Download presentation
Presentation is loading. Please wait.

1
Dynamic Dysrrhythmia 快速心律判讀準則與方法 三總急診部

2
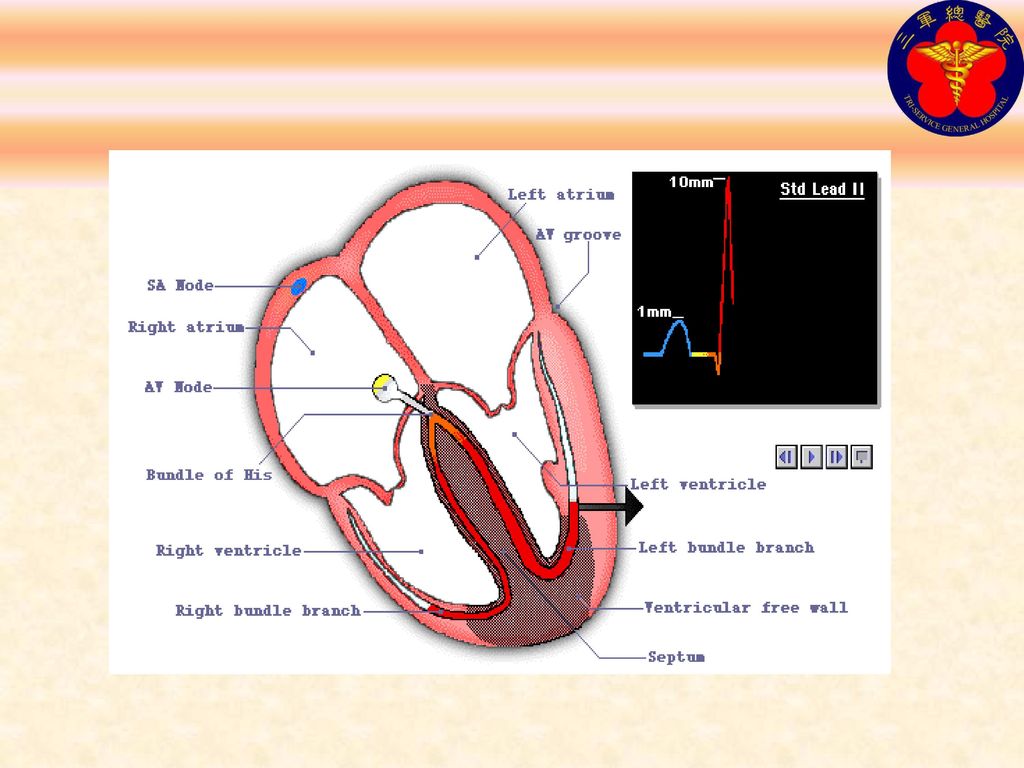
竇房結 房室結 希氏束 結間路徑 左束枝 右束枝 浦金纖維

4
心電圖的基本原理

5
U 波: 心室內 Purkinje fiber 的再極化
QRS:心室去極化 P波:心房去極化 T波:心室再極化

6
正常的心電圖

7
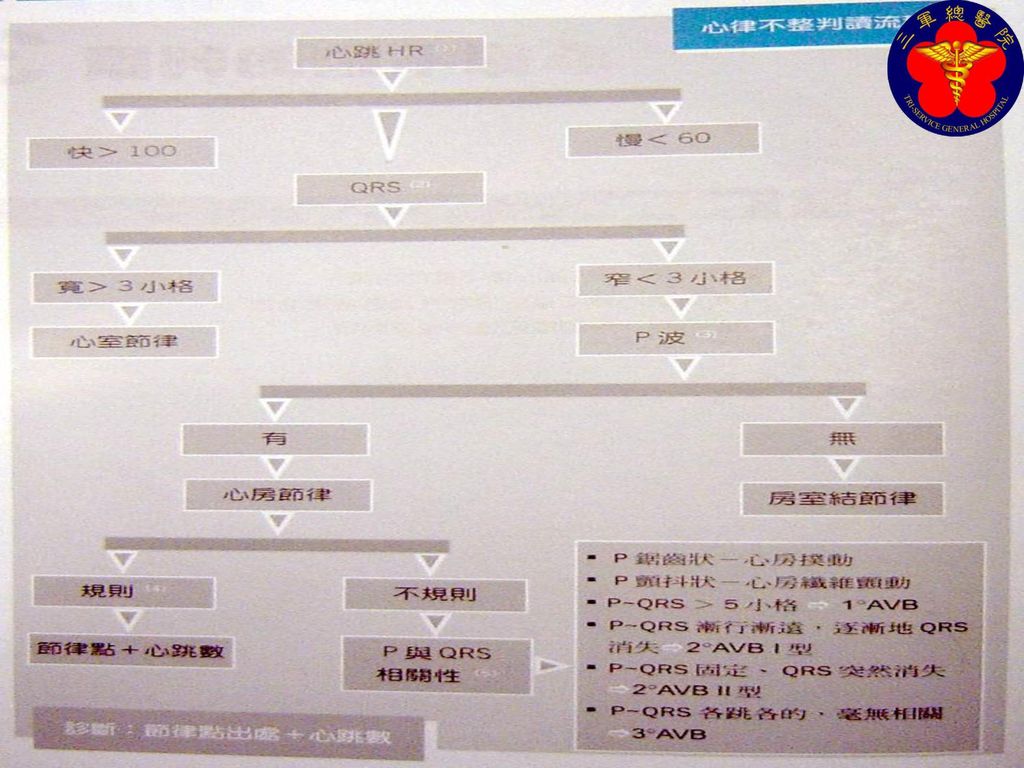
快速心律判讀準則與方法 1. 心跳數(快、慢) 2. QRS(寬、窄) (wide or narrow QRS) 3. P波(P wave)
4. 規則性(Regularity) 5. P & QRS 相關性
 5. P & QRS 相關性.")
8
快速心律判讀準則與方法 心律命名 出處+心跳數 (快or慢) (origin+HR)
 (origin+HR)")
9
快速心律判讀準則與方法 1-(1):沒有脈搏(致命的心律) (Vf, pulseless VT, PEA, asystole)
1-(2):有脈搏 (Normal, Tachycardia, Bradycardia)
:有脈搏. (Normal, Tachycardia, Bradycardia)")
10
沒有脈搏(致命的心律)
")
11
有脈搏 每分鐘心跳數 > 100 則為心搏過速 每分鐘心跳數 < 60 則為心搏過緩

12
快速心律判讀準則與方法 2-(1):寬QRS波 (VT, Idioventricular rhythm) 2-(2):窄QRS波
(Sinus, Atrial, Junctional rhythm, PSVT)
")
13
寬QRS波(Ventricle)
")
14
窄QRS波(SA, A, AV)
")
15
快速心律判讀準則與方法 3-(1):正常(明顯) P波 (Sinus rhythm, A-V block) 3-(2):不同型P波
(Atrial Tachy-, Atrial flutter, MAT(Multifocal AT)(>3種P)) 3-(3):沒有或不明顯的P波 (Asystole, Junctional rhythm, Idioventricular rhythm, Af)
(>3種P)) 3-(3):沒有或不明顯的P波. (Asystole, Junctional rhythm, Idioventricular rhythm, Af)")
16
正常(明顯) P波
 P波")
17
不同型P波

18
不同型P波 MAT

19
不同型P波 MAT

20
沒有或不明顯的P波

21
快速心律判讀準則與方法 4-(1):規則心律 (VT, PSVT, Sinus、Junct-rhythm,
Idioventricular rhythm, 1st & 3rd degree A-V block) 4-(2):不規則心律 (Af, MAT, APC, JPC, VPC, 2nd degree A-V block, 分 Mobitz type I & type II)
 4-(2):不規則心律. (Af, MAT, APC, JPC, VPC, 2nd degree A-V block, 分. Mobitz type I & type II)")
22
規則心律

23
規則心律

24
不規則心律

25
快速心律判讀準則與方法 AF (atrial flutter) 心房撲動 (P波呈鋸齒狀)
Af ( atrial fibrillation ) 心房顫動 (60/分<心跳<100/分) (沒明顯P波(亂抖),R-R不規則)
 心房顫動 (60/分<心跳<100/分) (沒明顯P波(亂抖),R-R不規則)")
26
快速心律判讀準則與方法 1. Af with RVR (心跳>100/分) (rapid ventricular response)
心房顫動合併快速心室反應 2. Af with SVR (心跳<60/分) (slow ventricular response) 心房顫動合併慢速心室反應
 (slow ventricular response) 心房顫動合併慢速心室反應.")
27
Af with RVR

28
WPW Syndrome Wolff-Parkinson-White Syndrome
先天性心臟異常,AV之間多一條輔助道路(肯特束),傳導路徑繞過AV node,心室提早被激活 EKG特點: PR interval<0.12秒 QRS:緩慢上升的Delta波 心搏過速
,傳導路徑繞過AV node,心室提早被激活. EKG特點: PR interval<0.12秒. QRS:緩慢上升的Delta波. 心搏過速.")
29
WPW Syndrome

31
WPW Syndrome with Af

33
了解急性心肌梗塞 知道如何尋找— ST 升高 >1 mm 連續三個導程 J point plus 0.04 second
PR baseline ST-segment deviation = 4.5 mm

34
12導程心電圖變化 Baseline 缺血—tall or inverted T wave (infarct), ST segment may be depressed (angina) 損傷—elevated ST segment, T wave may invert 梗塞 (急性)—abnormal Q wave, ST segment may be elevated and T wave may be inverted 梗塞 (時間不知)—abnormal Q wave, ST segment and T wave returned to normal
—abnormal Q wave, ST segment may be elevated and T wave may be inverted. 梗塞 (時間不知)—abnormal Q wave, ST segment and T wave returned to normal.")
35
前壁心肌梗塞

36
Acute Anterior Wall MI

37
下壁心肌梗塞

38
Acute Inferior Wall MI

39
Acute myocardial infarction in the presence of left bundle branch block
Features suggesting acute MI ST changes in the same direction as the QRS (as shown here) ST elevation more than you'd expect from LBBB alone (e.g. > 5 mm in leads V1 - 3) Q waves in two consecutive lateral leads (indicating anteroseptal MI) (ref. Sgarbossa EB et al, N Engl J Med 1996;334:481-7)
 ST elevation more than you d expect from LBBB alone (e.g. > 5 mm in leads V1 - 3) Q waves in two consecutive lateral leads (indicating anteroseptal MI) (ref. Sgarbossa EB et al, N Engl J Med 1996;334:481-7)")
40
Polymorphic VT

41
Ventricular Pacemaker

42
Long Q-T interval Romano-Ward syndrome is an autosomal dominantly inherited form of long QT interval and there is a risk of recurrent ventricular tachycardia, particularly Torsade de Pointes. Ventricular premature beats (VPBs)
")
43
Junctional rhythym This is a recording from a a woman in her 50's with a long standing history of asthma and palpitations, she was on amiodarone at the time of the recording. The patient had just been converted from supraventricular tachycardia. The rhythm is regular, the QRS is narrow, and p waves are not clearly seen, except for a possible one at the beginning of the second QRS in the rhythm strip. This could be a sign of digitalis toxicity but this was not believed to be the case for this patient.

Similar presentations



影像学检查考虑少 脂肪血管平滑肌脂肪瘤可能大,建议短期随访除外不典型肾癌可能;左肾下极.>")

 來控制,經由房 室結 (AV node) 、希氏徑 (His Bundle) ,把電刺 激由心房傳到心室,引起心臟的收縮,以維持 正常的血壓及身體所需之血液供應。 – 正常成人在休息狀態每分心跳速率為 60.>")






 的堆積,引起 血管內膜局部狹窄,影饗 血流,引發心肌缺氧的症 狀.>")

>")




 河南中医学院第一附属医院 杜正光>")
