Download presentation
Presentation is loading. Please wait.

1
透析液的選擇 與 抗凝劑在各種透析之應用 林口長庚醫院腎臟科 黃正誼

2
Acid concentrate + NaHCO3 concentrate A液+B液
1:1.83:34 Composition and management of HD fluid (PABST) A. Grassmann P 2000, pp 306 Although the concentrate market for single-pass dialysis is still dominated by liquid concentrates, dry concentrates are gaining ground. Dry concentrate for the B component of bicarbonate dialysis fluid is now routinely employed in many clinics, while a dry form of part of the A component has recently been developed. Merits: low weight, and volume, reduce transport costs, storage space and waste volume, bacterial growth is effectively hindered, stable physicohemical state makes long storage times feasible. 混合比例 e.g ,
 A. Grassmann P 2000, pp 306 Although the concentrate market for single-pass dialysis is still dominated by liquid concentrates, dry concentrates are gaining ground. Dry concentrate for the B component of bicarbonate dialysis fluid is now routinely employed in many clinics, while a dry form of part of the A component has recently been developed. Merits: low weight, and volume, reduce transport costs, storage space and waste volume, bacterial growth is effectively hindered, stable physicohemical state makes long storage times feasible. 混合比例. e.g ,")
4
Sodium Profiles 鈉濃度調整模式
Cramping reduction Hypotension reduction A sodium model is just that! A model must include the known kinetics and then apply mathematical algorithms that are consistent with the kinetics and can be validated in clinical practice. This is not what is available with current dialysis technology. What is available are sodium profiles. Sodium profiles are simply predetermined variations in dialysate sodium concentration (or activity) above or below a set point known as baseline sodium concentration. Typical sodium profile plots are shown in the slide. In some dialysis systems (e.g., Fresenius) the profiles are based on an algorithm such that net sodium diffusion is at or near zero. This is achieved by counterbalancing the sum of the times and magnitudes of Na > baseline by fixing the duration and magnitude of the phases when Na < baseline. Use of profiles with this built-in safeguard, while not 100% accurate, ensures the patient is protected from large changes in net diffusive sodium flux and, in the absence of truly comprehensive and physiological algorithms, seems a necessary safety feature. Other systems permit the operator to program the profile using a touch screen - I call this “free hand” profiling and it is represented by the last box in the slide. Access to such free profiling may produce creativity in dialysis but, without some imposed restriction or limit controlling net sodium diffusion, exposes patients to risk. = baseline Na concentration Time average [Na] Vs fixed [Na]
 above or below a set point known as baseline sodium concentration. Typical sodium profile plots are shown in the slide. In some dialysis systems (e.g., Fresenius) the profiles are based on an algorithm such that net sodium diffusion is at or near zero. This is achieved by counterbalancing the sum of the times and magnitudes of Na > baseline by fixing the duration and magnitude of the phases when Na < baseline. Use of profiles with this built-in safeguard, while not 100% accurate, ensures the patient is protected from large changes in net diffusive sodium flux and, in the absence of truly comprehensive and physiological algorithms, seems a necessary safety feature. Other systems permit the operator to program the profile using a touch screen - I call this free hand profiling and it is represented by the last box in the slide. Access to such free profiling may produce creativity in dialysis but, without some imposed restriction or limit controlling net sodium diffusion, exposes patients to risk. = baseline Na concentration. Time average [Na] Vs fixed [Na]")
5
鈉濃度調整模式 使用以穩定血壓的策略不一定奏效,有時候反而會造成口渴及加重體液上升,導致血壓上升、體重增加之惡性循環。
適應症包括:透析中低血壓、肌肉抽搐、重度氮血症的初始透析、血行動力學不穩定的病人(如加護病房病患)。 禁忌症則為高血壓病患。
。 禁忌症則為高血壓病患。")
6
Frequency with or without intradialytic hypotension with the use of four treatments
[Na] 148 131 vs 138 mmo/L Zhou, Y. L. et al. Nephrol. Dial. Transplant :

7
鉀 一般均使用低鉀透析液(1.0-2.0mEq/L) - no individualization.
鉀離子的透析量多寡,取決於血液和透析液的濃度差。 ( < mEq even under [K]=0 mEq/L) 影響鉀離子的分配而改變濃度差:酸鹼度的改變,液體張力(Tonicity),糖分的變化,胰島素濃度和交感神經活性。
 影響鉀離子的分配而改變濃度差:酸鹼度的改變,液體張力(Tonicity),糖分的變化,胰島素濃度和交感神經活性。")
8
鉀 心臟衰竭的病患,特別是同時服用Digoxin者,須慎防產生心律不整。
為了避免透析前期血鉀劇烈的下降,Redaelli 等學者採用鉀濃度調整模式(keep gradient 1.5 mEq/L),以指數線性逐步調降鉀離子濃度於肝硬化之病患 避免肝腦病變,透析液鉀濃度不應低於2.0mEq/L。 Find out origin paper
,以指數線性逐步調降鉀離子濃度於肝硬化之病患. 避免肝腦病變,透析液鉀濃度不應低於2.0mEq/L。 Find out origin paper.")
9
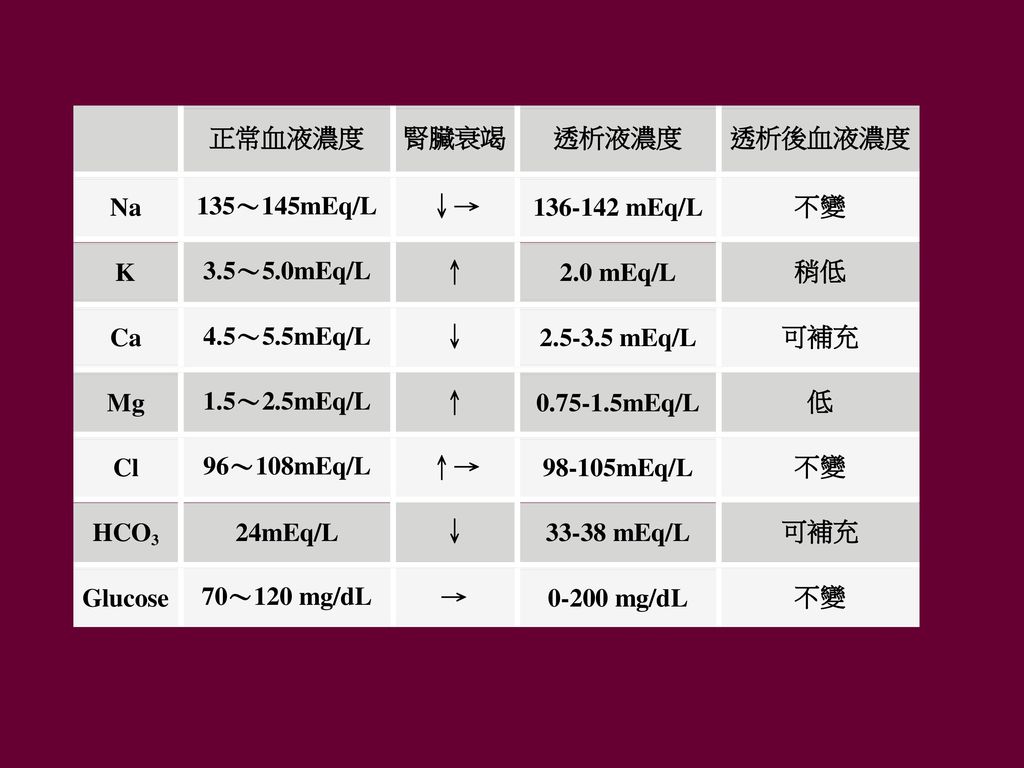
鈣 (2.5mEq/L-3.5mEq/L)
")
10
鈣 (2.5mEq/L-3.5mEq/L) 高鈣的透析液: 血壓上升的機轉主要在於左心室輸出量的增加,至於血管收縮所扮演的角色則極小。
 高鈣的透析液: 血壓上升的機轉主要在於左心室輸出量的增加,至於血管收縮所扮演的角色則極小。")
11
鎂離子 濃度一般為0.75-1.5 mEq/L。 使用口服氫氧化鎂(Mg(OH)2)配合無鎂離子的透析液,對於高磷血症無裨益。
口服碳酸鎂(MgCO3)和半量的碳酸鈣,同時配合鎂離子0.6 mg/dl (0.53 mEq/L)的透析液,其血磷值與口服一般量碳酸鈣配合鎂離子1.8 mg/dl (1.6 mEq/L)的透析液相同。
和半量的碳酸鈣,同時配合鎂離子0.6 mg/dl (0.53 mEq/L)的透析液,其血磷值與口服一般量碳酸鈣配合鎂離子1.8 mg/dl (1.6 mEq/L)的透析液相同。")
12
重碳酸鹽(Bicarbonate) 一般使用濃度為33-38 mEq/L。 使用高濃度之碳酸鹽時會增加PH值及重碳酸鹽濃度。
重碳酸鹽過高會引起急性代謝性鹼中毒之症狀,如疲倦、抽筋、意識改變等 維持透析後不要有鹼中毒,儘量保持透析前total CO2>23 mmol/L。

13
醋酸鹽(Acetate) 早期以重碳酸鹽為血液透析的酸鹼緩衝劑,使用不便。 1960年代後採用醋酸鹽
醋酸鹽經人體肌肉代謝後,可以轉變為重碳酸鹽 易造成血行動力的不穩定 如直接降低血管週邊阻力 interleukin-1釋放進而導致血管擴張 因透析中重碳酸鹽的流失造成代謝性酸血症 醋酸鹽代謝伴隨低血氧症…等

14
Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis:
Patients receiving the citrate dialysate had significantly lower systolic blood pressure (BP) (-4.3 mmHg, p < 0.01) and peripheral resistances (PR) (-51 dyne.sec.cm-5, p < 0.001) while stroke volume was not increased. In hypertensive patients there was a substantial reduction in BP (-7.8 mmHg, p < 0.01). With the C+ dialysate the BP gap was less pronounced but the reduction in PR was even greater (-226 dyne.sec.cm-5, p < 0.001). Analyses of the fluctuations in PR and of subjective tolerance suggested improved haemodynamic stability with the citrate dialysate. Furthermore, an increase in pre-dialysis bicarbonate and a decrease in pre-dialysis BUN, post-dialysis phosphate and ionised calcium were noted. Systemic coagulation activation was not influenced by citrate. Conclusion The positive impact on dialysis efficiency, acid-base status and haemodynamics, as well as the subjective tolerance, together indicate that citrate dialysate can significantly contribute to improving haemodialysis in selected patients. Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis: BMC Nephrology 2009; 10:7
 (-4.3 mmHg, p < 0.01) and peripheral resistances (PR) (-51 dyne.sec.cm-5, p < 0.001) while stroke volume was not increased. In hypertensive patients there was a substantial reduction in BP (-7.8 mmHg, p < 0.01). With the C+ dialysate the BP gap was less pronounced but the reduction in PR was even greater (-226 dyne.sec.cm-5, p < 0.001). Analyses of the fluctuations in PR and of subjective tolerance suggested improved haemodynamic stability with the citrate dialysate. Furthermore, an increase in pre-dialysis bicarbonate and a decrease in pre-dialysis BUN, post-dialysis phosphate and ionised calcium were noted. Systemic coagulation activation was not influenced by citrate. Conclusion. The positive impact on dialysis efficiency, acid-base status and haemodynamics, as well as the subjective tolerance, together indicate that citrate dialysate can significantly contribute to improving haemodialysis in selected patients. Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis: BMC Nephrology 2009; 10:7.")
15
Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis:
BMC Nephrology 2009; 10:7

16
Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis:
BMC Nephrology 2009; 10:7

17
透析液離子濃度變化優缺點 優點 缺點 鈉 增加 血行動力較穩定,較少抽筋 兩次透析間隔體重增加較多,血壓上升 減少 兩次透析間隔體重增加較少
透析中低血壓,較易抽筋 鈣 抑制PTH,促進血行動力穩定 高鈣血症,易引起不活動性骨病變 可容許使用較多含鈣藥品及Vit.D 刺激PTH, 稍微負向影響血行動力

18
優點 缺點 鉀 增加 冠狀動脈疾病或服用毛地黃較不會心律不整, 較不會反彈性高血壓 高鉀血症 減少 飲食攝取鉀離子較自由,可能改善心肌收縮功能 易引起心律不整或加重自律神經失調 重碳酸鹽 改善慢性酸血症,進而改善營養和骨骼代謝 透析後鹼血症 較不會慢性鹼血症 具慢性酸血症傾向 鎂 ? 較不會心律不整 ? 穩定血行動力 慢性高鎂血症 可容許使用含鎂之磷結合劑 慢性低鎂血症

19
添加葡萄糖的透析液 血壓可能變低 糖尿病患者血糖不變,且變異較少
BP / (glucose 100 mg/dl) BP / (glucose free) 糖尿病患者血糖不變,且變異較少 Sangill M. Am J Kidney Dis 2006;47:
 BP / (glucose free) 糖尿病患者血糖不變,且變異較少. Sangill M. Am J Kidney Dis 2006;47:")
20
透析液的選擇 個別性的考量 透析液應該依照病患的特殊性做適當的調整 病患平均和透析中血壓的變化 糖尿病與否 兩次透析間隔體液的增加
血中各類離子之高低…等

21
參考實例 張先生是一位長期接受血液透析治療的患者,其血壓一向穩定,透析中也無低血壓或血壓上升的現象。由於醫院透析機台的改變,使用不同的透析液之後,張先生屢次發生透析中血壓上升的現象。以下是兩種透析液的成分,試分析血壓高可能的原因。

22
參考實例 原使用的透析液 A液:B液:RO水=1:1.83:34 改變後的透析液 品名 濃度(mEq/L) Na+ K+ Ca+2 Mg+2
Cl- CH3COO- HCO3- Dextrose(mg/dl) No.X (A液) 75.0 2.0 2.5 1.0 80.5 5.0 --- 100.0 Bicarbonate(B液) 65.0 26.0 39.0 混和後濃度 140.0 106.5 改變後的透析液 改變後的透析液 品名 濃度(mEq/L) Na+ K+ Ca+2 Mg+2 Cl- CH3COO- HCO3- Dextrose(mg/dl) No. Y (A液) 100 2.0 3.0 0.75 105.75 --- 200.0 Bicarbonate(B液) 0.0 650gm 混和後濃度 135.0 35.0
 No.X (A液) Bicarbonate(B液) 混和後濃度 改變後的透析液. 改變後的透析液. 品名 濃度(mEq/L) Na+ K+ Ca+2. Mg+2. Cl- CH3COO- HCO3- Dextrose(mg/dl) No. Y (A液) Bicarbonate(B液) gm. 混和後濃度")
24
抗凝劑在各種透析之應用 血液離開正常血管系統在體外循環與透析膜以及迴路管道接觸時很快就會凝結。
一般經常使用的抗凝劑為肝素(heparin),用肝素使血液凝固時間延長,稱之為肝素化法(heparinization)。
,用肝素使血液凝固時間延長,稱之為肝素化法(heparinization)。")
25
Heparin

26
肝素 帶陰電的粘液多醣類(mucopolysaccharide) 分子量為8,000到12,000 (6000-20000)道爾頓間
分子量大,在透析時不會透過透析膜 半衰期(half-1ife)為40 到 120分鐘 肝素注入血管內,作用很快出現 主要的作用:與抗凝血脢III (Antithrombin III)結合而加速阻斷凝血脢原(Prothrombin)變為凝血脢(Thrombin)。 Figure for heparin
為40 到 120分鐘. 肝素注入血管內,作用很快出現. 主要的作用:與抗凝血脢III (Antithrombin III)結合而加速阻斷凝血脢原(Prothrombin)變為凝血脢(Thrombin)。 Figure for heparin.")
27
肝素化法 1. 全身肝素化法(systemic heparinization)
B 低量肝素化法(Low dose heparinization) 2. 局部肝素化法(Regional heparinization)
 2. 局部肝素化法(Regional heparinization)")
28
一般的全身性肝素化法 Priming dose :依照各個廠牌的透析器決定 初載荷劑量(Initial loading dose)
第一次依照病人的體重以及所使用的透析器做初步的判斷 一般是讓血凝時間延長到原來病人的凝血時間的1.5倍至2倍 通常約需肝素量2,000至4,000 unit (國人遠低於此量)
")
29
一般的全身性肝素化法 在透析中可採用 通常在透析治療終了前一小時終止肝素的注射
持續性的注入法(continuous infusion) 間歇性注入法(intermittent infusion) 通常在透析治療終了前一小時終止肝素的注射 由於採用間歇性注入法,容易使病患處於肝素化過高或肝素化不足的變動中,故建議以持續性的注入法為佳
 間歇性注入法(intermittent infusion) 通常在透析治療終了前一小時終止肝素的注射. 由於採用間歇性注入法,容易使病患處於肝素化過高或肝素化不足的變動中,故建議以持續性的注入法為佳.")
30
血液透析中抗凝作用的評估方法 1. Clotting Time (Lee-White Clotting Time)
2. Activated Partial Thromboplastin Time(APTT): 正常 秒 3. Activated Clotting Time (ACT)活化凝血時間: 是目前用的最多,最簡易的方法。
: 正常 秒. 3. Activated Clotting Time (ACT)活化凝血時間: 是目前用的最多,最簡易的方法。")
31
Activated Clotting Time (ACT)活化凝血時間
參考值是 秒 秒 in MGH 秒 in CGMH 血液透析時理想的 ACT為 秒 Or 1.5 X to 2.0X Or 80%↑

32
Activated Clotting Time (ACT)活化凝血時間
非標準化(celite-based or kaolin-based) 比PTT較不精準 缺乏與PTT 或heparin anti-factor Xa levels相關性 受下列因素影響 血小板功能與數目 Lupus anticoagulant 凝血因子缺乏 週遭溫度 低血溫 血液稀釋
 比PTT較不精準. 缺乏與PTT 或heparin anti-factor Xa levels相關性. 受下列因素影響. 血小板功能與數目. Lupus anticoagulant. 凝血因子缺乏. 週遭溫度. 低血溫. 血液稀釋.")
33
活化血凝時間 (Activated Clotting Time)
使用不同廠牌的自動系統測定ACT,如HemoTec,TriMed,和Hemochron系統其時效性和靈敏度不同 對新開始作血液透析治療的病入,要測試一下此病人對肝素的敏感度及反應度 方法是先測定此病人的基礎血凝時間(未注肝素前),然後靜脈注入1500至2000單位的肝素,5分鐘後,每隔一小時,再抽血測定病人的血凝時間 注射肝素後與基礎血凝時間之差便是病人的反應度(R),此反應度除以肝素劑量便為敏感度(S)
,然後靜脈注入1500至2000單位的肝素,5分鐘後,每隔一小時,再抽血測定病人的血凝時間. 注射肝素後與基礎血凝時間之差便是病人的反應度(R),此反應度除以肝素劑量便為敏感度(S)")
34
Activated Clotting Time (ACT) 測定 HEMOCHRON 法
1 2 3 Add different machine, different result fig.

35
活化血凝時間 (Activated Clotting Time)
公式 Rt = R0e-Kt + (IRS/K)(1-e-Kt) 其中IR是肝素注入速率(IU/hr),配合依照每個小時注入肝素後求得的衰減係數之平均值 K’ = IRS(1-e-Kt) /(Rt-R0e-Kt),便可以求得初始劑量和每小時之注射量。 初始劑量 = 預期增加的凝血時間 / S 每小時之注射量 =預期增加的凝血時間 X K / S ADD PPI figure for illustration
(1-e-Kt) 其中IR是肝素注入速率(IU/hr),配合依照每個小時注入肝素後求得的衰減係數之平均值 K’ = IRS(1-e-Kt) /(Rt-R0e-Kt),便可以求得初始劑量和每小時之注射量。 初始劑量 = 預期增加的凝血時間 / S. 每小時之注射量 =預期增加的凝血時間 X K / S. ADD PPI figure for illustration.")
36
經驗法則 以初始劑量25-30 IU/K投予後,再調整
活化血凝時間 (ACT)一般基礎值為60-140秒(註),例行的透析希望透析中的ACT為 秒(+80%),結束時為 秒(+40%) 但是由於前述ACT有不同測定方法,有些測定基礎值如Hemochron 400 系統則為 秒
一般基礎值為60-140秒(註),例行的透析希望透析中的ACT為 秒(+80%),結束時為 秒(+40%) 但是由於前述ACT有不同測定方法,有些測定基礎值如Hemochron 400 系統則為 秒.")
37
防範凝固或出血失敗之原因 肝素投予量不正確 血管通路之問題 肝素抽取量錯誤 時間不足讓初始肝素劑量充分分布 無法提供適當的維持劑量
未適當填充透析器 動脈滴注腔有過多亂流 過多的再循環

38
低量肝素化法 (Low dose heparinization)
適用有出血傾向或是近期開刀,胃腸道出血,中樞神經系統出血以及心包膜炎等病患 肝素的初載荷劑量是10-25 IU/Kg,約為750-1,000 units,並在載荷劑量前以及載荷劑量後半小時測試一次血凝時間 理想血凝時間約為病人的原來血凝時間的1.5倍。 可用持續或間歇注入法,每小時約需往肝素11-22 IU/kg 或600-1,000 units以維持一定的血凝時間。

39
局部肝素化法(Regional heparinization)
適用於出血傾向或是有出血癥候的病人 肝素持續地注入動脈向路管內,而在血液流回病人體內之前,從靜脈向路管注入魚精蛋白(Protamine),以中和肝素 局部肝素化法比起低量肝素化法並無較多優點,故目前幾乎已經不被使用。
,以中和肝素. 局部肝素化法比起低量肝素化法並無較多優點,故目前幾乎已經不被使用。")
40
不須抗凝劑的血液透析 (Heparin-free hemodialysis)
適用高出血傾向的病人 將透析器及向路管先用肝素生理食鹽水(肝素3000單位每公升生理食鹽水)沖洗 透析時血流速最好每分鐘 ml 透析期間每半小時注入生理食鹽水 ml。 調整透析膜壓以適當地脫出過多的水份 方便而且安全
沖洗. 透析時血流速最好每分鐘 ml. 透析期間每半小時注入生理食鹽水 ml。 調整透析膜壓以適當地脫出過多的水份. 方便而且安全.")
41
肝素的併發症 偶有皮膚癢及發熱。 用量太多,會導致胃腸出血、眼底出血、臚內或硬腦膜下(subdural)出血
長時間的高劑量可能會引起骨質疏鬆症(osteoporosis)及高血脂症 如果因肝素過量而導致出血時,應立即停止肝素的給予,如嚴重時,可注射魚精蛋白以中和肝素的作用。
及高血脂症. 如果因肝素過量而導致出血時,應立即停止肝素的給予,如嚴重時,可注射魚精蛋白以中和肝素的作用。")
42
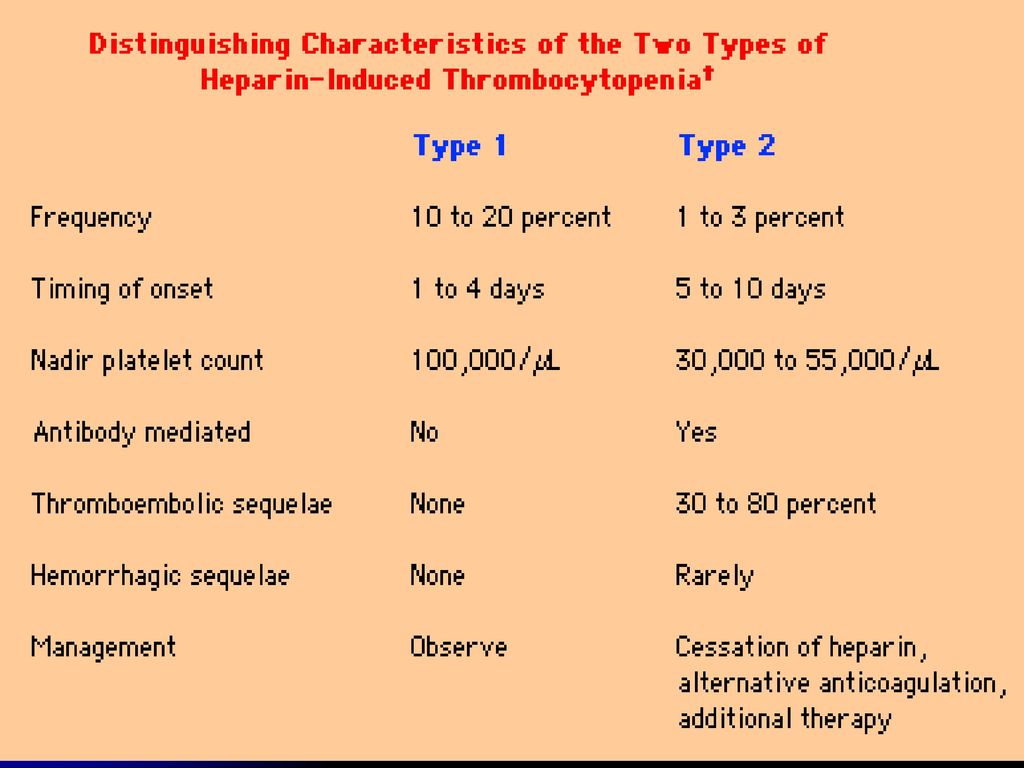
肝素 - 血小板過低 第一型 第二型 1至4天 5至10天 非免疫反應 免疫反應-抗體 血小板過低 血小板過低 + 動脈栓塞
Heparin + Platelet Factor 4 complex 血小板過低 + 動脈栓塞 Add one figure to illustrate

43
HIT antibodies directed against:
1. Epitopes within PF4 exposed when heparin-PF4 complexes have formed 2. Epitopes consisting partly of PF4 and heparin at points where the molecules are in close contact

45
Heparin: 連續性腎替代治療 (CRRT)(1)
肝素之使用於慢性連續性透析治療 (CAVHD, CVVHD) 與血液透析方法是相似的。 肝素可先給予 iu bolus loading後﹐持續給予10 u/kg/h或 u/h。 通常病患之間劑量差異可能相當大﹐故沒有固定不變之公式﹐而需因人而異。
 與血液透析方法是相似的。 肝素可先給予 iu bolus loading後﹐持續給予10 u/kg/h或 u/h。 通常病患之間劑量差異可能相當大﹐故沒有固定不變之公式﹐而需因人而異。")
46
Heparin: 連續性腎替代治療 (CRRT)(2)
通常每4-6小時監測一次APTT或ACT即可。 測血凝時間時以動脈端(肝素pump前)及靜脈端(透析器後)一併抽取﹐ 以APTT為例﹐肝素使動脈端維持小於45秒之延長﹐靜脈端維持大於60秒之延長為準。如需調整以100 u/h為調整基準。以ACT監測則維持正常之1.5倍至2倍左右。 低分子量肝素亦可使用於CRRT之治療
及靜脈端(透析器後)一併抽取﹐ 以APTT為例﹐肝素使動脈端維持小於45秒之延長﹐靜脈端維持大於60秒之延長為準。如需調整以100 u/h為調整基準。以ACT監測則維持正常之1.5倍至2倍左右。 低分子量肝素亦可使用於CRRT之治療.")
47
External Substitution On-Line HDF
Ficheux A, Kidney Int, 2000

48
Heparin Use in Hemodiafiltration(HDF)
Pre-dilution method may not need anticoagulant Post-dilution method need anticoagulation

49
Heparin in Hemoperfusion
More heparin needed than in hemodialysis because activated charcoal absorbs heparin Bolus heparin IU via arterial line Keep ACT 2x normal

50
低分子量肝素 low molecular weight heparin
分子量 道爾頓,黏液多醣體 作用於凝血因子Xa的專一性強 而不具備抑制thrombin的效果,所以不能使用傳統的血凝檢驗方法,必須採用專門檢驗anti-Xa因子活性的檢驗方法。 低分子量肝素作用時間長 (可達4小時以上)、人體生物相容性好、較不會出血,安全性高、方便等優點。 Add LMWH molecule fig
、人體生物相容性好、較不會出血,安全性高、方便等優點。 Add LMWH molecule fig.")
51
Figure 1.-Catalysis of Antithrombin-Mediated Inactivation of Thrombin or Factor Xa by Unfractionated Heparin or Low-Molecular-Weight Heparins. The interaction of unfractionated heparin and low-molecular-weight heparins with antithrombin is mediated by the pentasaccharide sequence of the drugs. Binding of either to antithrombin causes a conformational change at its reactive center that accelerates its interaction with factor Xa. Consequently, both unfractionated heparin and low-molecular-weight heparins catalyze the inactivation of factor Xa by antithrombin. In contrast to factor Xa inhibition, catalysis of antithrombin-mediated inactivation of thrombin requires the formation of a ternary heparin-antithrombin-thrombin complex. This complex can be formed only by chains at least 18 saccharide units long. This explains why low-molecular-weight heparins have less inhibitory activity against thrombin than unfractionated heparin. From: Weitz: N Engl J Med, Volume 337(10).September 4, Weitz, J I. Drug Therapy: Low-Molecular-Weight Heparins NEJM 1997;337:688

52
低分子量肝素 low molecular weight heparin
其半衰期為傳統肝素的的2倍,約80-200分鐘 每次血液透析使用劑量平均為 anti-Xa ICU/Kg不等 血液透析時,可以單劑量自動脈廔管迴路注射,維持足夠的抗凝血作用。或以一半當載荷劑另剩一半平均每小時加以靜脈滴往, 在透析結束前1-2小時即可關掉滴往的幫浦。

53
低分子量肝素 80-90%經由腎臟排出,小部份經由肝臟排出 病患腎功能不好,則須減少使用劑量。 出血機率較傳統肝素發生少
血小板稀少的現象及骨頭疏鬆的併發症較減少 低分子量肝素可暫時性被魚精蛋白(Protamine sulfate)中和 傳統肝素長期使用會引起高血脂症,而低分子量肝素長期使用 (?)
中和. 傳統肝素長期使用會引起高血脂症,而低分子量肝素長期使用 ( )")
54
其他抗凝劑 Argatroban: synthetic direct thrombin inhibitor derived from L-arginine. 檸檬酸三鈉 (trisodium citrate) Prostacyclin (PG I2) Danaparoid Hirudin
 Danaparoid. Hirudin.")
55
Prostacyclin (PG I2) (arachidonic acid) 的代謝物,主要在血管內皮細胞合成,是強力的血管擴張劑和血小板凝集抑制劑。 在體內的半衰期 (half-life) 約3.5分。 缺點: 化學上不安定,有頭痛、嘔心、嘔吐、臉部潮紅和血壓下降的副作用。

56
Danaparoid heparan sulfate,dermatan sulfate,和chondroitin sulfate的混合物。
其不含有肝素和低分子量肝素,可以避免肝素引起的血小板稀少(HIT)的現象。 半衰期長,為避免流血併發症,必須檢測anti-Xa 因子活性。
的現象。 半衰期長,為避免流血併發症,必須檢測anti-Xa 因子活性。")
57
Regional citrate anticoagulation
Infusion of trisodium citrate solution into the arterial side of the dialyzer The citrate-calcium complex is removed across the dialyzer keep the ACT above 200 seconds in the arterial limb Risk: Alkalosis, Hypocalcemia, Hypernatremia

58
Anticoagulants for Catheter lumen
Heparin 1000 U/ml 5000 U/ml High concentration- 30% or 43% Trisodium Citrate Anti-bacterial effect Risk of hypocalcemia? Weijmer MC J Am Soc Nephrol Sep;16(9):
:")
59
No difference in catheter-associated bacteremia.
Figure 1. Kaplan-Meier survival curve for time to catheter dysfunction Citrate 4% versus Heparin No difference in catheter-associated bacteremia. No difference in catheter-associated bacteremia. MacRae, J. M. et al. Clin J Am Soc Nephrol 2008;3:

60
Hirudin Hirudin – thrombin: noncovalent binding
Recombinant hirudin (Lepirudin): could be applied in dialysis Prolonged half life in uremic patients.
: could be applied in dialysis. Prolonged half life in uremic patients.")
61
Proportion of massive clotting versus time after inclusion in the protocol
Chanard, J. et al. Nephrol. Dial. Transplant. 2007

62
Figure 1. Kaplan-Meier analysis of survival by drug therapy
Chan, K. E. et al. J Am Soc Nephrol 2009;20:

63
Thank You for Your Attention!

Similar presentations




 病理生理学系 Department of Pathophysiology 高远生.>")









>")



 止血(hemostasis)>")

