Download presentation
1
北京世纪坛医院 北京大学第九临床医学院 杨水祥
心肾综合症:新概念新进展 Prevention and treatment of Cardio-Renal Syndrome: New Concepts and Updates 北京世纪坛医院 北京大学第九临床医学院 杨水祥

2
心肾交互影响 慢性心衰往往被肾功能不全复杂化;急性失代偿性心衰往往因肾功能恶化或利尿剂抵抗预后更差。
心肾综合征(CRS)可能涉及一系列的神经内分泌紊乱及肾稳态调节机制不良。 心肾综合征的发病和治疗需要我们更多的关注。
可能涉及一系列的神经内分泌紊乱及肾稳态调节机制不良。 心肾综合征的发病和治疗需要我们更多的关注。")
3
CRS的定义 2008年欧洲学者将CRS划分为5个亚型: 2010年提出了新的定义

4
CRS2010年的定义及分型

5
1型CRS

6
2型CRS

7
3型CRS

8
4型CRS

9
5型CRS

10
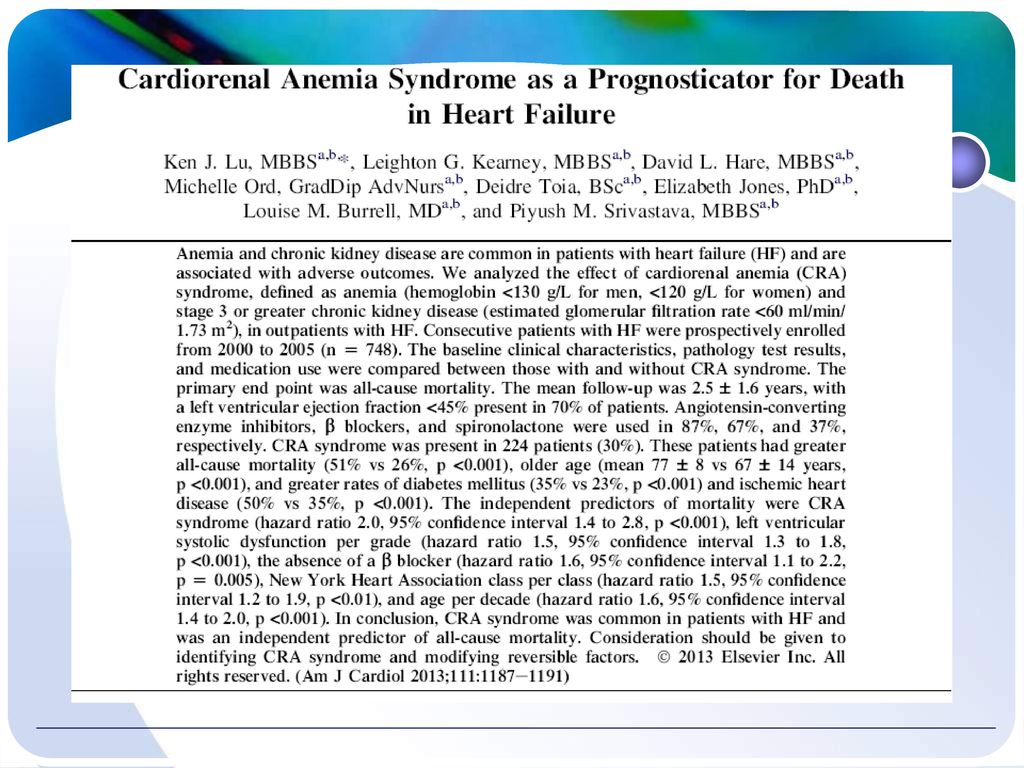
肾功能不全或肾脏疾病已成为慢性心衰或ADHF预后不良的一个独立预测指标。
左心室功能障碍预防和治疗回顾分析研究(SOLVD)提示,中度肾功能不全(肌酐清除率小于60毫升/分钟)与心衰住院的全因死亡率和复合终点死亡独立相关,对心衰的严重程度和合并的多元因素调整之后仍然明显相关。
提示,中度肾功能不全(肌酐清除率小于60毫升/分钟)与心衰住院的全因死亡率和复合终点死亡独立相关,对心衰的严重程度和合并的多元因素调整之后仍然明显相关。")
11
Smith GL等对16项80000万例患者 评价肾功能不全影响心力衰竭结果的研究进行的荟萃分析表明带给我们一些启示。
肾功能不全的严重程度与逐步增加的死亡率呈正相关 血肌酐每递增1毫克/分升则死亡风险增加33% 肾小球滤过率每递减10毫升/分钟则死亡风险上升7%

12
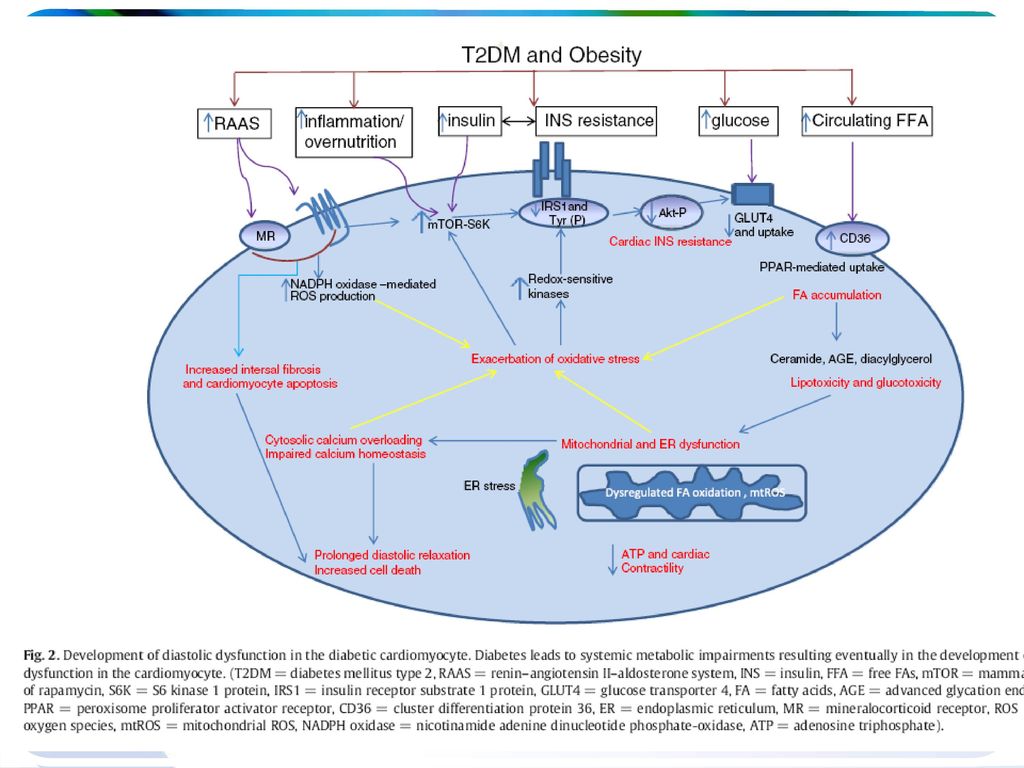
新概念的提出 心肾贫血综合征 心肾代谢综合征
新概念的提出 心肾贫血综合征 心肾代谢综合征

18
CRS的流行病学

19
CRS的流行病学

20
CRS1型较常见,在急性失代偿性心衰和急性冠脉综合征(ACS)患者中,急性肾损伤(AKI)的发生率分别约为24%~45%和9%~19%。
CRS2型患者,在ARCSCH研究中,随访9.3年,34%心血管疾病(CVD)患者的肾功能下降[肾小球滤过率(eGFR)下降幅度≥15 ml/(min·1.73m2)],其中5.6%的患者出现新发肾脏病。
患者的肾功能下降[肾小球滤过率(eGFR)下降幅度≥15 ml/(min·1.73m2)],其中5.6%的患者出现新发肾脏病。")
21
CRS3型的常见原因,包括对比剂所致急性肾损伤(CI-AKI)、药物诱导的肾病、心脏及非心脏大手术后AKI等。
CRS4型,美国健康营养调查研究(NHANES Ⅱ)显示,当患者eGFR≥90 ml/(min·1.73m2)、70~89 ml/(min·1.73m2)和 <70 ml/(min·1.73m2)时,其CVD的发生率分别为4.5%、7.9%和12.9%。该结果及数项研究提示,CKD可加速CVD的发生风险。 尚缺乏CRS5型的流行病和病理生理机制研究。
显示,当患者eGFR≥90 ml/(min·1.73m2)、70~89 ml/(min·1.73m2)和 <70 ml/(min·1.73m2)时,其CVD的发生率分别为4.5%、7.9%和12.9%。该结果及数项研究提示,CKD可加速CVD的发生风险。 尚缺乏CRS5型的流行病和病理生理机制研究。")
22
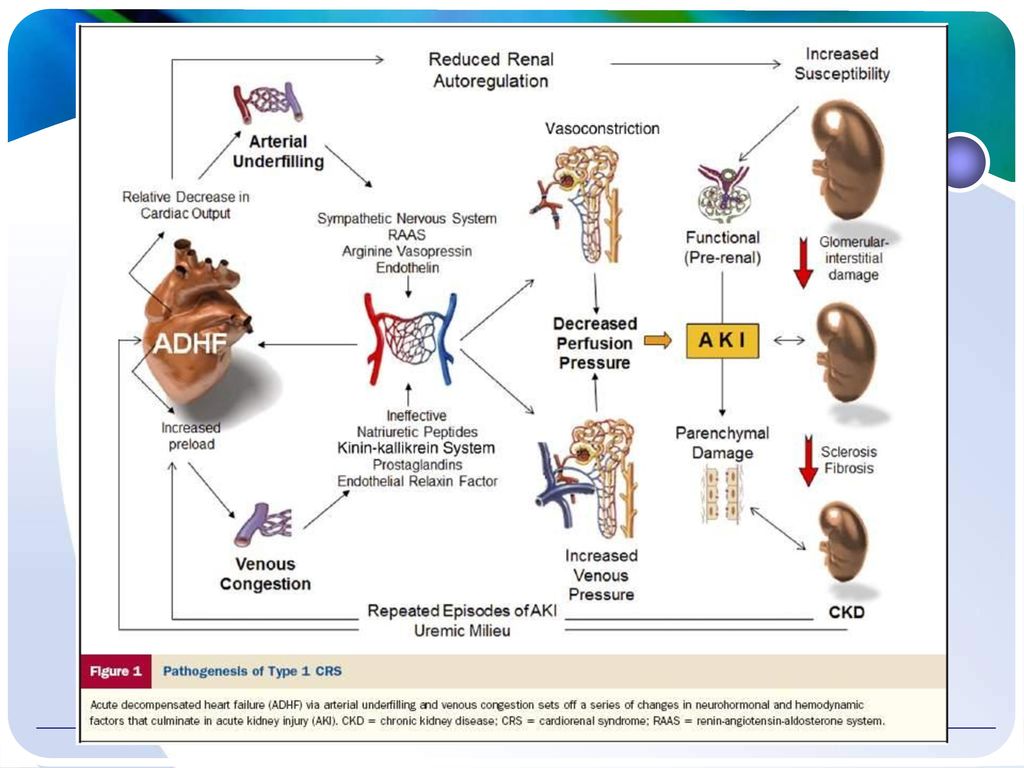
CRS的发病机制

24
Cardiorenal Interaction
Figure 1. Cardiorenal interaction and stage classification in the initiation and progression of chronic kidney disease and heart failure [1] and [11]. CVD, cardiovascular disease; HF, heart failure; GFR, glomerular filtration rate. Figure 1. Cardiorenal interaction and stage classification in the initiation and progression of chronic kidney disease and heart failure [1] and [11]. CVD, cardiovascular disease; HF, heart failure; GFR, glomerular filtration rate.

25
SNS激活 增加全身血管阻力、儿茶酚胺释放和直接神元刺激,增加肾脏肾素释放; 可进一步降低压力感受器反射调节的敏感性。
导致血管紧张素Ⅱ释放增多,血管收缩,肾出球小动脉收缩,心脏重塑及醛固酮释放增加,水钠滁留和促进心肌纤维化。

26
血管紧张素系统激活,血流动力学改变 精氨酸加压素的释放导致血管收缩,水滁留和低钠血症。 心房钠尿肽(心钠素和B型利钠肽)释放,健康人钠尿肽可以减轻血管紧张素系统和SNS激活所致的调节失衡,但心力衰竭时的长期释放可出现钠尿肽抵抗。 肾功能障碍和高血压控制不良也促进醛固酮释放,从而促进心衰发展。

27
Heart-kidney interactions

28
CRS的早期诊断(biomarker)
")
29
CRS的早期诊断(biomarker)
")
33
A Prospective, Blinded Study of Bioimpedance Vector Analysis and Biomarker Testing for the Prediction of Worsening Renal Function in Consecutive Patients with Acutely Decompensated Heart Failure: Primary Results of the Biomonitoring and Cardiorenal Syndrome in Heart Failure (BIONICS-HF) Trial
 Trial")
34
Independent role of high central venous pressure in predicting worsening of renal function in chronic heart failure outpatients

35
CRS的预防

36
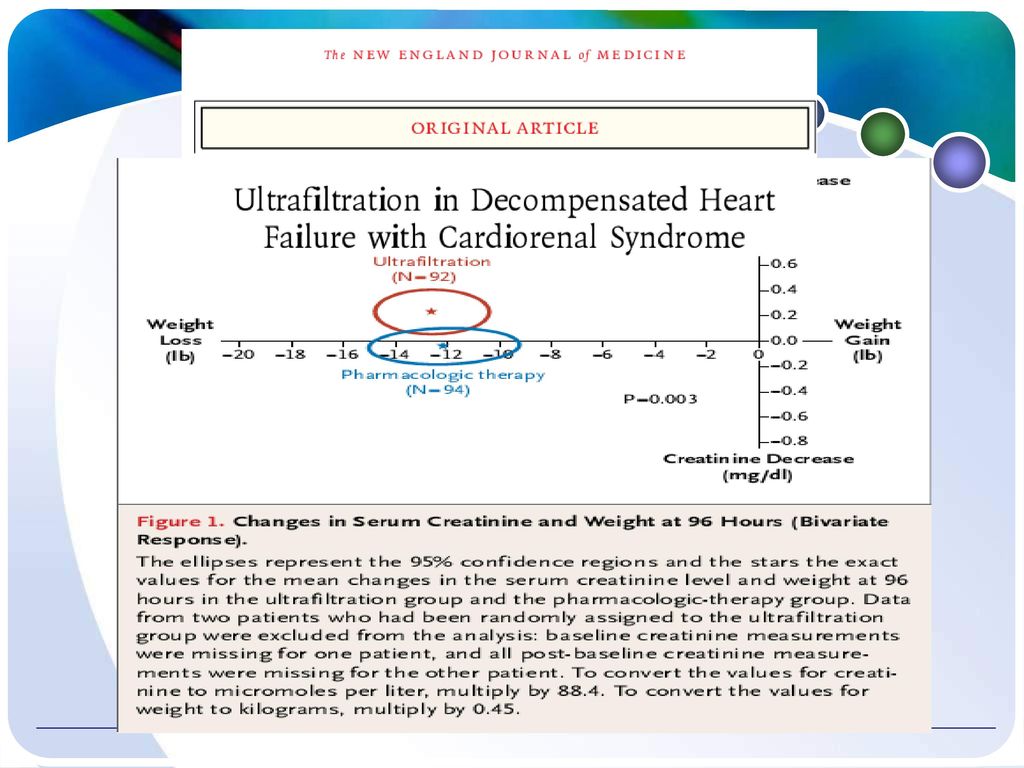
CRS的治疗 利尿剂抵抗治疗 (正/负)性肌力药物治疗 超滤 Treatment 奈西立肽 腺苷受体拮抗剂 加压素(抗利尿激素)拮抗剂
性肌力药物治疗 超滤 Treatment 奈西立肽 腺苷受体拮抗剂 加压素(抗利尿激素)拮抗剂")
37
Potential Effects of Digoxin on Long-Term Renal and Clinical Outcomes in Chronic Heart Failure

38
Fig. 2. Adjusted survival curves grouped by randomization to digoxin or placebo and subsequent improved renal function (IRF) status, in patients with a serum digoxin level #0.8 ng/mL. IRF defined as $20% improvement in estimated glomerular filtration rate (eGFR) from randomization to 1 year. Covariates adjusted for: age, race, ejection fraction, heart rate, systolic blood pressure, New York Heart Association functional class, diabetes, baseline use of digoxin, hydralazine, nitrates, diuretics, or angiotensin-converting enzyme inhibitors, physical examination findings, cardiothoracic ratio, and baseline eGFR. Overall between-group differences: P Comparisons of the Yes IRF/Yes Digoxin (n 5 58) and the No IRF/No Digoxin group (n 5 409; P ), No IRF/Yes Digoxin (n 5 213; P ), and Yes IRF/No Digoxin (n 5 60; P ) groups were all statistically significant.
 status, in patients with a serum digoxin level #0.8 ng/mL. IRF defined as $20% improvement in estimated glomerular filtration rate (eGFR) from randomization to 1 year. Covariates adjusted for: age, race, ejection fraction, heart rate, systolic blood pressure, New York Heart Association functional class, diabetes, baseline use of digoxin, hydralazine, nitrates, diuretics, or angiotensin-converting enzyme inhibitors, physical examination findings, cardiothoracic ratio, and baseline eGFR. Overall between-group differences: P Comparisons of the Yes IRF/Yes Digoxin (n 5 58) and the No IRF/No Digoxin group (n 5 409; P ), No IRF/Yes Digoxin (n 5 213; P ), and Yes IRF/No Digoxin (n 5 60; P ) groups were all statistically significant..")
39
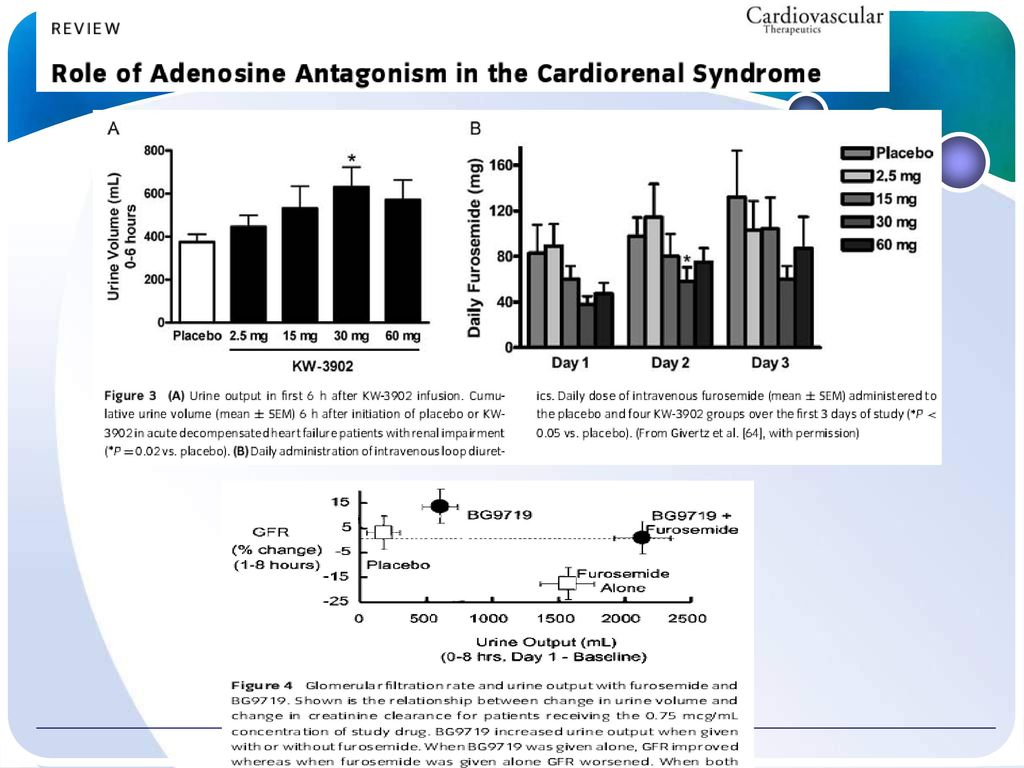
CRS的最新治疗药物 最新治疗药物 腺苷受 体拮抗 剂rolo fylline 加压素 (抗利 尿激素 ,AVP) 拮抗剂
 拮抗剂")
42
Ultrafiltration Figure 1. Water and solute transport in IU. Water molecules cross semipermeable membranes by UF, that is, a fluid shift driven by a hydrostatic pressure difference (TMP), according to the formula: Hourly fluid removal in IU=TMP×KUFwhere KUF is the UF coefficient of the filter, that is, the intrinsic permeability of the membrane. It represents the theoretical amount of plasma water transported in the unit of time per unit of TMP applied across the membrane (mL/mm Hg per hour). For example, given a filter KUF of 10 mL/mm Hg per hour, if TMP is 150 mm Hg, the maximum ultrafiltrate volume in 1 hour (hourly UF rate) will be 150 × 10 = 1.5 L. Hourly UF rate is directly set on the machine that modulates TMP according to the programmed weight loss. Solutes are dragged along with plasma water across the membrane (solvent drag: solutes with molecular size lower than membrane pores are transported with the solvent) (B). Urea (60 D) or electrolytes (sodium 23 D and potassium 35 D) will be moved easily; on the contrary, high-molecular-weight solutes (eg, albumin D) will not undergo the solvent drag effect. TMP, Transmembrane pressure; D, Daltons.
, according to the formula: Hourly fluid removal in IU=TMP×KUFwhere KUF is the UF coefficient of the filter, that is, the intrinsic permeability of the membrane. It represents the theoretical amount of plasma water transported in the unit of time per unit of TMP applied across the membrane (mL/mm Hg per hour). For example, given a filter KUF of 10 mL/mm Hg per hour, if TMP is 150 mm Hg, the maximum ultrafiltrate volume in 1 hour (hourly UF rate) will be 150 × 10 = 1.5 L. Hourly UF rate is directly set on the machine that modulates TMP according to the programmed weight loss. Solutes are dragged along with plasma water across the membrane (solvent drag: solutes with molecular size lower than membrane pores are transported with the solvent) (B). Urea (60 D) or electrolytes (sodium 23 D and potassium 35 D) will be moved easily; on the contrary, high-molecular-weight solutes (eg, albumin D) will not undergo the solvent drag effect. TMP, Transmembrane pressure; D, Daltons.")
44
Nesiritide奈西立肽 recombinant human B-type natriuretic
peptide (BNP), acts at the natriuretic peptide A receptor (NPR-A) to decrease preload, afterload, and PCWP, increase CO, increase urine output, and improve diastolic function. Adverse effects include headache and hypotension.
, acts at the natriuretic peptide A receptor (NPR-A) to decrease preload, afterload, and PCWP, increase CO, increase urine output, and improve diastolic function. Adverse effects include headache and. hypotension.")
46
Carperitide 卡培立肽 Carperitide, or A-type natriuretic peptide (ANP),
acts as a stronger agonist than BNP at NPR-A. Its hemodynamic effects are similar to those of nesiritide, Although it has more robust natriuretic and diuretic effects that are more pronounced in healthy subjects than in patients with HF. It increases and decreases MAP and PCWP, and its most common adverse effect is hypotension.

47
Urodilatin肾钠素 Ularitide, the product of differential processing
of the pro-ANP precursor in the kidney, acts on NPR-A in the collecting duct thereby increasing excretion of water and sodium. it decreased PCWP, decreased MAP, and increased CI, while down-regulating the RAAS and improving renal sodium excretion in healthy volunteers. The most common adverse effect is dosedependent hypotension.

48
CD-NP CD-NP (or ‘‘cenderitide’’) is a chimeric NP
synthesized from C-type natriuretic peptide (CNP) and Dendroaspis natriuretic peptide (DNP). CNP originates from endothelial cells and activates NPR-B, resulting predominately in venodilation DNP was isolated from the green mamba snake and activates NPR-A, with effects similar to those of ANP and BNP By fusing the DNP tail to CNP, an NP is created that acts as a partial agonist of NPR-A and an agonist of NPR-B CD-NP decreases PCWP and causes natriuresis and diuresis without a significant decrease in MAP in animal models It significantly decreases Cr compared with furosemide in patients with stable to cause a dose-dependent decrease in SBP
 and Dendroaspis natriuretic peptide (DNP). CNP originates from endothelial cells and activates NPR-B, resulting predominately in venodilation. DNP was isolated from the green mamba snake and activates NPR-A, with effects similar to those of ANP and BNP. By fusing the DNP tail to CNP, an NP is created that acts as a partial agonist of NPR-A and an agonist of NPR-B. CD-NP decreases PCWP and causes natriuresis and diuresis without a significant decrease in MAP in animal models. It significantly decreases Cr compared with furosemide in patients with stable. to cause a dose-dependent decrease in SBP.")
49
Soluble Guanylyl Cyclase Agents
Cinaciguat. Cinaciguat (or BAY ) is an NO independent sGC activator that is effective Cinaciguat decreases diastolic blood pressure compared with placebo without significantly decreasing SBP, and in patients with ADHF it decreases PCWP and MAP and increases CO without significantly changing Cr. Dose-dependent hypotension is the most common adverse effect.
 is an NO independent sGC activator that is effective. Cinaciguat decreases diastolic blood pressure compared with placebo without significantly decreasing SBP, and in patients. with ADHF. it decreases PCWP and MAP and increases. CO without significantly changing Cr. Dose-dependent hypotension is the most common adverse effect.")
50
RAAS-Modifying Agents
Aliskiren阿利吉仑. Aliskiren is an oral direct renin inhibitor that blocks formation of angiotensin I and II without affecting kinin metabolism. decrease SVR and PCWP in patients with decompensated HF, Decreased N-terminal prohormone of BNP (NT-proBNP),plasma renin activity, and urinary aldosterone. Hyperkalemia,hypotension, and decreased renal function have been reported as adverse effects.
,plasma renin activity, and urinary aldosterone. Hyperkalemia,hypotension, and decreased renal function have been reported as adverse effects.")
51
Relaxin松弛素 Relaxin, the hormone responsible for many
of the maternal hemodynamic changes in pregnancy, acts as a systemic, renal, and coronary vasodilator in animalmodels decreasing afterload, increasing CO, and decreasing the risk of infarction during periods of myocardial ischemia. In humans with HF, relaxin levels were increased and correlated with disease severity it increased CI and decreased PCWP, NT-proBNP, and Cr. No adverse effects have been reported.

52
Hydralazine肼苯哒嗪 Hydralazine is a direct vasodilator with
an unknown mechanism of action that decreases afterload and improves stroke volume, increases renal blood flow and has a moderate direct inotropic effect. Adverse effects include hypotension, nausea, headache, and tachycardia.

53
总结 心肾交互影响 机制更为复杂,治疗更加困难 发病率越来越高,需要更多关注 交叉学科联手,防治心肾综合征

54
Thank You !







 Regulate fluid, electrolyte Acid-base balance 調整血壓:經由腎素體系進行調節。>")


家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")


 :非实验室工作人 员在实验室之外的化验检测 其他命名 : Near Patient Doctors Office Testing Extra Laboratory Testing Decentralised.>")





 河南中医学院第一附属医院 杜正光>")




