Download presentation
Presentation is loading. Please wait.

1
卫生技术评估在医用耗材管理中的应用 上海市第六人民医院 医学装备处 杨 海 2012年5月

3
杨 海 医学硕士、副研究员 中国医学装备协会管理专业委员会常务委员 上海医学会临床医学工程专科委员会医用耗材管理学组副组长
杨 海 医学硕士、副研究员 中国医学装备协会管理专业委员会常务委员 上海医学会临床医学工程专科委员会医用耗材管理学组副组长 上海市卫生局耗材招标采购专家 2000年上海中医药大学附属曙光医院科教处 2000年先后两次赴华西医科大学学习临床流行病学及循证医学 2001年—2004年在生物医药企业工作 2005年5月起上海市第六人民医院,分管医院医用耗材的采购及供应链管理 杨 海

4
论 著 标 题 刊物/专著 出版时间 出版社 医用耗材的循证管理 中国医疗器械杂志 2009年3月
论 著 标 题 刊物/专著 出版时间 出版社 医用耗材的循证管理 中国医疗器械杂志 2009年3月 非消毒包装植入性医疗器械追溯系统的优化方案 2009年7月 医用耗材定价中循证评价及经济学评价的作用 2010年5月 医用耗材数据资源利用 中国医疗设备 2011年5月 第五章 医院物资管理 医院管理学 第2版 后勤管理分册 2011年8月 人民卫生出版社 杨 海

5
医改形势下的医用耗材管理目标

6
保证本医疗机构的医、教、研工作及时使用到合法、安全、有效、适宜的医用耗材,并在此基础上不断追求患者费用合理,医院成本效益合理。
杨 海

7
选择适宜医疗耗材,合理控制费用

8
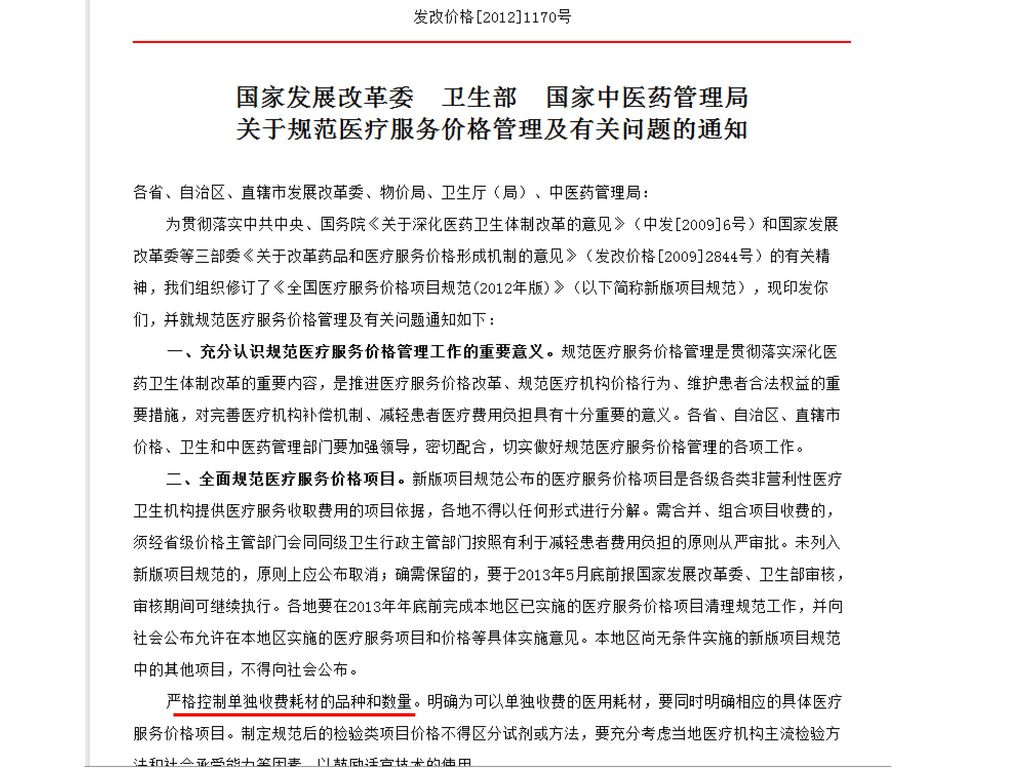
关于医药卫生体制改革的重要文件 2009年中共中央、国务院发布的《关于深化医药卫生体制改革的意见》
国务院发布的《医药卫生体制改革近期重点实施方案(2009—2011年)》 2011年卫生部等有关部门发布的《关于公立医院改革试点的指导意见》 2012年3月国务院印发的《“十二五”期间深化医药卫生体制改革规划暨实施方案》 杨 海
》 2011年卫生部等有关部门发布的《关于公立医院改革试点的指导意见》 2012年3月国务院印发的《 十二五 期间深化医药卫生体制改革规划暨实施方案》 杨 海")
9
中共中央 国务院《关于深化医药卫生体制改革的意见》2009年发布(摘要)
(三)总体目标:……为群众提供安全、有效、方便、价廉的医疗卫生服务。 (十一)建立科学合理的医药价格形成机制。 ……规范公立医疗机构收费项目和标准,研究探索按病种收费等收费方式改革。 ……加强医用耗材及植(介)入类医疗器械流通和使用环节价格的控制和管理。……积极探索建立医疗保险经办机构与医疗机构、药品供应商的谈判机制,发挥医疗保障对医疗服务和药品费用的制约作用. (十二)建立严格有效的医药卫生监管体制。 ……强化医疗保障对医疗服务的监控作用,完善支付制度,积极探索实行按人头付费、按病种付费、总额预付等方式…… 杨 海
总体目标:……为群众提供安全、有效、方便、价廉的医疗卫生服务。 (十一)建立科学合理的医药价格形成机制。 ……规范公立医疗机构收费项目和标准,研究探索按病种收费等收费方式改革。 ……加强医用耗材及植(介)入类医疗器械流通和使用环节价格的控制和管理。……积极探索建立医疗保险经办机构与医疗机构、药品供应商的谈判机制,发挥医疗保障对医疗服务和药品费用的制约作用. (十二)建立严格有效的医药卫生监管体制。 ……强化医疗保障对医疗服务的监控作用,完善支付制度,积极探索实行按人头付费、按病种付费、总额预付等方式…… 杨 海")
10
《医药卫生体制改革近期重点实施方案(2009—2011年)》国务院2009年发布(摘要)
一、加快推进基本医疗保障制度建设 (五)提高基本医疗保障管理服务水平。鼓励地方积极探索建立医保经办机构与医药服务提供方的谈判机制和付费方式改革,合理确定药品、医疗服务和医用材料支付标准,控制成本费用。 五、推进公立医院改革试点 (十七)改革公立医院管理体制、运行机制和监管机制。......规范公立医院临床检查、诊断、治疗、使用药物和植(介)入类医疗器械行为,优先使用基本药物和适宜技术...... (十八)推进公立医院补偿机制改革。逐步将公立医院补偿由服务收费、药品加成收入和财政补助三个渠道改为服务收费和财政补助两个渠道......推进医药分开,逐步取消药品加成,不得接受药品折扣......适当提高医疗技术服务价格,降低药品、医用耗材和大型设备检查价格......公立医院提供特需服务的比例不超过全部医疗服务的10%...... 杨 海
提高基本医疗保障管理服务水平。鼓励地方积极探索建立医保经办机构与医药服务提供方的谈判机制和付费方式改革,合理确定药品、医疗服务和医用材料支付标准,控制成本费用。 五、推进公立医院改革试点. (十七)改革公立医院管理体制、运行机制和监管机制。......规范公立医院临床检查、诊断、治疗、使用药物和植(介)入类医疗器械行为,优先使用基本药物和适宜技术 (十八)推进公立医院补偿机制改革。逐步将公立医院补偿由服务收费、药品加成收入和财政补助三个渠道改为服务收费和财政补助两个渠道......推进医药分开,逐步取消药品加成,不得接受药品折扣......适当提高医疗技术服务价格,降低药品、医用耗材和大型设备检查价格......公立医院提供特需服务的比例不超过全部医疗服务的10% 杨 海")
11
《“十二五”期间深化医药卫生体制改革规划暨实施方案》 国务院 2012年发布(摘要) :
三、加快健全全民医保体系(五)改革完善医保支付制度。加大医保支付方式改革力度,结合疾病临床路径实施,在全国范围内积极推行按病种付费、按人头付费、总额预付等,增强医保对医疗行为的激励约束作用。建立医保对统筹区域内医疗费用增长的制约机制,制定医保基金支出总体控制目标并分解到定点医疗机构,将医疗机构次均(病种)医疗费用增长控制和个人负担定额控制情况列入医保分级评价体系。积极推动建立医保经办机构与医疗机构、药品供应商的谈判机制和购买服务的付费机制。 五、积极推进公立医院改革 (二)推进补偿机制改革。……逐步取消药品加成政策,将公立医院补偿由服务收费、药品加成收入和财政补助三个渠道改为服务收费和财政补助两个渠道。医院的药品和高值医用耗材实行集中采购。...... (三)控制医疗费用增长。……强化医保对医疗服务的监控作用,采取总额预付、按人头、按病种付费等复合支付方式,引导医疗机构主动控制成本……严格基本医保药品目录使用率及自费药品控制率等指标考核。加强卫生部门对医疗费用的监管控制,将次均费用和总费用增长率、住院床日以及药占比等控制管理目标纳入公立医院目标管理责任制并作为绩效考核的重要指标,及时查处为追求经济利益的不合理用药、用材和检查及重复检查等行为…… 杨 海
改革完善医保支付制度。加大医保支付方式改革力度,结合疾病临床路径实施,在全国范围内积极推行按病种付费、按人头付费、总额预付等,增强医保对医疗行为的激励约束作用。建立医保对统筹区域内医疗费用增长的制约机制,制定医保基金支出总体控制目标并分解到定点医疗机构,将医疗机构次均(病种)医疗费用增长控制和个人负担定额控制情况列入医保分级评价体系。积极推动建立医保经办机构与医疗机构、药品供应商的谈判机制和购买服务的付费机制。 五、积极推进公立医院改革. (二)推进补偿机制改革。……逐步取消药品加成政策,将公立医院补偿由服务收费、药品加成收入和财政补助三个渠道改为服务收费和财政补助两个渠道。医院的药品和高值医用耗材实行集中采购。 (三)控制医疗费用增长。……强化医保对医疗服务的监控作用,采取总额预付、按人头、按病种付费等复合支付方式,引导医疗机构主动控制成本……严格基本医保药品目录使用率及自费药品控制率等指标考核。加强卫生部门对医疗费用的监管控制,将次均费用和总费用增长率、住院床日以及药占比等控制管理目标纳入公立医院目标管理责任制并作为绩效考核的重要指标,及时查处为追求经济利益的不合理用药、用材和检查及重复检查等行为…… 杨 海")
13
医疗机构为什么要控制医用耗材费用: 随着“以药补医”机制的取消,医用耗材对患者负担的影响将更加明显地显现出来
医用耗材也将逐步取消收费加成,将不再作为医院收入来源 大部分医用耗材将不能单独收费而成为医院的成本 植(介)入医疗器械即使能按成本收费,其使用也受到费用控制政策的压力 杨 海
入医疗器械即使能按成本收费,其使用也受到费用控制政策的压力. 杨 海")
14
单纯依靠集中采购(招标)能有效控制费用吗?
为什么招了标以后费用还是涨啊? 杨 海

15
总数量相同的金块和银块重量不同 杨 海

16
影响材料费用的各种因素及其相互关系 无证据的所谓优势 杨 海 liuyuanwuliu8257@163.com 费用 收费价 使用量 采购价
医院进销差 病种 手术方式 对新技术的探索 占据学术领先地位 技术领先性 / 市场独占性 真实的优势 虚假的优势 kickback 无证据的所谓优势 杨 海

17
造成医用耗材费用不合理增高的主要原因: 采购价过高 使用中的价格不均衡(贵的用得多,便宜的用得少甚至不用) 超适应证使用 进销差过大
可能是趋利行为 学科发展目的与基本医疗目的混淆 应进行分类管控:对于医院考虑支持的因学科发展目的使用的材料应有明确的适应证规范并及时总结 超适应证使用 进销差过大 杨 海

18
卫生技术评估简介 医疗评估(循证医学) 经济评估(成本效果、成本效用) 社会评估 道德评估
费用 收费价 使用量 采购价 医院进销差 病种 手术方式 对新技术的探索 占据学术领先地位 技术领先性 / 市场独占性 真实的优势 虚假的优势 kickback 无证据的所谓优势 杨 海

19
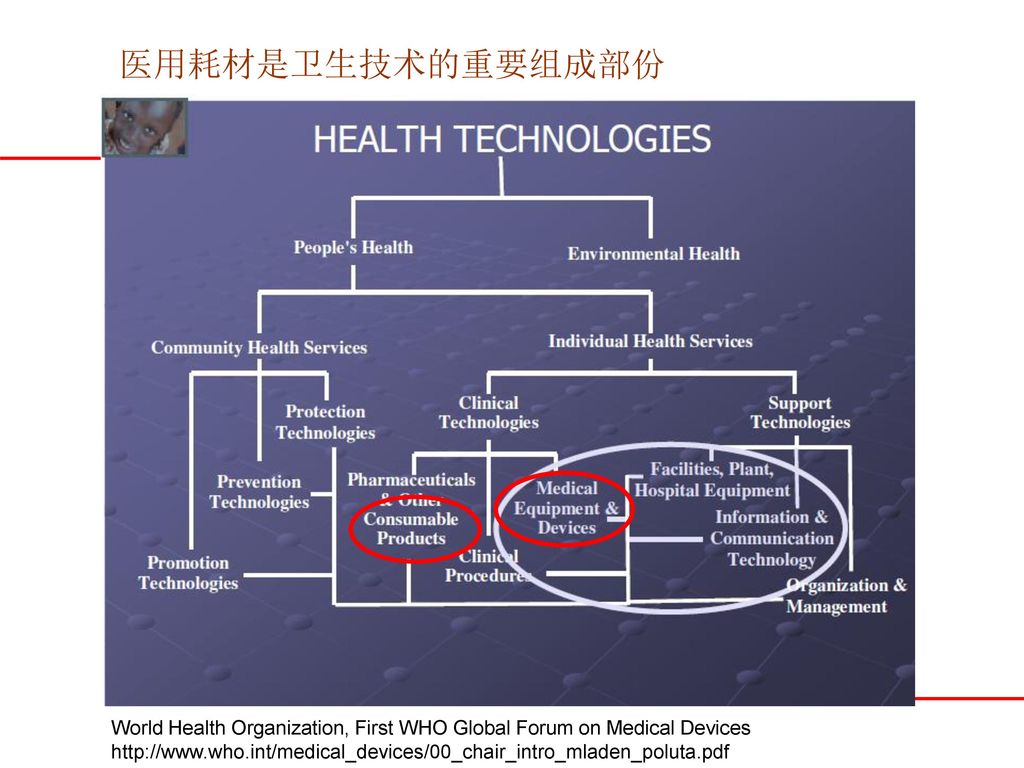
医用耗材是卫生技术的重要组成部份 World Health Organization, First WHO Global Forum on Medical Devices
20
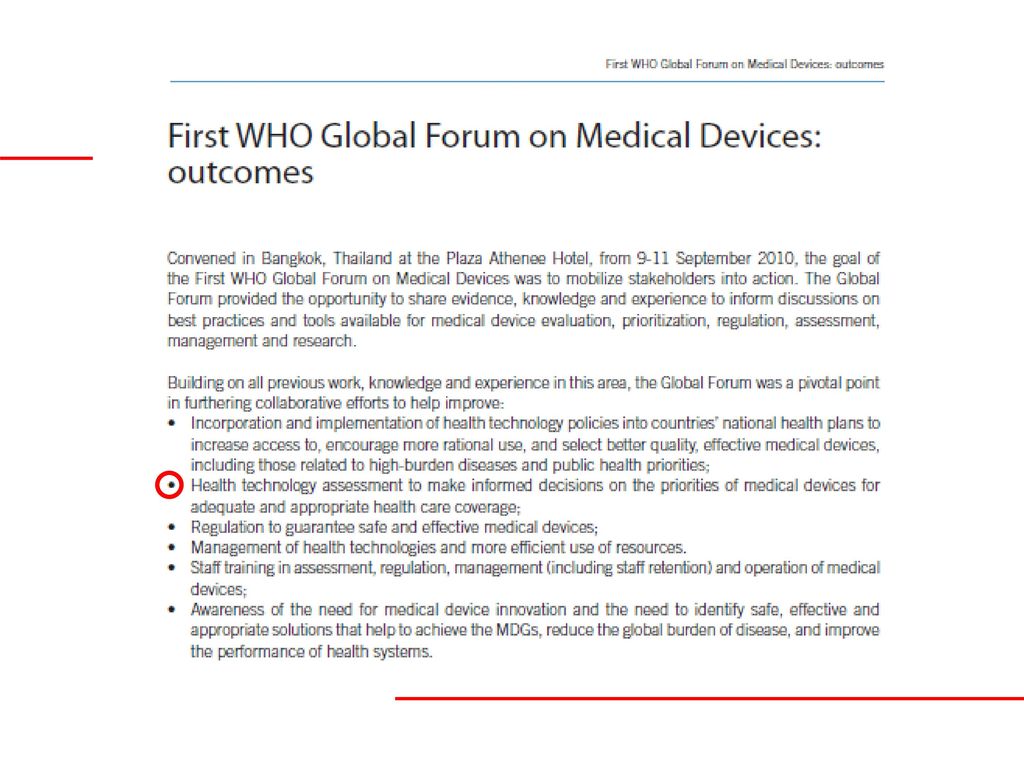
2007年WHO第六十届世界卫生大会提案及决议

21
第六十届世界卫生大会后WHO组织了多项关于医疗器械理性决策等方面的研究

27
——April 2011 MSAC application 1090.1 Assessment report
Review of interim funded service Artificial intervertebral disc replacement - lumbar ——April 2011 MSAC application Assessment report

28
Aim To assess the safety, effectiveness and cost-effectiveness of lumbar artificial intervertebral disc replacement (AIDR) for the treatment of patients suffering from significant axial back pain and/or radicular pain, secondary to disc degeneration or prolapse, who have failed nonoperative treatment. 杨 海
 for the treatment of patients suffering from significant axial back pain and/or radicular pain, secondary to disc degeneration or prolapse, who have failed nonoperative treatment. 杨 海")
29
Results and Conclusions Safety
A total of 43 studies were identified for inclusion in the assessment of the safety of lumbar AIDR. This included five comparative studies and 38 case series. Comparative studies compared lumbar AIDR with lumbar fusion procedures. Sample sizes ranged from 10 to 427 patients, with safety data reported for an overall total of 3,224 patients. For the majority of adverse events reported, there were no obvious differences in incidence rates between the lumbar AIDR and lumbar fusion groups, with two studies reporting no statistical differences in the rate of overall complications between the two groups. Wound infection was the most commonly reported adverse event, and demonstrated an incidence rate of 3.2 per cent in the lumbar AIDR population, and 5.1 per cent in the lumbar fusion population. Prosthesis-related adverse events were those relating to movement of the device, including collapse or subsidence (3%), and displacement (0.78%). Fusion-related adverse events included nonunion/pseudarthrosis (6.4%) and bone graft donor-site pain (11.1%). The rate of adjacent segment problems appeared higher following lumbar fusion (8.3%) compared with lumbar AIDR (1.3%). Major adverse events such as major vessel injury, and neurological damage including nerve root injury were rare in both the lumbar AIDR and fusion groups. There was one reported death following lumbar AIDR which was narcotic-related, while no deaths were reported following lumbar fusion. Overall, the safety of lumbar AIDR is comparable to that of lumbar fusion. It appears that the lumbar AIDR procedure is relatively safe, and is not associated with serious adverse events. 杨 海
, and displacement (0.78%). Fusion-related adverse events included nonunion/pseudarthrosis (6.4%) and bone graft donor-site pain (11.1%). The rate of adjacent segment problems appeared higher following lumbar fusion (8.3%) compared with lumbar AIDR (1.3%). Major adverse events such as major vessel injury, and neurological damage including nerve root injury were rare in both the lumbar AIDR and fusion groups. There was one reported death following lumbar AIDR which was narcotic-related, while no deaths were reported following lumbar fusion. Overall, the safety of lumbar AIDR is comparable to that of lumbar fusion. It appears that the lumbar AIDR procedure is relatively safe, and is not associated with serious adverse events. 杨 海")
30
Results and Conclusions Effectiveness
A total of 13 comparative studies were identified and included to inform on the comparative effectiveness of lumbar AIDR, including a total of four RCTs (comprising 12 studies) that compared lumbar AIDR to anterior lumbar interbody fusion (ALIF), circumferential fusion, or posterolateral fusion/posterior lumbar interbody fusion (PLF/PLIF), as well as one nonrandomised comparative study that compared lumbar AIDR to ALIF. All of the included comparative studies utilised the Owestry Disability Index (ODI), one of the principal condition-specific measures used in the management of spinal disorders, and the gold standard for assessing the extent to which a patient’s functional level is limited by low back pain. Three studies reported that patients in the lumbar AIDR group showed statistically greater improvements in ODI scores than lumbar fusion patients at various time points up to 1-year follow-up; however, none of the studies reported significant differences between the groups at 2- or 5-year follow-up. Similarly, two studies reported that at 2-year follow-up overall clinical success was significantly higher in the lumbar AIDR group compared with the lumbar fusion group, while the rate of reoperation was similar in both groups. In two studies, patient satisfaction at 2-year follow-up was significantly higher in lumbar AIDR patients compared with lumbar fusion patients, with up to 81 per cent of AIDR patients saying they would have the procedure again, compared with 69 per cent of fusion patients. This may have reflected the fact that lumbar AIDR patients experienced significantly less pain and required less narcotic medication, reported better sexual function, and returned to work at higher rates, when compared with lumbar fusion patients up to 2 years after surgery. Radiographic outcomes were reported in several studies; however, outcomes were reported differently across studies, and no statistical comparisons between the lumbar AIDR and lumbar fusion groups were reported, making it difficult to draw firm conclusions. Overall, in the short to medium term the effectiveness of lumbar AIDR, in terms of ODI scores, success of the procedure, pain, patient satisfaction, workstatus, quality of life and sexual function, appears to be comparable to lumbar fusion procedures. 杨 海
 that compared lumbar AIDR to anterior lumbar interbody fusion (ALIF), circumferential fusion, or posterolateral fusion/posterior lumbar interbody fusion (PLF/PLIF), as well as one nonrandomised comparative study that compared lumbar AIDR to ALIF. All of the included comparative studies utilised the Owestry Disability Index (ODI), one of the principal condition-specific measures used in the management of spinal disorders, and the gold standard for assessing the extent to which a patient’s functional level is limited by low back pain. Three studies reported that patients in the lumbar AIDR group showed statistically greater improvements in ODI scores than lumbar fusion patients at various time points up to 1-year follow-up; however, none of the studies reported significant differences between the groups at 2- or 5-year follow-up. Similarly, two studies reported that at 2-year follow-up overall clinical success was significantly higher in the lumbar AIDR group compared with the lumbar fusion group, while the rate of reoperation was similar in both groups. In two studies, patient satisfaction at 2-year follow-up was significantly higher in lumbar AIDR patients compared with lumbar fusion patients, with up to 81 per cent of AIDR patients saying they would have the procedure again, compared with 69 per cent of fusion patients. This may have reflected the fact that lumbar AIDR patients experienced significantly less pain and required less narcotic medication, reported better sexual function, and returned to work at higher rates, when compared with lumbar fusion patients up to 2 years after surgery. Radiographic outcomes were reported in several studies; however, outcomes were reported differently across studies, and no statistical comparisons between the lumbar AIDR and lumbar fusion groups were reported, making it difficult to draw firm conclusions. Overall, in the short to medium term the effectiveness of lumbar AIDR, in terms of ODI scores, success of the procedure, pain, patient satisfaction, workstatus, quality of life and sexual function, appears to be comparable to lumbar fusion procedures. 杨 海")
31
Results and Conclusions Cost-effectiveness
The incremental costs associated with each procedure demonstrate that compared to PLIF, combination and circumferential fusion, AIDR is cost saving. Compared to ALIF, AIDR is marginally more expensive. Overall, compared to the average fusion cost, AIDR represents a cost saving of $1,600 per patient. Overall the results were most sensitive to using the direct approach to apply utility weights, changes in the relative risk of overall or ODI success and the time in hospital with AIDR. The results were somewhat sensitive to the proportion of fusion patients requiring bone morphogenetic protein (BMP). When hospitalisation costs with AIDR were assumed to be equal to that with fusion, fusion became less costly compared to AIDR. If a direct approach were used to apply utility weights, the average QALYs gained with lumbar AIDR and PLIF/PLF was 1.25 QALYs and 1.16 QALYs, respectively. Thus QALYs experienced increased by 0.10 QALYs with lumbar AIDR compared to PLIF/PLF. Using this approach AIDR was estimated to be less costly and more effective compared to PLIF. While compared to PLF, AIDR was estimated to be more costly and more effective, and had an additional cost per QALY of $8,443. 杨 海
. When hospitalisation costs with AIDR were assumed to be equal to that with fusion, fusion became less costly compared to AIDR. If a direct approach were used to apply utility weights, the average QALYs gained with lumbar AIDR and PLIF/PLF was 1.25 QALYs and 1.16 QALYs, respectively. Thus QALYs experienced increased by 0.10 QALYs with lumbar AIDR compared to PLIF/PLF. Using this approach AIDR was estimated to be less costly and more effective compared to PLIF. While compared to PLF, AIDR was estimated to be more costly and more effective, and had an additional cost per QALY of $8,443. 杨 海")
32
Locking plate osteosynthesis in displaced 4-part fractures of the proximal humerus ——Stig Brorson Acta Orthopaedica 2011; 82 (4) Background and purpose There is considerable uncertainty about the optimal treatment of displaced 4-part fractures of the proximal humerus. Within the last decade, locking plate technology has been considered a breakthrough in the treatment of these complex injuries. Methods We systematically identified and reviewed clinical studies on the benefits and harms after osteosynthesis with locking plates in displaced 4-part fractures. Results We included 14 studies with 374 four-part fractures. There were 10 case series, 3 retrospective observational comparative studies, 1 prospective observational comparative study, and no randomized trials. Small studies with a high risk of bias precluded reliable estimates of functional outcome. High rates of complications (16–64%) and reoperations (11–27%) were reported. Interpretation The empirical foundation for the value of locking plates in displaced 4-part fractures of the proximal humerus is weak. We emphasize the need for well-conducted randomized trials and observational studies. 杨 海
 and reoperations (11–27%) were reported. Interpretation The empirical foundation for the value of locking plates in displaced 4-part fractures of the proximal humerus is weak. We emphasize the need for well-conducted randomized trials and observational studies. 杨 海")
33
A systematic review of locking plate fixation of proximal humerus fractures ——Robert C. Injury, Int. J. Care Injured 42 (2011) Purpose: Technique for the fixation of two, three, and four part proximal humerus fractures has rapidly shifted towards the use of specially contoured proximal humerus locking plates. The purpose of this study is to evaluate the short to medium term functional results and common complications associated with the fixation of proximal humerus fractures with locking plates. Methods: The PubMed and EMBASE databases were used to perform a systematic review of the English literature to assess the functional results and complications associated with proximal humerus locking plates. Our inclusion criteria were proximal humerus fracture due to trauma (excluding pathologic fractures), patients greater than 18 years of age, more than 15 patients in the study or subgroup of interest, at least 18 months follow-up, at least one relevant functional outcome score, and quality outcome score of at least 5/10. Studies that did not meet these criteria were excluded. All institutional, author, and journal information was concealed to minimize reviewer bias. Results: Twelve studies including 514 patients met the inclusion criteria. At most recent follow-up patients achieved a mean Constant score of 74 and a mean DASH score of 27. The overall rate of complications was 49% including varus malunion, 33% excluding varus malunion, and reoperation rate was 14%. The most common complications included varus malunion 16%, AVN 10%, screw perforation of the humeral head into the joint 8%, subacromial impingement 6%, and infection 4%. Discussion: Fixation of proximal humerus fractures with proximal humerus locking plates is associated with a high rate of complications and reoperation. Further study is needed to determine what technical errors and patient characteristics are risk factors for failure of this now common fixation technique. 杨 海
, patients greater than 18 years of age, more than 15 patients in the study or subgroup of interest, at least 18 months follow-up, at least one relevant functional outcome score, and quality outcome score of at least 5/10. Studies that did not meet these criteria were excluded. All institutional, author, and journal information was concealed to minimize reviewer bias. Results: Twelve studies including 514 patients met the inclusion criteria. At most recent follow-up patients achieved a mean Constant score of 74 and a mean DASH score of 27. The overall rate of complications was 49% including varus malunion, 33% excluding varus malunion, and reoperation rate was 14%. The most common complications included varus malunion 16%, AVN 10%, screw perforation of the humeral head into the joint 8%, subacromial impingement 6%, and infection 4%. Discussion: Fixation of proximal humerus fractures with proximal humerus locking plates is associated with a high rate of complications and reoperation. Further study is needed to determine what technical errors and patient characteristics are risk factors for failure of this now common fixation technique. 杨 海")
34
基于卫生技术评估的医用耗材采购价格控制 医用耗材 循证评价 有无真正优势? 竞标定价 无 有 供应商讨论会 文献调查 经济学评价
确定经竟标的基准品 CEA CEA结果+基准品价格 →单列产品的价格区间 临床专家意见 杨 海

35
基于卫生技术评估的医用耗材使用量控制 控制用量 本医疗机构现有 医疗器械(耗材) 目录 有无充分HTA证据证明其 “安全有效、成本较低”
基本器械目录 高端器械目录 有 无 用量不受控制 使用前 审批 控制用量 适应证承诺 及监测 限制比例 或数量 杨 海

36
过去这些年,我们的探索

37
非消毒包装植入性医疗器械追溯系统的优化方案 2009年7月
标 题 刊物/专著 出版时间 出版社 医用耗材的循证管理 中国医疗器械杂志 2009年3月 非消毒包装植入性医疗器械追溯系统的优化方案 2009年7月 医用耗材定价中循证评价及经济学评价的作用 2010年5月 医用耗材数据资源利用 中国医疗设备 2011年5月 第五章 医院物资管理 医院管理学 第2版 后勤管理分册 2011年8月 人民卫生出版社 杨 海

38
卫生技术评估 循证管理 社会评估 道德评估 医学评估 经济学评估 合法性管理 安全性管理
杨 海

39
循证管理经常被误解为“用几篇文章管理医生”
应尽可能选择论证强度高的证据,最理想的证据是建立在大量研究基础上的专家共识或指南

40
循证医学对文献论证强度的划分 第一级:联合RCT(随机双盲对照试验)所作出的具有同质性的系统综述(Systematic Review)或可信区间窄的单个RCT。 第二级:联合队列研究所作出的具有同质性的系统综述(Systematic Review)或单个队列研究或预后研究。 第三级:联合病例-对照研究所作出的具有同质性的系统综述或单个病例-对照研究。 第四级:系列病例观察。 第五级:专家意见或基于生理、病理生理和基础研究的证据。 杨 海

41
例1:经循证评价纳入竞标范围的实例(用证)
在髓内钉招标中非扩髓髓内钉是否应该被单列?

42
生产方理由 非扩髓髓内钉设计新颖,能够避免因扩髓而造成的对骨内膜血液供应的破坏,从而降低骨折不愈合及深部感染的危险性。动物实验的研究结果证明扩髓破坏了70%的骨内膜血流量,而非扩髓只破坏30%。有部分临床文献能证实。 杨 海

43
独立文献调查结果 《非扩髓与扩髓髓内钉固定治疗成人胫骨干骨折的系统评价》《扩髓与非扩髓髓内钉固定治疗股骨干骨折的系统评价》
两篇循证评价分别纳入文献320篇和206篇。 非扩髓髓内钉固定的骨折不愈合率比扩髓髓内钉固定高 术后感染率方面对胫骨干骨折系统评价的结果显示两种髓内钉的差异没有统计学意义,在股骨干骨折的系统评价中发现由于一些文献的数据缺乏或不全而无法做Meta分析。 杨 海

44
结论 非扩髓髓内钉不应单列,而应该与扩髓髓内钉合并竞标。 杨 海

45
结果 有效增加了该类材料招标的竞争。 获得了供应商、临床专家及管理方的认可。 杨 海

46
例2:为某医院业务管理部门所做的控费咨询实例
医院为控制费用,对某材料实行使用前行政审批 临床专家提出意见: 效率降低 必须使用的患者得不到业务主管部门批准,影响治疗或造成患者流失 管理部门诉求: 论证本措施的合理性 希望获得更好的建议 杨 海

47
步骤1:循证医学证据检索 经采用多重检索策略查找获得一重要证据
该共识是29个国家共422位专家在894篇文献基础上筛选出192篇文献(包括建立在RCT基础上的Meta分析),对这些文献进行严格评价后对照循证医学对证据论证强度的分级形成专家推荐等级,并超过80%的专家意见一致 影响因子2.269 杨 海
,对这些文献进行严格评价后对照循证医学对证据论证强度的分级形成专家推荐等级,并超过80%的专家意见一致. 影响因子 杨 海")
48
杨 海

49
步骤2:根据推荐等级检查部分病史 行政审批前某月 行政审批后某月 使用该材料的患者数量 84 64 其中
用量占80%的患者数量(详细检查这些患者的病史记录) 30 29 推荐等级为A 9 推荐等级为B和/或A 20 26 推荐等级为C和/或D 3 病史中缺相关记录的 11 1 使用该材料数量 211 169 用量占80%的数量 170 135 53 42 121 126 17 7 57 2 杨 海
 推荐等级为A. 9. 推荐等级为B和/或A 推荐等级为C和/或D. 3. 病史中缺相关记录的 使用该材料数量 用量占80%的数量 杨 海")
50
行政审批前某月病史中缺相关记录的 杨 海

51
结果 (1)与行政审批前对照,审批后使用本耗材的患者数量及本耗材数量都有明显减少(84/64、211/169)
(2)与行政审批前对照,审批后使用本耗材的患者中推荐等级为B和/或A的患者比例明显上升(66.67%/89.65%) (3)与行政审批前对照,审批后所使用的本耗材中推荐等级为B和/或A的耗材数量比例明显上升(71.18%/93.33%) (4)与行政审批前对照,审批后所使用的本耗材中推荐等级为C和/或D的耗材数量比例明显下降(10%/5.2%) (5)与行政审批前对照,审批后使用本耗材的患者中病史中缺相关记录的患者比例明显下降(37%/3%,审批后份仅一例) (6)与行政审批前对照,审批后病史中缺相关记录的本耗材数量比例明显下降(33.53%/1.48%,审批后份仅一例2张) 杨 海
与行政审批前对照,审批后使用本耗材的患者中推荐等级为B和/或A的患者比例明显上升(66.67%/89.65%) (3)与行政审批前对照,审批后所使用的本耗材中推荐等级为B和/或A的耗材数量比例明显上升(71.18%/93.33%) (4)与行政审批前对照,审批后所使用的本耗材中推荐等级为C和/或D的耗材数量比例明显下降(10%/5.2%) (5)与行政审批前对照,审批后使用本耗材的患者中病史中缺相关记录的患者比例明显下降(37%/3%,审批后份仅一例) (6)与行政审批前对照,审批后病史中缺相关记录的本耗材数量比例明显下降(33.53%/1.48%,审批后份仅一例2张) 杨 海")
52
我们提供的咨询意见 行政审批明显降低了该耗材的使用量。
行政审批后降低用量的部分主要来自推荐等级为C(may)和D(possible)的适应证,在这两类适应证使用该材料目前循证医学证据并不充足。 如果医院使用该材料的主要目的是保证基本医疗而非学科发展,可以继续采取行政审批方式。 为了提高效率,也可以考虑在临床科室向医院承诺只用于推荐等级为A(must)和B(should)的前提下改为病史抽查加惩戒的方式进行监管。 杨 海
和D(possible)的适应证,在这两类适应证使用该材料目前循证医学证据并不充足。 如果医院使用该材料的主要目的是保证基本医疗而非学科发展,可以继续采取行政审批方式。 为了提高效率,也可以考虑在临床科室向医院承诺只用于推荐等级为A(must)和B(should)的前提下改为病史抽查加惩戒的方式进行监管。 杨 海")
53
例3:下腔静脉滤器 根据该共识以及临床近年使用的回顾性研究结果,医院控制了该材料在相对适应证中的使用,允许在绝对适应证中使用。
杨 海

54
例4:CC Cage和CO Cage 肾形的CC Cage(7480元/个)比直形CO Cage (5540元/个)形状更适合从侧后路植入,但没有证据证明CC Cage的安全性、有效性或成本效果明显优于CO Cage。 将CO Cage作为基本器械,规定CC Cage的用量不得超过Cage总用量的40%。 控制前CC Cage占总用量99%,Cage一月的总收费153.7万元。 控制后CC Cage占总用量40%,相同数量Cage的总收费130.8万元,降低23万元,均次材料费下降1643元。 杨 海

55
医用耗材卫生技术评估目前存在的问题1: 国内 国外 卫生技术评估报告 罕见 较少 医疗评估原研文献 证据等级较高的文献较少 较多
卫生经济评估原研文献 杨 海

56
医用耗材存在很强的专业特点,单纯依靠卫生技术评估专业或卫生经济学专业人员不可能在医用耗材领域推进卫生技术评估。
问题2:医用工程人员参与不够 医用耗材存在很强的专业特点,单纯依靠卫生技术评估专业或卫生经济学专业人员不可能在医用耗材领域推进卫生技术评估。

57
由医用耗材管理者推动并参与的医用耗材卫生技术评估示意
购买者 销售者 要求提供HTA证据 卫生技术评估机构 临床疗效及经济评价 文献 1、2…n 卫生技术评估 文献 使用者 生产者 合作研究 医疗器械注册 及监管部门 医保基金 管理部门 价格管理部门 医政管理部门 采购部门 收费定价 支付政策 采购决策 适宜技术选择 安全/疗效 常规要求提供HTA证据 为医用耗材管理者可以作为的地方

58
由购买者推动的医用耗材卫生经济评价原研项目成功案例:
某品牌透明敷料应如何定价?

59
某品牌强调其透明敷料粘胶专利设计,有明显质量优势,无法与同类产品直接进行价格竞争。
在护理部的支持下进行对照试验,试验组42例、对照组42例主要观察各时段因敷料剥离造成更换的数量。 结果: 杨 海 59

60
合理价格≤基准品价格×3.52 根据相关护理规范,若对100例病例使用透明敷料固定, 对照组需使用100÷(1-73.17%)=373张。
24小时 48小时 72小时 试验组累计更换率 0.00% 5.26% 对照组累计更换率 4.88% 26.83% 73.17% 根据相关护理规范,若对100例病例使用透明敷料固定, 对照组需使用100÷( %)=373张。 试验组需使用100÷(1-5.26%)=106张。 成本之比:373/106=3.52 合理价格≤基准品价格×3.52 在本试验的基础上该品牌正在上海多家医院开展多中心临床研究,已接近尾声:
=373张。 试验组需使用100÷(1-5.26%)=106张。 成本之比:373/106=3.52. 合理价格≤基准品价格×3.52. 在本试验的基础上该品牌正在上海多家医院开展多中心临床研究,已接近尾声:")
61
PI(项目带头人):曹建文 在没有收费名目的前提下,如何选择透明敷料? 申康医院管理研究所所长 上海第六人民医院院长助理
杨 海 61

62
多中心随机对照试验 中心 效应指标: 目的: 从其性能、总成本,为选择透明敷料提供循证依据,进而为收费奠定基础
中心1-儿科医院:试验组110例、对照组103例 中心2-第一人民医院:试验组96例,对照组110例 中心3-肿瘤医院:试验组123例,对照组136例 中心4-新华医院:入组试验组100例,对照组100例 效应指标: 敷料的性能 (便于观察穿刺点、固定导管牢固、方便操作、透气、皮肤反应、撕除时疼痛感) 维护导管的总成本 (耗材成本+维护成本+不良反应处理成本) 目的: 从其性能、总成本,为选择透明敷料提供循证依据,进而为收费奠定基础 杨 海 62
 维护导管的总成本 (耗材成本+维护成本+不良反应处理成本) 目的: 从其性能、总成本,为选择透明敷料提供循证依据,进而为收费奠定基础. 杨 海 62.")
63
“医疗器械循证管理智库沙龙” ——发起单位:卫生部医院管理研究所临床医学工程技术研究基地(上海)
卫生部医院管理研究所上海临床医学工程技术研究基地发起了“医疗器械循证管理智库沙龙” (Medical device Evidence-based Management Summit, MEMS),旨在培养一批能够将循证管理、卫生技术评估等方法学工具用于医用耗材采购及管理的医学工程人员,并通过在采购中索要证据迫使供应商重视循证医学、经济学证据的研究和积累,以促进此类方法学在医用耗材领域广泛开展,进而促进医用耗材费用趋向合理、管理日趋理性。 杨 海 63
,旨在培养一批能够将循证管理、卫生技术评估等方法学工具用于医用耗材采购及管理的医学工程人员,并通过在采购中索要证据迫使供应商重视循证医学、经济学证据的研究和积累,以促进此类方法学在医用耗材领域广泛开展,进而促进医用耗材费用趋向合理、管理日趋理性。 杨 海 63.")
64
设想 第一阶段——启蒙阶段 第二阶段——机制及队伍形成阶段 第三阶段——机制及队伍成熟阶段
杨 海

65
第一阶段——启蒙阶段 时间:从目前到2013年年底前 目标 方法 标志性成果
培养一批能读懂和评价卫生技术评估报告、循证医学证据及经济学评估证据的医用耗材管理者 基于卫生技术评估的医用耗材管理机制形成小范围共识并在少数医疗机构试点 方法 集中的沙龙活动与分散工作相结合 国外医用耗材卫生技术评估实践情况交流 国内卫生技术评估专业人员授课和指导 国内最佳实践单位(包括医疗机构和企业)交流 翻译和学习国外卫生技术评估报告 以基地及实验室为平台,接收企业捐赠并争取政府投入,设立研究基金 标志性成果 形成若干医疗机构基于卫生技术评估的医用耗材管理实践案例 启动若干医用耗材卫生技术评估原研项目 杨 海
交流. 翻译和学习国外卫生技术评估报告. 以基地及实验室为平台,接收企业捐赠并争取政府投入,设立研究基金. 标志性成果. 形成若干医疗机构基于卫生技术评估的医用耗材管理实践案例. 启动若干医用耗材卫生技术评估原研项目. 杨 海")
66
第二阶段——队伍及机制形成阶段 时间:2014年-2015年年底前 目标 方法 标志性成果
在医疗机构医用耗材管理者中形成一支比较稳定的卫生技术评估人才队伍 在部分有代表性的医疗机构形成基于卫生技术评估的医用耗材管理机制 方法 举办“基于卫生技术评估的医用耗材管理”课程教育,对一批医疗机构医用耗材管理者进行系统训练 在卫生技术评估专家指导下进行最佳实践单位经验交流,并以此为基础形成专家团队 举办全国性论坛及征文 标志性成果 完成若干医用耗材卫生技术评估原研项目 向杂志推荐一批论文,有条件的情况下在杂志开辟专栏 形成医疗机构基于卫生技术评估的医用耗材管理机制专家共识或行动指南 形成《基于卫生技术评估的医用耗材定价、选择与使用管理建议》,供政府部门参考 杨 海

67
第三阶段——队伍及机制成熟阶段 时间:2016-2020年(十三五期间) 目标: 方法 标志性成果
医疗机构医用耗材管理者中卫生技术评估人才队伍稳定并扩大 更多的医疗机构形成基于卫生技术评估的医用耗材管理机制 在政府定价、医保支付等方面逐步形成基于卫生技术评估的决策机制 方法 继续举办课程教育、论坛等 与卫生技术评估机构较紧密地合作,共同完成评估项目 在专家指导下完善机制 标志性成果 基于中国数据的各类医用耗材原研文献证据较2012年明显增加 形成若干高新贵重医用耗材的评估报告,供政府定价、医保支付等决策用 对采用该机制的医疗机构或区域通过纵向或横向对比研究能证实该机制在控制医用耗材费用方面的效果 杨 海

68
本图片摄自强生Cordis产品宣传海报

69
我们在每次活动前会具体告知活动主题、时间和地点,您可以选择性地参加。
谢谢聆听,欢迎指正! 有兴趣参加沙龙者可以与我联系: 我们在每次活动前会具体告知活动主题、时间和地点,您可以选择性地参加。

Similar presentations


 日期: 102 年 10 月 09 日 1.>")
家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")









 人生召命的更新 使徒行傳廿六章19-23節.>")





