓80%, 病人症状改善 ≥ 8 (共11级) 无效.")
28
对比观察结果 NIOBE, n=125 (27 with Lasso, 98 without) CARTO/Navx-Manuell
No AF, no AA 52 (41.6%) 29 (35%) Clinically cured 25 (20%),共61.6%临床治愈 16 (19.3%),共54.3%临床治愈 Clinically improved 14 (11.2%),共72.8%有效 6 (7.2%),共61.5%有效 No effect/AT 34 (27.2%) 32 (38.5) % Total RF, 10,000J Procedure time,min 209+34 198+47 X-ray time,min X-ray dose, mc Gy/cm2 Major Complications 1 pericardial effusion 3 tamponades
 29 (35%) Clinically cured. 25 (20%),共61.6%临床治愈. 16 (19.3%),共54.3%临床治愈. Clinically improved. 14 (11.2%),共72.8%有效. 6 (7.2%),共61.5%有效. No effect/AT. 34 (27.2%) 32 (38.5) % Total RF, 10,000J Procedure time,min X-ray time,min X-ray dose, mc Gy/cm Major Complications. 1 pericardial effusion. 3 tamponades.")
29
总结 肺静脉内的触发灶并非房颤的唯一致病因素,因此肺静脉电隔离不是唯一有效的治疗途径。
肺静脉前庭部的折返活动及其消除,对房颤的终止和预防也有很重要的作用。 磁导航的应用可以准确重建肺静脉前庭部解剖。 肺静脉前庭部宽带消融可以同时实现肺静脉电隔离和前庭部折返活动的消除。 和单纯肺静脉电隔离相比,肺静脉前庭部宽带消融可望提高房颤消融的疗效。

30
谢谢大家!

Similar presentations





 几乎所有心衰者均可记录到室性心律失常 (Holter) 多形、成对室早 87% (PVCs) 多形、成对室早 87% (PVCs) 非持续性室速 54% (NSVT) 非持续性室速 54%>")


 10070 大米粥一碗 (500g) 100400 面条一碗 (170g) 100 70( 汤另计 ) 蒸蛋糕一碗 (170g) 5025 藕粉 50210 牛奶 10087.>")

 105 年 5 月 15 日(日) 08:20- 08:30 考試說明 08:20- 08:30 考試說明 08:30- 09:40 社 會 08:30- 09:40 自 然 09:40- 10:20 休息 09:40->")








