Download presentation
Presentation is loading. Please wait.

1
中山醫學大學附設醫院 感染科 李原地 (Yuan-Ti Lee) 醫師
登革熱等蟲媒傳染病之臨床診療及實例探討 恙蟲病之診療及實例探討 中山醫學大學附設醫院 感染科 李原地 (Yuan-Ti Lee) 醫師 中華民國醫師公會全國聯合會及衛生署疾病管制局 日期:101年5月26日(星期六) 地點:台大醫院第7講堂(台北市中正區常德街1號)
 醫師. 中華民國醫師公會全國聯合會及衛生署疾病管制局. 日期:101年5月26日(星期六) 地點:台大醫院第7講堂(台北市中正區常德街1號)")
2
課程大綱 恙蟲病 (Scrub typhus)實例 恙蟲病感染流行病學 恙蟲病感染的病理機轉 恙蟲病的診斷 理學檢查及實驗室檢查
恙蟲病及不明原因發燒(Fever cause unknown)的鑑別診斷 恙蟲病感染抗生素治療
的鑑別診斷. 恙蟲病感染抗生素治療.")
3
病史 51歲婦人有5年高血壓及糖尿病,有規則服藥控制,並無特殊病史。
住南投縣中寮鄉並無固定工作,有時在農田或茶園做幫工,這次感冒症狀,有頭痛、發燒和寒顫及肌肉酸痛等,在診所及地區醫院治療,打針吃藥一直沒退燒,因為發燒5日病情未改善,她先生帶她到大醫院做詳細檢查及治療。 門診,血壓145/70mmHg,體溫過高達39.8。C,心跳每分鐘89次。 進一步詢問病史,家裡無養寵物,及近一個月內無出國旅遊史。 最近因發燒,胃口不佳、出現腹痛及腹脹情形,婦人精神狀況顯得倦怠和虛弱、發燒和合併寒顫,有嚴重頭痛及肌肉酸痛情形並有些咳嗽流鼻水及喉嚨痛。大小便習慣正常,無頻尿或便秘或腹瀉。

4
病史 理學檢查出現急性病態、意識清楚,血壓150/70mmHg偏高,體溫過高達40.8。C,呼吸稍快每分鐘19次,心跳每分鐘88次正常。
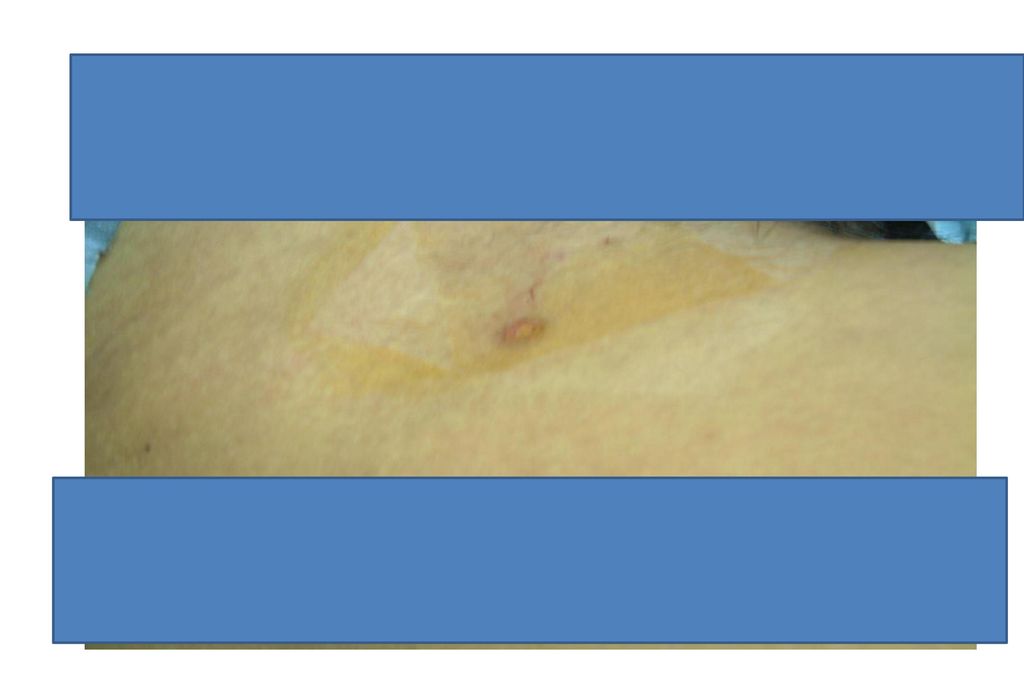
皮膚乾燥,臉色蒼白略黃,下眼瞼蒼白鞏膜發黃,甲狀腺無腫大或結節、頭部腋下或鼠膝無淋巴節腫大,頸部無僵硬、無腦膜炎徵象,心跳規則再左側心尖處可聽到第二級舒張性心雜音、呼吸規律呼吸因清楚、腹部平坦、柔軟,腸音蠕動正常、觸診無肝脾腫大及無摸到腫痛、肋椎間無敲痛,四肢活動正常、皮膚無皮疹及瘀斑。 在頸部有一個0.5x0.5公分大小之傷口。〔附圖〕

5
實驗室檢查結果 檢查項目 檢查結果 W.B.C(/cumm) 5610 W.B.C D/C %
Band Segment Lymphocyte Monocyte Atypical Lymphocyte R.B.C(X 106/cumm) 326 Hemoglobin(gm/dl) 8.1 Ht. (%) 25.1 MCV(fl) 77.0 Platelet (/cumm) 86000 ESR 1 Hour 83, 2 hour 120
 326. Hemoglobin(gm/dl) 8.1. Ht. (%) MCV(fl) Platelet (/cumm) ESR. 1 Hour 83, 2 hour 120.")
6
實驗室檢查結果 檢查項目 檢查結果 Glucose(mg/dl) 186 BUN(mg/dl) 20 Creatinie(mg/dl)
2.1 Albumin(g/dl) 3.4 NA(meq/l) 130 K(meq/l) 4.9 Total Bilirubin 5.1 Direct Bilirubin 2.5 ALP(IU/L) 520 γGT (IU/L) 166 ALT(GPT) (IU/L) 53 AST(GOP) (IU/L) 203 LDH(IU/L) 2371 C.R.P 8.21
 3.4. NA(meq/l) 130. K(meq/l) 4.9. Total Bilirubin Direct Bilirubin ALP(IU/L) 520. γGT (IU/L) 166. ALT(GPT) (IU/L) 53. AST(GOP) (IU/L) 203. LDH(IU/L) C.R.P")
7
微生物學檢查結果 細菌培養 尿液培養及血液培養皆無分離出任何微生物 微生物及免疫檢查 檢查結果 HBsAg (EIA) positive
Anti-HBs negative HBeAg(EIA) Anti-HBC IgM Anti-HCV CMV Ab IgG CMV Ab IgM Mycoplasma Ab 40x negative Cold Hemagglutin 4x negative Chlamydia pneumoniae IgA Chlamydia pneumoniae IgM Widal test 20x negative Weil-Felix test Ferritin 137.53 TIBC 315 Fe 8 Rheumatoid factor <10 Anti-Ds DNA 4.7(negative)
 Anti-HBC IgM. Anti-HCV. CMV Ab IgG. CMV Ab IgM. Mycoplasma Ab. 40x negative. Cold Hemagglutin. 4x negative. Chlamydia pneumoniae IgA. Chlamydia pneumoniae IgM. Widal test. 20x negative. Weil-Felix test. Ferritin TIBC Fe. 8. Rheumatoid factor. <10. Anti-Ds DNA. 4.7(negative)")
8
影像學檢查結果 胸部X光檢查-正常 腹部X光檢查結果-正常 腹部超音波結果-正常

9
病史 會診感染科專科醫師。 感染科專科醫師實驗檢查發現在WBC D/C中有atypical lymphocyte及不成熟的young ce11,thrombocytopenia, 而肝功能不正常,經仔細詢問病史後,發現病患發病約2週前有在南投縣田野工作,病史應和此次發病有關聯,再重新做理學檢查,於病患的前頸部有一個0.5╳ 0.5公分的傷口,判斷為焦痂。 綜合病患的臨床的表徵及檢查,初步診斷為叢林性斑疹傷寒(恙蟲病),抽血送疾病管制局檢驗恙蟲病抗體。 在原有的抗生素中加入Doxycyclin 100mg每12小時口服,病患在第三天後逐漸退燒,臨床症狀大為進步,在口服7日Doxycyclin後病患完全退燒,後來病患完全痊癒出院。 恙蟲病的血清抗體試驗(IFA)為陽性,最後診斷為恙蟲病併合併多發器官侵犯。
,抽血送疾病管制局檢驗恙蟲病抗體。 在原有的抗生素中加入Doxycyclin 100mg每12小時口服,病患在第三天後逐漸退燒,臨床症狀大為進步,在口服7日Doxycyclin後病患完全退燒,後來病患完全痊癒出院。 恙蟲病的血清抗體試驗(IFA)為陽性,最後診斷為恙蟲病併合併多發器官侵犯。")
10
Rickettsial Diseases 立克次體病
Rickettsiae are obligate intracellular gram-negative coccobacilli and short bacilli(屬於絕對細胞內寄生的革蘭氏陰性立克次體科細菌) Usually transmitted by tick, mite, flea, or louse vectors. Except in the case of louse-borne typhus, humans are incidental hosts. 行政院衛生署疾病管制局 人畜共通傳染病臨床指引 A Clinical Guide to Zoonoses
 Usually transmitted by tick, mite, flea, or louse vectors. Except in the case of louse-borne typhus, humans are incidental hosts. 行政院衛生署疾病管制局 人畜共通傳染病臨床指引 A Clinical Guide to Zoonoses.")
11
Rickettsial Diseases立克次體病
依據16S rRNA序列立克次體亦可明顯分為3群, 斑點熱群(spotted fever group rickettsia;SFG)立克次體,為立克次體中依抗原性分為3群中最複雜的一群,種類也最多。 斑疹傷寒群(typhus group;TG) 恙蟲病(又稱叢林型斑疹傷寒)。 行政院衛生署疾病管制局 人畜共通傳染病臨床指引 A Clinical Guide to Zoonoses
立克次體,為立克次體中依抗原性分為3群中最複雜的一群,種類也最多。 斑疹傷寒群(typhus group;TG) 恙蟲病(又稱叢林型斑疹傷寒)。 行政院衛生署疾病管制局 人畜共通傳染病臨床指引 A Clinical Guide to Zoonoses.")
12
恙蟲病(Scrub Typhus) 恙蟲病(Tsutsugamushi disease,tsutsu是惡疾之意,而mushi是指恙蟲)又名叢林型斑疹傷寒〈Scrub typhus〉 病原:恙蟲立克次體〈Orientiatsutsugamushi〉 病媒:恙蟎,屬於蛛形綱(Arachnida),幼螨(chigger)微小約0.2~0.3 mm,肉眼幾乎看不見 台灣主要的恙蟲病媒以地里恙螨(Leptotrombidiumdeliense)為主 疾病分類–屬第四類法定傳染病 通報期限–於1週內進行通報
,幼螨(chigger)微小約0.2~0.3 mm,肉眼幾乎看不見. 台灣主要的恙蟲病媒以地里恙螨(Leptotrombidiumdeliense)為主. 疾病分類–屬第四類法定傳染病. 通報期限–於1週內進行通報.")
13
恙蟲病流行病學特徵 分佈區域:恙蟲病三角亞洲及大洋洲流行的感染症 易感族群 流行季節 流行區域 在恙蟲流行地區〈特別是草叢〉活動者
4月份病例數開始增加 流行區域 以花蓮縣、台東縣、南投縣及離島地區(金門縣、澎湖縣)病例數較多
病例數較多.")
14
Map shows the geographic areas (black) where scrub typhus is endemic.
Figure 1. Map shows the geographic areas (black) where scrub typhus is endemic. 流行病學﹝Epidemiology﹞ 分布於中亞、東亞及東南亞;從西伯利亞東南部、日本北部至澳洲北部以及新赫布里,更西邊至巴基斯坦,甚至海拔10,000英呎高度之喜馬拉雅山上都有此病的分布。 ©2007 by Radiological Society of North America Jeong Y J et al. Radiographics 2007;27:
 where scrub typhus is endemic. 流行病學﹝Epidemiology﹞ 分布於中亞、東亞及東南亞;從西伯利亞東南部、日本北部至澳洲北部以及新赫布里,更西邊至巴基斯坦,甚至海拔10,000英呎高度之喜馬拉雅山上都有此病的分布。 ©2007 by Radiological Society of North America. Jeong Y J et al. Radiographics 2007;27:")
15
Schematic representation of the phylogenetic relationships among major clades of Orientia tsutsugamushi as represented by the DNA sequences of the 56-kDa surface antigen gene. Scrub Typhus: The Geographic Distribution of Phenotypic and Genotypic Variants of Orientia tsutsugamushi 血清型別除了有日本的Kato、新幾內亞的Karp與緬甸的Gilliam三種標準株外,各地還有Kuroki、Kawasaki等超過三十種不同血清型之分布。 Schematic representation of the phylogenetic relationships among major clades of Orientia tsutsugamushi as represented by the DNA sequences of the 56-kDa surface antigen gene. The size of each triangle roughly represents the proportion of all complete or nearly complete sequences from a clade. The percentage in parentheses next to each clade name represents the frequency among 271 sequences, including partial sequences. Detailed phylogenetic relationships are shown in figures 5and 6. Kelly D J et al. Clin Infect Dis. 2009;48:S203-S230 © 2009 by the Infectious Diseases Society of America

16
KARP-related, Gilliam, TA763, JG, JG-v, and KATO-related in Taiwan.
Phylogenetic tree of O. tsutsugamushi based on the nucleotide sequences of the 56-kDa cell surface antigen gene. KARP-related, Gilliam, TA763, JG, JG-v, and KATO-related in Taiwan. Phylogenetic tree of O. tsutsugamushi based on the nucleotide sequences of the 56-kDa cell surface antigen gene. The subset of the phylogenetic tree is made up of isolates (strains from this study are indicated by open circles) associated with clades with sequence divergence from the reference strains (filled circles), such as Karp, Gilliam-related strains, and Kato, and strains isolated from humans (no mark). Isolates are identified by their GenBank accession numbers. Phylogenetic analyses were conducted using MEGA4. The evolutionary history was inferred using the neighbor-joining method and a bootstrap test on 1,000 replicates. Lin P et al. Appl. Environ. Microbiol. 2011; doi: /AEM
 associated with clades with sequence divergence from the reference strains (filled circles), such as Karp, Gilliam-related strains, and Kato, and strains isolated from humans (no mark). Isolates are identified by their GenBank accession numbers. Phylogenetic analyses were conducted using MEGA4. The evolutionary history was inferred using the neighbor-joining method and a bootstrap test on 1,000 replicates. Lin P et al. Appl. Environ. Microbiol. 2011; doi: /AEM")
17
Scrub Typhus Patients in Taiwan
人常在由立克次體、蟲媒以及適當的囓齒類動物共同存在之流行小島 (typhus island) 遭致感染。人的感染機會和職業以及於感染地區的活動有關,易感受者﹝如軍隊﹞進入地方性流行區域時,約有20 ~ 50%的人會在數週至數月內發病。 台灣的恙蟲病病例近年有增加的趨勢,各縣市均有病例報告,病例主要分布在金門縣、澎湖縣、台東縣、花蓮縣、南投縣。
 遭致感染。人的感染機會和職業以及於感染地區的活動有關,易感受者﹝如軍隊﹞進入地方性流行區域時,約有20 ~ 50%的人會在數週至數月內發病。 台灣的恙蟲病病例近年有增加的趨勢,各縣市均有病例報告,病例主要分布在金門縣、澎湖縣、台東縣、花蓮縣、南投縣。")
18
Map of the geographic areas in Taiwan showing O
Map of the geographic areas in Taiwan showing O. tsutsugamushi strains isolated in scrub typhus patient. 2011 縣市名稱 合計 台北市 14 基隆市 新北市(台北縣) 10 宜蘭縣 2 金門縣 77 連江縣 19 新竹市 1 桃園縣 3 新竹縣 苗栗縣 台中市 12 彰化縣 6 南投縣 13 台南市 嘉義市 雲林縣 嘉義縣 4 高雄市 22 屏東縣 澎湖縣 花蓮縣 33 台東縣 42 293
 10. 宜蘭縣. 2. 金門縣. 77. 連江縣. 19. 新竹市. 1. 桃園縣. 3. 新竹縣. 苗栗縣. 台中市. 12. 彰化縣. 6. 南投縣. 13. 台南市. 嘉義市. 雲林縣. 嘉義縣. 4. 高雄市. 22. 屏東縣. 澎湖縣. 花蓮縣. 33. 台東縣")
19
Figure 2. Schema shows the life cycle of a Leptotrombidium mite.
©2007 by Radiological Society of North America Jeong Y J et al. Radiographics 2007;27:

20
傳染窩 感染立克次體的恙蟎,會經由垂直傳染而代傳立克次體,並於其每個發育期中,如卵、幼蟲、若蟲、成蟲各階段均保有立克次體,成為永久性感染
動物宿主為囓齒類、哺乳類(羊、豬、狗、貓)、鳥類(鳥、雞)等,其中又以囓齒類為主 Jerome Goddard Infect Med 17(4): , 2000.
、鳥類(鳥、雞)等,其中又以囓齒類為主. Jerome Goddard Infect Med 17(4): ,")
21
恙蟲病 ( Scrub typhus)感染過程
傳染方式–被具傳染性的恙螨叮咬,經由其唾液使宿主感染立克次體 潛伏期–1-2週,通常為9-12天 可傳染期–不會直接由人傳染給人 感染性及抵抗力 –受感染後對同一型別的立克次體有長期的保護力,但對不同型別此保護力僅短暫存在 –對於生活在流行地區的人,有可能第二次甚至第三次受感染,不過通常症狀較輕微

22
Clinical manifestations of patients with diagnosis of scrub typhus
Fatal case Non-fatal case Clinical manifestations (%) (N = 18) (N = 279) P Fever 13 (72.2) 254 (91.0) 0.025 Chills 11 (61.1) 240 (86.0) 0.011 Sore throat 5 (27.8) 41 (14.7) 0.171 Headache 8 (44.4) 178 (63.8) 0.131 Myalgia 7 (38.9) 177 (63.4) 0.046 Arthralgia 0 (0.0) 12 (4.3) 1 Cough 104 (37.3) Dyspnea 73 (26.2) < 0.001 Nausea/vomiting 6 (33.3) 100 (35.8) Abdominal pain 88 (31.5) Skin rash 182 (65.2) 0.002 Eschar 2 (11.1) 196 (70.3) Lymphadenopathy 1 (5.6) 25 (9.0) Conjunctivitis 31 (11.1) 0.704 Am. J. Trop. Med. Hyg., 81(3), 2009, pp. 484–488
 (N = 18) (N = 279) P. Fever. 13 (72.2) 254 (91.0) Chills. 11 (61.1) 240 (86.0) Sore throat. 5 (27.8) 41 (14.7) Headache. 8 (44.4) 178 (63.8) Myalgia. 7 (38.9) 177 (63.4) Arthralgia. 0 (0.0) 12 (4.3) 1. Cough. 104 (37.3) Dyspnea. 73 (26.2) < Nausea/vomiting. 6 (33.3) 100 (35.8) Abdominal pain. 88 (31.5) Skin rash. 182 (65.2) Eschar. 2 (11.1) 196 (70.3) Lymphadenopathy. 1 (5.6) 25 (9.0) Conjunctivitis. 31 (11.1) Am. J. Trop. Med. Hyg., 81(3), 2009, pp. 484–488.")
23
Clinical manifestations and complications of patients with diagnosis of scrub typhus
Fatal case Non-fatal case Complications (%) (N = 18) (N = 279) P Central nervous system 14 (77.8) 33 (11.8) < 0.001 Confusion 8 (44.5) 29 (10.4) Seizure 2 (11.1) 2 (0.7) 0.019 Coma 4 (22.2) Respiratory system 12 (66.7) 75 (26.9) 0.001 Pulmonary edema 1 (5.6) 19 (6.8) 1 Interstitial pneumonia 11 (3.9) 0.182 Pleural effusion 3 (16.7) 40 (14.3) 0.732 Ventilator use 6 (33.3) 5 (1.8) Cardiovascular system 3 (16.8) 15 (5.4) 0.086 Pericardial effusion 4 (1.4) 0.27 Atrial fibrillation (new onset) 11 (4.0) 0.535 IHD (new onset) 0 (0.0) 0.061 Gastrointestinal system 0 (0.0%) 21 (7.5%) 0.256 Gastric ulcer 18 (7.5%) 0.612 Pancreatitis 1 (7.5%) Upper gastrointestinal bleeding 2 (7.5%) Acute renal failure 13 (72.2) 54 (19.4) Am. J. Trop. Med. Hyg., 81(3), 2009, pp. 484–488
 (N = 18) (N = 279) P. Central nervous system. 14 (77.8) 33 (11.8) < Confusion. 8 (44.5) 29 (10.4) Seizure. 2 (11.1) 2 (0.7) Coma. 4 (22.2) Respiratory system. 12 (66.7) 75 (26.9) Pulmonary edema. 1 (5.6) 19 (6.8) 1. Interstitial pneumonia. 11 (3.9) Pleural effusion. 3 (16.7) 40 (14.3) Ventilator use. 6 (33.3) 5 (1.8) Cardiovascular system. 3 (16.8) 15 (5.4) Pericardial effusion. 4 (1.4) Atrial fibrillation (new onset) 11 (4.0) IHD (new onset) 0 (0.0) Gastrointestinal system. 0 (0.0%) 21 (7.5%) Gastric ulcer. 18 (7.5%) Pancreatitis. 1 (7.5%) Upper gastrointestinal. bleeding. 2 (7.5%) Acute renal failure. 13 (72.2) 54 (19.4) Am. J. Trop. Med. Hyg., 81(3), 2009, pp. 484–488.")
24
恙蟲病 ( Scrub typhus)臨床表徵
發燒:猝發性,持續性高燒伴隨頭痛、背痛、惡寒、盜汗、淋巴結腫大等症狀 焦痂(eschar):約有50-80﹪患者可在叮咬處發現潰瘍性焦痂,大都為無痛性。 出疹:發燒4-5天起皮膚出現紅色斑狀丘疹,由軀幹上部擴至四肢〈不出現於臉、手掌及腳掌〉,第9-10病日消退
:約有50-80﹪患者可在叮咬處發現潰瘍性焦痂,大都為無痛性。 出疹:發燒4-5天起皮膚出現紅色斑狀丘疹,由軀幹上部擴至四肢〈不出現於臉、手掌及腳掌〉,第9-10病日消退.")
25
恙蟲病: 叮咬部位 25 2017/3/18
26
恙蟲病 ( Scrub typhus)臨床表徵
27
Eschar on the abdomen of the patient.
Izzard L et al. J. Clin. Microbiol. 2010; doi: /JCM

28
Figure 3b. Eschar from the bite of a Leptotrombidium mite.
Figure 3b. Eschar from the bite of a Leptotrombidium mite. (a) Photograph shows an epidermal ulcer covered by a black crust surrounded by an erythematous halo. (b) High-power photomicrograph (original magnification, ×400; hematoxylin-eosin stain) shows dermal vasculitis with perivascular infiltrates that consist mostly of lymphocytes and macrophages. The basic pathology of scrub typhus is a vasculitis secondary to direct endothelial injury, in multiple organs, by Orientia tsutsugamushi Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America
 Photograph shows an epidermal ulcer covered by a black crust surrounded by an erythematous halo. (b) High-power photomicrograph (original magnification, ×400; hematoxylin-eosin stain) shows dermal vasculitis with perivascular infiltrates that consist mostly of lymphocytes and macrophages. The basic pathology of scrub typhus is a vasculitis secondary to direct endothelial injury, in multiple organs, by Orientia tsutsugamushi. Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America.")
30
Scrub Typhus: Radiological and Clinical Findings
No. of Lung zone Patients (%) Bilateral Unilateral Upper Lower Even Negative 21(28) Pulmonary abnormalities 53(71) 44 9 2 39 12 Reticulonodular opacities 30(40) 28 1 14 15 Ground-glass opacity 19(25) 17 11 8 Patchy consolidation 14(19) 6 Confluent consolidation 5(7) 5 3 Septal lines 27(36) 27 Subsegmental collapse 4 10 Coarse nodules 6(8) Hilar enlargement 16* – Pleural effusion 9(12) 7 Cardiomegaly 10(13) * Hilar enlargement was predominantly on the right side in 15 cases. Clinical Radiology (2000) 55, 140–144
 Bilateral. Unilateral. Upper. Lower. Even. Negative. 21(28) Pulmonary abnormalities. 53(71) Reticulonodular opacities. 30(40) Ground-glass opacity. 19(25) Patchy consolidation. 14(19) 6. Confluent consolidation. 5(7) Septal lines. 27(36) 27. Subsegmental collapse Coarse nodules. 6(8) Hilar enlargement. 16* – Pleural effusion. 9(12) 7. Cardiomegaly. 10(13) * Hilar enlargement was predominantly on the right side in 15 cases. Clinical Radiology (2000) 55, 140–144.")
31
Figure 6a. Scrub typhus in a 68-year-old man with previously diagnosed usual interstitial pneumonia.
Figure 6a. Scrub typhus in a 68-year-old man with previously diagnosed usual interstitial pneumonia. (a) Initial chest radiograph shows patchy opacity (arrow) in the upper lobe of the right lung and areas of reticular and ground-glass opacity near the base in both lungs, findings suggestive of usual interstitial pneumonia. (b) Axial thin-section (1.0-mm collimation) CT image obtained with lung window settings shows a focal area of ground-glass opacity in the upper lobe of the right lung. Follow-up thin-section CT images obtained 2 weeks later and 17 months later (not shown) revealed resolution of the parenchymal opacity in the right upper lobe. Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America
 Initial chest radiograph shows patchy opacity (arrow) in the upper lobe of the right lung and areas of reticular and ground-glass opacity near the base in both lungs, findings suggestive of usual interstitial pneumonia. (b) Axial thin-section (1.0-mm collimation) CT image obtained with lung window settings shows a focal area of ground-glass opacity in the upper lobe of the right lung. Follow-up thin-section CT images obtained 2 weeks later and 17 months later (not shown) revealed resolution of the parenchymal opacity in the right upper lobe. Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America.")
32
Figure 10a. Acute respiratory distress syndrome in a 47-year-old woman with scrub typhus.
Figure 10a. Acute respiratory distress syndrome in a 47-year-old woman with scrub typhus. (a) Initial anteroposterior chest radiograph shows diffuse ground-glass opacity in the right lung and the lower zone of the left lung and a small amount of pleural effusion in both lungs. (b) Follow-up anteroposterior chest radiograph obtained 6 days later shows extensive airspace consolidation in both lungs, a feature suggestive of acute respiratory distress syndrome. Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America
 Initial anteroposterior chest radiograph shows diffuse ground-glass opacity in the right lung and the lower zone of the left lung and a small amount of pleural effusion in both lungs. (b) Follow-up anteroposterior chest radiograph obtained 6 days later shows extensive airspace consolidation in both lungs, a feature suggestive of acute respiratory distress syndrome. Jeong Y J et al. Radiographics 2007;27: ©2007 by Radiological Society of North America.")
33
Pediatric Scrub Typhus in Eastern Taiwan
Scrub typhus should be considered in children with fever and hepatic dysfunction, particularly in those with a history of environmental exposure in an endemic area for scrub typhus. Eschar offers an important diagnostic clue, but not for all cases. Children with scrub typhus may develop serious complications and may even die if appropriate treatment is not given. Doxycycline is an effective antibiotic for pediatric scrub typhus in Taiwan. Pediatr Neonatol 2009;50(3):96−101
:96−101.")
34
Complications of Scrub Typhus
No. of patients (%) Pneumonia 12(36) ARDS 5(15) ARF 3(9) Myocarditis 1(3) Septic shock Data from Clinical Radiology (2000) 55, 140–144 Journal of the American Academy of Nurse Practitioners 24 (2012) 160–165
 Pneumonia. 12(36) ARDS. 5(15) ARF. 3(9) Myocarditis. 1(3) Septic shock. Data from Clinical Radiology (2000) 55, 140–144. Journal of the American Academy of Nurse Practitioners 24 (2012) 160–165.")
35
An 81-year-old woman with scrub typhus
An 81-year-old woman with scrub typhus. Initially, bilateral extensive consolidation is visible mainly in the lower zones. Cardiomegaly, pulmonary oedema and pleural effusions are also present. Clinical Radiology (2000) 55, 140–144
 55, 140–144.")
36
Follow-up chest radiograph taken 10 days later, after treatment with doxycycline, shows clearing of both lower lungs and pleural effusions and a decrease in cardiac size. Clinical Radiology (2000) 55, 140–144
 55, 140–144.")
39
Scrub Typhus-Associated Central Nervous System Complications
Meningoencephalitis1,5 Acute Disseminated Encephalomyelitis2 Scrub typhus complicated by intracranial hemorrhage - A Case report.3 Acute transverse myelitis4 Ann Indian Acad Neurol 2012;15:141-4. Acta Neurol Taiwan 2006;15: Tzu Chi Med J 2005;17:111-4. Diagn Microbiol Infect Dis. 2008;60(2):237-9. Arch Neurol 2000;57:1770-2
: Arch Neurol 2000;57:")
40
Differentiate Diagnosis
Coinfection with Leptospirosis and Scrub Typhus in Taiwanese Patients1 The clinical differences between dengue and scrub typhus with acute respiratory failure in southern Taiwan2 Acute Q fever and scrub typhus, southern Taiwan3 Clinical Manifestations and Complications of Rickettsiosis in Southern Taiwan4 Acute Q fever Scrub typhus Murine typhus Am J Trop Med Hyg. 2007; 77(3): 525–527. Infection 2012, DOI: /s Emerg Infect Dis. 2009; 15(10): 1659–1661. J Formos Med Assoc. 2002;101:385–92.
: 525–527. Infection 2012, DOI: /s Emerg Infect Dis. 2009; 15(10): 1659–1661. J Formos Med Assoc. 2002;101:385–92.")
41
Comparative initial symptoms/signs between adult dengue and scrub typhus patients with acute respiratory failure Initial symptoms/signs Dengue (n = 18) Scrub typhus (n = 8) P-value Fever 17 (94.4%) 8 (100%) 1.000 Eschar 6 (62.5%) 0.001 Petechiae 8 (44.4%) 3 (37.5%) Arthralgia 1 (12.5%) 0.190 Myalgia Headache 2 (25%) 0.420 Gum bleeding 3 (16.7%) Chest pain 5 (27.8%) Cough 10 (55.6%) 0.031 Dyspnea 7 (41.2%) Hemoptysis 2 (11.1%) Abdomen pain 11 (61.1%) 0.401 Vomiting 7 (38.9%) 0.360 Tarry stool 6 (33.3%) INFECTION 2012, DOI: /s INFECTION 2012, DOI: /s
 Scrub typhus (n = 8) P-value. Fever. 17 (94.4%) 8 (100%) Eschar. 6 (62.5%) Petechiae. 8 (44.4%) 3 (37.5%) Arthralgia. 1 (12.5%) Myalgia. Headache. 2 (25%) Gum bleeding. 3 (16.7%) Chest pain. 5 (27.8%) Cough. 10 (55.6%) Dyspnea. 7 (41.2%) Hemoptysis. 2 (11.1%) Abdomen pain. 11 (61.1%) Vomiting. 7 (38.9%) Tarry stool. 6 (33.3%) INFECTION 2012, DOI: /s INFECTION 2012, DOI: /s")
42
Dengue (n = sample size) Scrub typhus (n = sample size)
Comparative initial laboratory data between adult dengue and scrub typhus patients with ARF Dengue (n = sample size) Scrub typhus (n = sample size) P-value WBC (×103/μL) 7.40 ± 5.74(n = 18) 11.84 ± 4.95 (n = 8) 0.026 Hematocrit (%) 33.19 ± 8.64 (n = 18) 33.13 ± 5.54 (n = 8) 0.935 Platelet (×109/L) 42.2 ± 33.9 (n = 18) 104.1 ± 93.3 (n = 8) 0.008 PT (s) 12.82 ± 1.36 (n = 18) 10.74 ± 0.98 (n = 5) 0.007 APTT (s) 50.81 ± (n = 18) 37.44 ± 4.06 (n = 5) 0.002 AST (U/L) 709.2 ± 1,381.4 (n = 18) 153.9 ± 68.5 (n = 8) 0.129 ALT (U/L) 543.8 ± 1,029.6 (n = 18) 153.5 ± 78.1 (n = 8) 0.461 ALP 115.0 ± 29.4 (n = 9) 178.8 ± (n = 8) 0.114 Total bilirubin (mg/dL) 2.68 ± 1.29 (n = 12) 3.72 ± 3.67 (n = 8) 0.473 BUN (mg/dL) 64.6 ± 43.2 (n = 14) 20.9 ± 9.1 (n = 8) <0.001 Creatinine (mg/dL) 3.77 ± 3.37 (n = 17) 1.05 ± 0.37 (n = 8) Albumin (g/dL) 2.47 ± 0.53 (n = 18) 2.80 ± 0.92 (n = 8) 0.531 INFECTION 2012, DOI: /s
 Scrub typhus (n = sample size) P-value. WBC (×103/μL) 7.40 ± 5.74(n = 18) ± 4.95 (n = 8) Hematocrit (%) ± 8.64 (n = 18) ± 5.54 (n = 8) Platelet (×109/L) 42.2 ± 33.9 (n = 18) ± 93.3 (n = 8) PT (s) ± 1.36 (n = 18) ± 0.98 (n = 5) APTT (s) ± (n = 18) ± 4.06 (n = 5) AST (U/L) ± 1,381.4 (n = 18) ± 68.5 (n = 8) ALT (U/L) ± 1,029.6 (n = 18) ± 78.1 (n = 8) ALP ± 29.4 (n = 9) ± (n = 8) Total bilirubin (mg/dL) 2.68 ± 1.29 (n = 12) 3.72 ± 3.67 (n = 8) BUN (mg/dL) 64.6 ± 43.2 (n = 14) 20.9 ± 9.1 (n = 8) < Creatinine (mg/dL) 3.77 ± 3.37 (n = 17) 1.05 ± 0.37 (n = 8) Albumin (g/dL) 2.47 ± 0.53 (n = 18) 2.80 ± 0.92 (n = 8) INFECTION 2012, DOI: /s")
43
Symptoms and Signs in 51 Patients with Rickettsial Infections
Acute Q fever (n = 28) Scrub typhus (n = 16) Murine typhus (n = 7) Symptoms Fever 28 16 6 Chills 22 13 Cough 12 7 5 Sore throat 3 1 Headache 14 10 Diarrhea Abdominal discomfort/pain 8 2 Nausea/vomiting Arthralgia/myalgia 4 Signs Maculopapular rash Eschar Regional lymphadenopathy Relative bradycardia 20 (n = 21) 11 (n = 15) 2 (n = 6) Hepatomegaly* Splenomegaly* *Signs detected on physical examination. J Formos Med Assoc. 2002;101:385–92.
 Scrub typhus (n = 16) Murine typhus (n = 7) Symptoms. Fever Chills Cough Sore throat Headache Diarrhea. Abdominal discomfort/pain Nausea/vomiting. Arthralgia/myalgia. 4. Signs. Maculopapular rash. Eschar. Regional lymphadenopathy. Relative bradycardia. 20 (n = 21) 11 (n = 15) 2 (n = 6) Hepatomegaly* Splenomegaly* *Signs detected on physical examination. J Formos Med Assoc. 2002;101:385–92.")
44
Laboratory and Image Findings In 51 Patients with Rickettsial Infections
Acute Q fever (n = 28) Scrub typhus (n = 16) Murine typhus (n = 7) Elevated aminotransferases 28 16 7 Hyperbilirubinemia 5 (n = 25) 6 2 Elevated C-reactive protein 27 Microscopic hematuria 4 Leukocytosis 3 Thrombocytopenia Abnormal chest roentgenogram 3 (n = 25) 10 2 (n = 5) Hepatomegaly* 8 (n = 27) 1 (n = 13) 1 Splenomegaly* 8 (n = 13) *Detected by ultrasonography or computerized tomography. J Formos Med Assoc. 2002;101:385–92.
 Scrub typhus (n = 16) Murine typhus (n = 7) Elevated aminotransferases Hyperbilirubinemia. 5 (n = 25) Elevated C-reactive protein. 27. Microscopic hematuria. 4. Leukocytosis. 3. Thrombocytopenia. Abnormal chest roentgenogram. 3 (n = 25) (n = 5) Hepatomegaly* 8 (n = 27) 1 (n = 13) 1. Splenomegaly* 8 (n = 13) *Detected by ultrasonography or computerized tomography. J Formos Med Assoc. 2002;101:385–92.")
45
Diagnosis of Scrub Typhus
檢驗條件 符合下列檢驗結果之任一項者,定義為檢驗結果陽性: (一)臨床檢體(血液或皮膚傷口(焦痂))分離並鑑定出恙蟲病立克次體(Orientia tsutsugamushi)。 (二)臨床檢體分子生物學核酸檢測陽性以間接免疫螢光染色法(Indirect Immunofluorescene Assay,IFA)檢測急性期(或初次採檢)血清,IgM 抗體≧1:80 且 IgG 抗體≧1:320。 (三)以間接免疫螢光染色法,檢測成對(恢復期及急性期)血清,恙蟲病立克次體特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升。
臨床檢體(血液或皮膚傷口(焦痂))分離並鑑定出恙蟲病立克次體(Orientia tsutsugamushi)。 (二)臨床檢體分子生物學核酸檢測陽性以間接免疫螢光染色法(Indirect Immunofluorescene Assay,IFA)檢測急性期(或初次採檢)血清,IgM 抗體≧1:80 且 IgG 抗體≧1:320。 (三)以間接免疫螢光染色法,檢測成對(恢復期及急性期)血清,恙蟲病立克次體特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升。")
46
Summary of antigenic strains described by the selected studies, listed by the country where the indirect immunofluorescence assay was used. Summary of antigenic strains described by the selected studies, listed by the country where the indirect immunofluorescence assay was used. Blacksell S D et al. Clin Infect Dis. 2007;44: © 2007 Infectious Diseases Society of America

47
檢體採檢送驗事項

48
Summary of key treatment studies in scrub typhus
Drugs Author/ Year Type of study Key finding Chloramphenicol VS tetracycline Sheehyet al. 1973 CT Tetracycline superior to chloramphenicol Doxycycline 200 mg SD VS tetracycline 100 mg QID 7 days Brownet al. 1978 RCT doxycycline as effective as tetracycline Doxycycline 100 mg BID 3 days VS tetracycline 100 mg QID 7 days Songet al. 1995 doxycycline as effective as tetracycline Azithromycin 500 mg SD VS doxycycline 200 mg Daily 7 days Kim et al. 2004 Azithromycin equally effective as doxycycline . Defervescence slightly longer with doxycycline. Less gastrointestinal adverse effects with azithromycin Azithromycin 500 mg 3 days VS doxycycline 200 mg 7 days Phimdaet al. 2007 Azithromycin 3-day equally effective as doxycycline. Defervescence longer with azithromycin. Telithromycin 800 mg daily 5 days VS doxycycline 200 mg 5 days Quasi-RCT Teilithromycin as effective as doxycycline Rifampicin 600 mg/900 mg VS doxycycline 200 mg 7 days Wattet al. 2000 Rifampicin superior to doxycycline–faster defervescence, fewer relapses (trial was in a geographical locality where doxycycline resistance was known to occur) Levofloxacin VS tetracyclines Tsaiet al. 2010 Retrospective analysis Levofloxacin as effective as tetracyclines. Longer time to defervescence with levofloxacin. Higher mortality with levofloxacin in severe disease Trop Doct January 2011 vol. 41 no. 1 1-4 RCT:Randomized controlled trial Trop Doct January 2011 vol. 41 no. 1 1-4
 Levofloxacin VS tetracyclines. Tsaiet al Retrospective analysis. Levofloxacin as effective as tetracyclines. Longer time to defervescence with levofloxacin. Higher mortality with levofloxacin in severe disease. Trop Doct January 2011 vol. 41 no RCT:Randomized controlled trial. Trop Doct January 2011 vol. 41 no")
49
Intravenous Minocycline Versus Oral Doxycycline for the Treatment of Noncomplicated Scrub Typhus
Conclusion: Both antibiotics have similar efficacy for the treatment of noncomplicated scrub typhus. Nearly all cases responding to both antibiotics became afebrile within 3 days. Journal of Microbiology, Immunology and Infection. 2011; 44:33-38

50
Levofloxacin Versus Tetracycline Antibiotics for the Treatment of Scrub Typhus
Conclusions: Levofloxacin is effective in patients with scrub typhus, but has a longer time to defervescence compared with tetracycline antibiotics. When levofloxacin is used for severe scrub typhus, higher mortality may be attributed to the longer time to defervescence. Kaplan—Meier curve of the time to defervescence in patients initially treated with levofloxacin and tetracycline antibiotics ( p = ). International Journal of Infectious Diseases;2010:14, e62—e67.
. International Journal of Infectious Diseases;2010:14, e62—e67.")
51
Treatment of O. tsutsugamushi Infection
Tetracycline, doxycycline, or chloramphenicol is used to treat scrub typhus. Minocin 200mg/ IV/ st., 100mg/ IV/ q12h Doxycycline 100mg/ P.O./ q12h, for 14 days Chloramphenicol-resistant & doxycycline-resistant strains of O tsutsugamushi occur in the areas of northern Thailand.# Oral azithromycin was administered in a 500-mg dose on the first day, followed by 250 mg daily on days 2 to 5.* in children and pregnant women. #Lancet 1996 Jul 13;348(9020):86-9 *Antimicrob. Agents Chemother. 1999, 43:
:86-9. *Antimicrob. Agents Chemother. 1999, 43:")
52
治療及預後 治療方式 –抗生素療法: 預後 –未經治療,死亡率可達百分之六十 –經治療後死亡率小於百分之五
四環黴素(tetracycline)類 如doxycycline、minocycline等 氯黴素(chloramphenicol) 預後 –未經治療,死亡率可達百分之六十 –經治療後死亡率小於百分之五
類 如doxycycline、minocycline等. 氯黴素(chloramphenicol) 預後. –未經治療,死亡率可達百分之六十. –經治療後死亡率小於百分之五.")
53
References, Web sites and Further readings
Center for Disease Control Taiwan, ROC,台灣疾病管制局 Centers for Disease Control and Prevention, U.S.A, World Health Organization, Mandell, Gerald L. et al. Principles and Practice of Infectious Disease. Sixth Edition Churchill Livingstone. October 22, pp Timmreck, Thomas C. An Introduction to Epidemiology. 2nd ed Jones & Bartlett Publishers, Inc. Boston, United States of America. CDC, Principles of Epidemiology. 3nd ed Atlanta, GA: Centers for Disease Control and Prevention. Wolfgang, A & Iris, P. Handbook of Epidemiology. 1st ed Springer-Verlag Berlin Heidelberg , Germany. Fred, B.; Pauline, van den D. ; Jianhong, W. Mathematical Epidemiology Springer-Verlag Berlin Heidelberg , Germany. Richard D.T. Farmer, Ross Lawrenson. Lecture notes on epidemiology and public health medicine. 5th ed Blackwell Publishing, Inc., Massachusetts, USA. Stefan Ma. Mathematical Understanding of Infectious Disease Dynamics World Scientific Publishing. Bonita R., R. Beaglehole, T. Kjellstrom. Basic epidemiology. 2nd ed. World Health Organization, 2006.

Similar presentations

 定義 免疫性水皰病 表皮內水皰 Immunoglobulins and complements are found bound to the intercellular substance in the perilesional epidermis.>")




 – 全球疫情 (Global) – 台灣 (Taiwan) 致病機轉及傳染 (Pathogenesis and transmission) 診斷 (Diagnosis)>")
 的制定及临床应用体会 北京朝阳医院 呼吸与危重症医学科 曹志新 2009-10-27.>")



>")

 重庆医科大学 儿科学院 刘恩梅.>")

>")
 河南中医学院第一附属医院 杜正光>")



