Download presentation
Presentation is loading. Please wait.

1
Transfusion Therapy 章人欽 醫師 高雄捐血中心 台灣血液基金會

2
Outline Blood provision About blood products
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products Blood administration

3
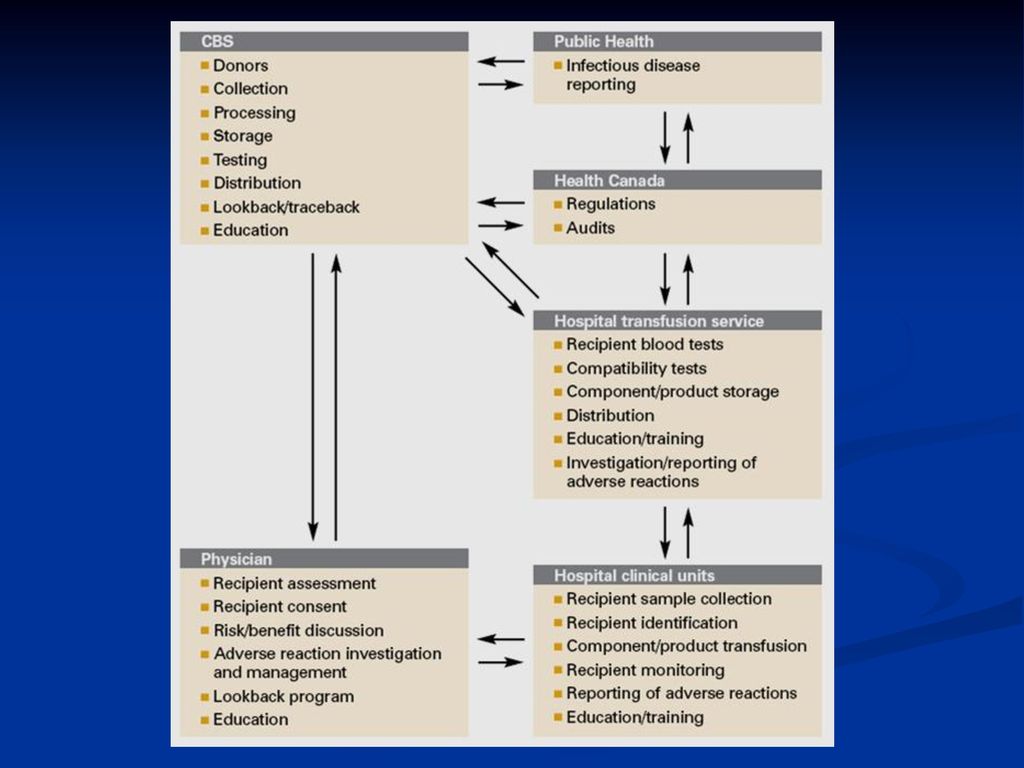
Blood Safety Donor education recruitment screening Storage
Distribution Transportation Bedside use Blood collection Testings NAT Prestorage LR (CMV ,Alloimmune,FNHTR) Pathogen reduction Donor Retest 1. Appropriate Use of Blood component 2. Hemovigilance System 3. Look back Monitor of temperature Inspection Storage time Skin disinfection compliance with SOP C.U.E Donor suitability Quarantined, Retrieve Donor remark
 Pathogen. reduction. Donor Retest. 1. Appropriate. Use of Blood. component. 2. Hemovigilance. System. 3. Look back. Monitor of. temperature. Inspection. Storage time. Skin disinfection. compliance with. SOP. C.U.E. Donor. suitability. Quarantined, Retrieve. Donor remark.")
5
Blood provision Pretransfusion sample
Collector Venipuncture will only be performed by an appropriately trained pathology collector, medical officer, registered nurse or anaesthetic or theatre technician, or a trainee in direct supervision of one of the above. Patients must be identified before sample collection Ask the patient (or parent) to state their name, date of birth and address (outpatients) Inspect the patient ID bracelet (inpatients) and confirm that these details match those on the request form Correctly identifying the patient during collection of the pretransfusion sample is vital in avoiding 'wrong blood to wrong patient' episodes.
 to state their name, date of birth and address (outpatients) Inspect the patient ID bracelet (inpatients) and confirm that these details match those on the request form. Correctly identifying the patient during collection of the pretransfusion sample is vital in avoiding wrong blood to wrong patient episodes.")
6
Blood provision Pretransfusion sample Specimen labelling
must be labelled at the bedside before leaving the patient specimens must have the following identifiers Full Name (Surname and First name) Date of birth UR number (if known) Date and time of collection Collectors signature or initial on the request form labelling of tubes in advance of collection is not acceptable due to the risk of patient specimen mismatch Use of pre-printed bradma labels is permissible but only if they also bear the signature of the collector and date and time of collection. Care must be taken to ensure the correct bradma label is applied. Details on the bradma must be identical with those on the patient wristband. All details must correspond completely and accurately between the sample and the request form. Where inconsistencies of spelling or numerical inaccuracy are present, the specimen will not be processed and the requesting medical officer will be notified to obtain a repeat sample.
 Date of birth. UR number (if known) Date and time of collection. Collectors signature or initial on the request form. labelling of tubes in advance of collection is not acceptable due to the risk of patient specimen mismatch. Use of pre-printed bradma labels is permissible but only if they also bear the signature of the collector and date and time of collection. Care must be taken to ensure the correct bradma label is applied. Details on the bradma must be identical with those on the patient wristband. All details must correspond completely and accurately between the sample and the request form. Where inconsistencies of spelling or numerical inaccuracy are present, the specimen will not be processed and the requesting medical officer will be notified to obtain a repeat sample.")
7
Blood provision Pretransfusion testing Group and Screen
Determines the ABO and Rh(D) group Antibody screen to detect red cell antibodies Checking for previous transfusion and blood group records 1. For patients who have "no red cell antibodies detected", a crossmatch is performed to ensure compatibility of blood prior to issue of donor units 2. For patients who have "red cell antibodies detected", further laboratory work is required to identify the specificity of the antibody, to type the patient and donor units in order to provide specific antigen negative blood and to perform a full serological crossmatch. For patients with multiple antibodies this work can take several hours to complete.
 group. Antibody screen to detect red cell antibodies. Checking for previous transfusion and blood group records. 1. For patients who have no red cell antibodies detected , a crossmatch is performed to ensure compatibility of blood prior to issue of donor units. 2. For patients who have red cell antibodies detected , further laboratory work is required to identify the specificity of the antibody, to type the patient and donor units in order to provide specific antigen negative blood and to perform a full serological crossmatch. For patients with multiple antibodies this work can take several hours to complete.")
8
Blood provision Issue of blood products from the blood bank
Blood products should only be picked up when the transfusion is ready to commence in order to ensure appropriate storage of blood products. Blood products must not be stored in ward areas or domestic fridges. If the transfusion cannot commence within 30 minutes, the product must be returned to blood bank for storage

9
高醫輸血作業流程

10
不要愛睏喔 !!!

11
About blood products Blood products Blood product modifications
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products

12
Blood Groups and Compatibilities
Many blood groups including ABO, Rh, Kidd, Kell, Duffy, MNS and Lewis The most important of these are ABO and RhD Transfusion with ABO incompatible blood can lead to severe and potentially fatal transfusion reactions RhD is highly immunogenic and can lead to red cell hemolysis in certain settings

13
Blood Groups and Compatibilities
ABO Blood Groups Blood Group ABO antigens present on the red cell surface ABO antibodies present in the plasma Type O nil anti-A and anti-B Type A A antigen anti-B Type B B antigen anti-A Type AB A and B antigens

14
Blood Groups and Compatibilities
Rhesus D (RhD) Antigen More than 40 different kinds of Rh antigens The most significant Rh antigen is RhD. When RhD is present on the red cell surface, the red cells are called RhD positive. Antibodies to RhD develop only after an individual is exposed to RhD antigens via transfusion, pregnancy or organ transplantation. As a general rule, RhD negative individuals should not be transfused with RhD positive red cells, especially RhD negative girls and women of childbearing age.
 Antigen. More than 40 different kinds of Rh antigens. The most significant Rh antigen is RhD. When RhD is present on the red cell surface, the red cells are called RhD positive. Antibodies to RhD develop only after an individual is exposed to RhD antigens via transfusion, pregnancy or organ transplantation. As a general rule, RhD negative individuals should not be transfused with RhD positive red cells, especially RhD negative girls and women of childbearing age.")
15
Blood Groups and Compatibilities
Blood Compatibility - Are they Compatible? Patient Type Compatible Red Cell Types Compatible Plasma Types (FFP & Cryoprecipitate) A A, O A, AB B B, O B, AB O O, A, B, AB AB AB, A, B, O AB RhD Positive RhD Positive RhD Negative RhD Positive RhD Negative RhD Negative Group AB individuals have neither anti-A nor anti-B antibodies in their plasma. Group AB plasma can therefore be given to patients of any ABO blood group and is often referred to as the universal plasma donor.
 A. A, O. A, AB. B. B, O. B, AB. O. O, A, B, AB. AB. AB, A, B, O. AB. RhD Positive. RhD Positive RhD Negative. RhD Positive RhD Negative RhD Negative. Group AB individuals have neither anti-A nor anti-B antibodies in their plasma. Group AB plasma can therefore be given to patients of any ABO blood group and is often referred to as the universal plasma donor.")
16
Blood Groups and Compatibilities
Avoiding ABO Incompatible Transfusions Most ABO incompatible transfusions occur as a result of improper patient identification at the time of collection of the pre-transfusion sample or administration of the blood product. The pre-transfusion check is carried out at the bedside by 2 members of clinical staff to ensure the right blood is transfused to the right patient. Positive patient identification prior to blood sample collection and labelling the specimen tube at the bedside is critical for accurate sample collection

17
About blood products Blood products Blood product modifications
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products

18
血液成份療法 (Blood Component Therapy)
")
19
血液成份製備流程圖

20
冷凍血漿 冷凍血漿 血漿 冷凍沉澱品 新鮮冷凍血漿 血漿 全血 白血球濃厚液 紅血球濃厚液 血小板濃厚液 富含血小板之血漿 新鮮冷凍血漿
8hr後分離 冷凍沉澱品 新鮮冷凍血漿 冷凍 血漿 8hr內分離 解凍離心 全血 白血球濃厚液 紅血球濃厚液 Buffy coat 20-24。C, 6hr 內分離 血小板濃厚液 富含血小板之血漿 新鮮冷凍血漿 6-8hr內製備

21
血液成份之貯存 全血 CPDA-1 35天 1º~6 ℃ 紅血球濃縮液 CPDA-1 乏白血球紅血球 1º~6 º 血小板 3-5天
20 º~24℃(室溫) 白血球 24小時 20 º~24℃ 新鮮冷凍血漿 1年 -20℃以下 冷凍血漿 5年 冷凍沉澱品
 白血球. 24小時. 20 º~24℃ 新鮮冷凍血漿. 1年. -20℃以下. 冷凍血漿. 5年. 冷凍沉澱品.")
22
為什麼使用血液成份療法? 針對病人的特殊醫療需要,給予所缺的成份,並且將不必要的成份濃度降至最低。 有效率地利用給血者的資源。

23
新鮮全血 (Fresh Whole Blood)
說明: 自捐血日起3天內之全血稱為新鮮全血。 紅血球約100 ml,血漿150 ml,抗凝劑35 ml,捐血後第二天尚含所有凝血因子,白血球及血小板,Ht 32-42%。 容量:285 ml 貯存 / 期效:4℃,35天

24
新鮮全血 (Fresh Whole Blood)
功能:每單位全血可提升Hb 0.5g / dl,含有適量的2, 3 - DPG可增加釋氧能力,並含適當之電解質濃度。 適應症: 新生兒輸血 新生兒換血治療 小兒科心臟血管手術

25
全血 (Stored Whole Blood)
主要成份:紅血球100 ml,血漿150 ml,抗凝劑35 ml,安定凝血因子120單位,Ht %。但缺少factor Ⅴ、 Ⅷ 等不穩定因子,雖含白血球及血小板,但無功能。 容量:285 ml 貯存/期效:4℃,35天 功能:每單位全血可提升Hb 0.5 g / dl,補充紅血球以增加攜氧能力,及擴張循環容積。

26
全血 (Stored Whole Blood)
適應症: 休克伴隨急性大量出血或手術中出血大於1000 ml或失血量大於全血量之30 % 時,可輸給全血,而全血量 = 體重(kg)x 70 ml。 但因儲存3天以上的全血所含不安定凝血因子Ⅴ、Ⅷ 及血小板均功能大減,故出血時,仍建議採用血液成份療法取代全血,可同時輸給病患packed RBC、FFP、和 platelet concentrate。 1000ml以內的失血,只需輸給packed RBC。
x 70 ml。 但因儲存3天以上的全血所含不安定凝血因子Ⅴ、Ⅷ 及血小板均功能大減,故出血時,仍建議採用血液成份療法取代全血,可同時輸給病患packed RBC、FFP、和 platelet concentrate。 1000ml以內的失血,只需輸給packed RBC。")
27
紅血球濃厚液(Packed RBC) 主要成份:紅血球約100 ml,血漿40 ml,安定凝血因子40 單位,亦含白血球及血小板,但無功能。
貯存 / 期效:4℃,35 天 功能:每單位血可提升 Hb 0.5 g / dl,可補充紅血球之攜氧能力。

28
紅血球濃厚液(Packed RBC) 適應症: 1. 500 ml以上的出血 2. 具症狀的貧血不能用外科治療 (脾切除)或
內科治療(iron、folate、維生素B12等) 改 善之情況。 3. Hb < 9 g / dl 時,包括開刀麻醉前必須矯正 的貧血,癌症病患,有症狀的心臟衰竭病 人,angina 的病人及慢性肺阻塞病人。 4. Hb < 8 g / dl 時,如長期慢性貧血病人。
 改. 善之情況。 3. Hb < 9 g / dl 時,包括開刀麻醉前必須矯正. 的貧血,癌症病患,有症狀的心臟衰竭病. 人,angina 的病人及慢性肺阻塞病人。 4. Hb < 8 g / dl 時,如長期慢性貧血病人。")
29
洗滌紅血球濃厚液 (Washed RBC) 主要成份: 容量:130 ml 貯存 / 期效:4℃,24小時
紅血球約 90 ml,含少量白血球 (每單位約含 WBC 1 x 108,即移除原有的 WBC的90%),亦含少量血小板 ,缺乏血漿及凝血因子。 容量:130 ml 貯存 / 期效:4℃,24小時
,亦含少量血小板 ,缺乏血漿及凝血因子。 容量:130 ml. 貯存 / 期效:4℃,24小時.")
30
洗滌紅血球濃厚液 (Washed RBC) 功能:每單位血可提升 Hb 0.5g / dl 適應症: 1. 血漿蛋白過敏(全身性蕁麻疹反應,
IgA 缺乏症) 2. 白血球抗體引起發燒發冷輸血反應 3. 陣發性夜間血紅素尿症(PNH)
 2. 白血球抗體引起發燒發冷輸血反應. 3. 陣發性夜間血紅素尿症(PNH)")
31
冷凍去甘油紅血球濃厚液 (Frozen Deglyceride RBC)
主要成份: 紅血球約90 ml,缺血漿,凝血因子,白血球及血小板,攜氧能力與新鮮全血相近。 容量:120 ml 貯存 / 期效: - 65℃,10年,解凍後置於 4 ℃,24小時

32
冷凍去甘油紅血球濃厚液 (Frozen Deglyceride RBC)
功能:每單位可提升Hb 0.5 g / dl 適應症: 1. 稀有血型病患之輸血 2. 具多項異體抗體病人的輸血之自體輸血 3. 陣發性夜間血紅素尿症(PNH)
")
33
減除白血球之紅血球濃厚液(Leukocyte-Poor RBC)
主要成份: 將2U之紅血球濃厚液(含SAGM),經白血球過濾器(filter)去除絕大部分白血球而成, 每袋WBC<5x106。 容量:200~350 ml/袋 (2U) 貯存/期效:1~6℃,採血後42天
,經白血球過濾器(filter)去除絕大部分白血球而成, 每袋WBC<5x106。 容量:200~350 ml/袋 (2U) 貯存/期效:1~6℃,採血後42天.")
34
減除白血球之紅血球濃厚液(Leukocyte-Poor RBC)
功能: 每單位可提升 Hb 0.5g / dl 可預防 Febrile nonhemolytic transfusion reaction,HLA alloimmunization,CMV,HTLV-Ⅰ之感染 可能預防 GVHD

35
減除白血球之紅血球濃厚液(Leukocyte-Poor RBC)
適應症: 1. 需長期輸血,如chemotherapy,thalassemia,aplastic anemia,dyserythropoiesis的病人。 2. 避免TA-GVHD。 3. 避免因輸血引起CMV感染,如器官移植病 患,骨髓移植病患,新生兒及免疫不全之病患。(須 WBC < 1 x 107) 4. 發燒發冷反應二次以上,需再次輸血。
 4. 發燒發冷反應二次以上,需再次輸血。")
36
新鮮冷凍血漿(Fresh Frozen Plasma)
主要成份: 自250ml全血採集後8小時內所分離之血漿,經急速冷凍而成,保存了所有血液凝固因子,包括第V及VIII等不安定性因子。 容量: ml 貯存 / 期效:-18℃,1年, 經 30 ~ 37℃解凍後輸用。

37
新鮮冷凍血漿(FFP)之適應症: 1. Anti-thrombin Ⅲ缺乏
2. Coagulation factor 如Ⅱ、Ⅴ、Ⅶ、Ⅷ、IX、X、XIII 之缺乏 3. Coumadin引起的副作用 4. DIC,TTP,hemolytic-uremic syndrome 5. 大量輸血所造成凝血因子的稀釋 6. 因肝病而引發多項凝血因子缺乏 7. 新生兒的換血或輸血

38
Transfusion audit of fresh-frozen plasma in southern Taiwan
The indications for FFP included the following: surgery and invasive treatment of patients who had activated partial thromboplastin time (APTT) and prothrombin time (PT) elevated to 1·5 times the normal level, with a bleeding tendency disseminated intravascular coagulation (DIC) plasma exchange for thrombotic thrombocytopenic purpura (TTP) massive transfusion with coagulopathy exchange transfusion for newborns Vox Sanguinis (2006) 91, 270–274
 and prothrombin time (PT) elevated to 1·5 times the normal level, with a bleeding tendency. disseminated intravascular coagulation (DIC) plasma exchange for thrombotic thrombocytopenic purpura (TTP) massive transfusion with coagulopathy. exchange transfusion for newborns. Vox Sanguinis (2006) 91, 270–274.")
39
The change in red blood cell (RBC)-to-plasma ratio and inappropriate requests for fresh frozen plasma (FFP), before and after the intervention Transfusion audit of fresh-frozen plasma in southern Taiwan Vox Sanguinis (2006) 91, 270–274
 91, 270–274.")
40
Internal Medicine Journal 2005; 35: 283–288

41
Internal Medicine Journal 2005; 35: 283–288

42
冷凍血漿(Frozen Plasma) 主要成份:含安定凝血因子約 90單位,缺factor Ⅴ、Ⅷ,亦無血小板及白血球。
容量: ml 貯存 / 期效:-18℃,五年 功能:補充穩定性凝血因子。 適應症: 須緊急中止口服抗凝劑(warfarin) 之抗凝效果時 某些疾病之血漿交換治療
 之抗凝效果時. 某些疾病之血漿交換治療.")
43
冷凍血漿(FP) Practice Guidelines for Blood Transfusion
2007 American National Red Cross

44
冷凍血漿(FP) Practice Guidelines for Blood Transfusion
2007 American National Red Cross

45
冷凍沉澱(Cryoprecipitates)
製作及成份: 全血採血後8小時內依新鮮冷凍血漿分離程序於-80℃冷凍櫃或乾冰酒精浴中急速冷凍後,於1-6℃解凍再經離心分離移除血漿後的餘留不溶物,懸浮於血漿中;於1小時內再冷凍於-20℃以下。 每單位約含45IU的factor VIII,125mg纖維蛋白原,40IU von-Willebrand因子,fibronectin 23mg及20-30IU factor XIII 容量:15~20 ml 貯存 / 期效:-20℃,1年

46
冷凍沉澱(Cryoprecipitates)
適應症: 1. Coagulation factor Ⅷ 缺乏 2. Von Willebrand’s disease 3. DIC,Sepsis 4. Hypofibrinogenemia (fibrinogen≦100 mg / dl,若出血時,則≦150 mg / dl)
")
47
血小板濃厚液(Platelet Concentrate)
分為兩類,主要成份: (a) 傳統血小板濃厚液,每1單位中含 血小板約 2~3 x 1010,並含少量白血球及紅血球。 (b) 分離術血小板(相當於12單位傳統血小板) ,每袋含 血小板 3 x 1011,亦含少量白血球及紅血球。 容量:(a) 30 ~ 40 ml (b) 200 ~ 300 ml 貯存 / 期效:20~24℃恆溫振盪器內,5 天 功能:(a) 每單位可提升血小板數 2500 /μl (b) 每單位可提升血小板數 /μl
 傳統血小板濃厚液,每1單位中含. 血小板約 2~3 x 1010,並含少量白血球及紅血球。 (b) 分離術血小板(相當於12單位傳統血小板) ,每袋含. 血小板 3 x 1011,亦含少量白血球及紅血球。 容量:(a) 30 ~ 40 ml (b) 200 ~ 300 ml. 貯存 / 期效:20~24℃恆溫振盪器內,5 天. 功能:(a) 每單位可提升血小板數 2500 /μl. (b) 每單位可提升血小板數 /μl.")
48
血小板濃厚液 (Platelet Concentrate)
適應症: 1. 血小板 < 10,000 – 20,000 /μl, 白血病,癌症 之治療,再生不良性貧血 2. 血小板 < 80, ,000 /μl, 要腦部開刀的 病人 3. 血小板 < 50,000 /μl, 接受外科手術之病人 4. 血小板 < /μl, 具出血傾向,應提升至5萬

49
血小板濃厚液 (Platelet Concentrate)
適應症: 5. 大量輸血及DIC,因缺少血小板引起 的出血,ITP有危及生命的出血 6. 先天性血小板機能不良者 7. 後天性血小板機能不良者(uremia) 8. 心臟手術使用心肺機引起血小板功能不良
 8. 心臟手術使用心肺機引起血小板功能不良.")
50
Platelet Product Group
Platelet transfusion Blood Group? Principles Patient’s ABO Group Platelet Product Group First Choice Second Choice Third Choice O A B AB B or A

51
Platelet transfusion Platelet Administration
Use a fresh administration set for platelets. Do not transfuse though a standard filter straight after red cells as platelets will get caught up in fibrin strands /debris etc. Platelet transfusion must be completed within 4 hours of spiking pack. Occasionally platelets are given over 30 minutes, but this may contribute to an increased risk of some reactions (fever/chill) and fluid overload. In patients receiving multiple other fluids etc give at a rate of 3ml/kg/hr over 2-3 hours.
 and fluid overload. In patients receiving multiple other fluids etc give at a rate of 3ml/kg/hr over 2-3 hours.")
52
白血球濃厚液 (White Blood Cells Concentrate)
血液採集6小時內,將室溫(20~24°C)存放之新鮮血液離心分離出之buffy coat稱之 成分:1單位 - 250ml全血製作而來,體積20~30ml,含1x109 白血球,混含部份血小板及紅血球 貯存 / 期效: 20~24℃,24小時,在6小時內 儘速輸用。
存放之新鮮血液離心分離出之buffy coat稱之. 成分:1單位 - 250ml全血製作而來,體積20~30ml,含1x109 白血球,混含部份血小板及紅血球. 貯存 / 期效: 20~24℃,24小時,在6小時內. 儘速輸用。")
53
白血球濃厚液 (WBC Concentrate)
功能: 治療 neutropenia 時合併之嚴重細菌或黴菌感染。 適應症:病人需要有所有下列的情形, 1. 嗜中性球減少症 ( neutrophils < 500 /μl)。 2. 持續高燒 24小時,以第3代抗生素治療無效者。 3. 骨髓檢查顯示 myeloid series 再生不良。 4. 病人骨髓功能有復原的機會。
。 2. 持續高燒 24小時,以第3代抗生素治療無效者。 3. 骨髓檢查顯示 myeloid series 再生不良。 4. 病人骨髓功能有復原的機會。")
54
白血球濃厚液 (WBC Concentrate)
注意事項: 1.此血液製品中混有血小板濃厚液,對病人有 益,因缺乏白血球的病人亦常缺乏血小板。 2.連續輸用一星期後,觀察病人恢復的情況,有部分病人發生持續高燒及嚴重肺部反應,此時應立即停止輸用白血球。 3.輸白血球濃厚液和輸血漿相同,亦有疾病傳播的危險。 4.不需做預防的輸注。

55
Volumes and rates for transfusion of blood products

56
很專心喔!!

57
About blood products Blood products Blood product modifications
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products

58
Blood product modifications
Irradiation of blood products by gamma irradiation of cellular blood products (whole blood, red blood cells, platelets, granulocytes) using a dedicated blood irradiator with a long half-life gamma emitting source to prevent Transfusion Associated Graft-Versus Host Disease (TA-GVHD) occurs days post transfusion fever, skin rash, hepatitis, diarrhea and pancytopenia fatal in more than 90% of cases
 using a dedicated blood irradiator with a long half-life gamma emitting source. to prevent Transfusion Associated Graft-Versus Host Disease (TA-GVHD) occurs days post transfusion. fever, skin rash, hepatitis, diarrhea and pancytopenia. fatal in more than 90% of cases.")
59
Blood product modifications
Irradiation of blood products Irradiation of RBCs and whole blood results in reduced post transfusion red cell recovery and increases the rate of efflux of intracellular potassium no clinically significant effect on red cell pH, glucose, 2,3 DPG levels or ATP Packs irradiated within 14 days of collection expire 28 days after collection Packs irradiated more than 14 days after collection expire either 5 days after irradiation OR at original expiry of pack, whichever comes first In patients where hyperkalemia is a concern, red cells should be transfused within 24 hours of irradiation. Examples include large volume neonatal transfusion such as exchange transfusion, ECMO or rapid large volume transfusion

60
Blood product modifications
Irradiation of blood products Irradiation of platelets has not been shown to cause any clinically significant change in platelet function. Platelets may be irradiated at any stage during their 5 day storage life. Irradiation of granulocytes conflicting evidence of irradiation damage to granulocytes. Granulocytes should be transfused as soon as possible after collection and irradiation.

61
Blood product modifications
Irradiation of blood products Labelling

62
About blood products Blood products Blood product modifications
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products

63
Blood product modifications
Leucocyte depletion - 1 Removal of white cells from cellular blood products (whole blood, red blood cells, platelets) to a level of <1 x 106 per pack Why? Reduces alloimmunisation and platelet refractoriness Reduces frequency of recurrent febrile reactions Reduces the risk of CMV transmission Reduces the risk of potential immunomodulatory effects Patients transfused with standard red cell and platelet products are exposed to large numbers of leucocytes (~1x109 per adult pack) which are responsible for some transfusion complications. The established indications for using leucocyte depleted blood products include: To prevent or delay alloimmunisation and platelet refractoriness Alloimmunisation is defined as the development of antibodies to red cell, white cell or platelet antigens and is related to the patient's history of previous blood transfusions and pregnancies. White cells strongly express HLA class I antigens and may stimulate HLA antibodies in some individuals. HLA alloimunisation can be associated with platelet refractoriness (failure to obtain satisfactory responses to platelet transfusions) and organ transplant rejection. Leucocyte depletion of blood products can reduce the incidence of alloimmunisation and platelet refractoriness. Reducing the risk of alloimmunisation is particularly important in patients where alloimmunisation may compromise the success of future transplantation, e.g. patients with severe aplastic anaemia or sickle cell disease. See alloimmunisation To reduce recurrent febrile non-haemolytic transfusion reactions Febrile non-haemolytic transfusion reactions (FNHTR) are more commonly associated with platelet rather than red cell transfusion and have been reported to occur with an incidence of 37.5% after platelet transfusion. The major cause of platelet related FNHTR is thought to be due to the presence of cytokines released from white cells in the platelet product during storage. Removal of leucocytes by Australian Red Cross Blood Society (ARCBS) soon after the blood is collected from the donor (prestorage leucocyte depletion) is more likely to reduce the occurrence of platelet related FNHTR than leucocyte depletion at the bedside (bedside leucocyte depletion). Recurrent (2 or more) FNHTR to red cells are probably caused by HLA alloimmunisation rather than cytokines and can be effectively prevented by bedside leucocyte depletion. To reduce the risk of CMV transmission Transfusion transmitted CMV infection can cause significant morbidity and mortality in the fetus, neonate or immunocompromised CMV seronegative patient. The use of CMV seronegative blood components has been shown to significantly reduce the incidence of CMV infection in at risk groups. Although conclusive evidence from randomized trials proving equivalence of leucocyte depleted and CMV seronegative blood products is lacking, when CMV seronegative products are not available, leucocyte depleted products should be selected. In this setting, leucocyte depleted products offer a high level of safety in preventing CMV transmission. Leucocyte depletion using current technology is inadequate for preventing Transfusion Associated-Graft Versus Host Disease (TA-GVHD). TA-GVHD is prevented by gamma irradiation of blood products. See Irradiation of Blood Products.
 to a level of <1 x 106 per pack. Why Reduces alloimmunisation and platelet refractoriness. Reduces frequency of recurrent febrile reactions. Reduces the risk of CMV transmission. Reduces the risk of potential immunomodulatory effects. Patients transfused with standard red cell and platelet products are exposed to large numbers of leucocytes (~1x109 per adult pack) which are responsible for some transfusion complications. The established indications for using leucocyte depleted blood products include: To prevent or delay alloimmunisation and platelet refractoriness Alloimmunisation is defined as the development of antibodies to red cell, white cell or platelet antigens and is related to the patient s history of previous blood transfusions and pregnancies. White cells strongly express HLA class I antigens and may stimulate HLA antibodies in some individuals. HLA alloimunisation can be associated with platelet refractoriness (failure to obtain satisfactory responses to platelet transfusions) and organ transplant rejection. Leucocyte depletion of blood products can reduce the incidence of alloimmunisation and platelet refractoriness. Reducing the risk of alloimmunisation is particularly important in patients where alloimmunisation may compromise the success of future transplantation, e.g. patients with severe aplastic anaemia or sickle cell disease. See alloimmunisation. To reduce recurrent febrile non-haemolytic transfusion reactions Febrile non-haemolytic transfusion reactions (FNHTR) are more commonly associated with platelet rather than red cell transfusion and have been reported to occur with an incidence of 37.5% after platelet transfusion. The major cause of platelet related FNHTR is thought to be due to the presence of cytokines released from white cells in the platelet product during storage. Removal of leucocytes by Australian Red Cross Blood Society (ARCBS) soon after the blood is collected from the donor (prestorage leucocyte depletion) is more likely to reduce the occurrence of platelet related FNHTR than leucocyte depletion at the bedside (bedside leucocyte depletion). Recurrent (2 or more) FNHTR to red cells are probably caused by HLA alloimmunisation rather than cytokines and can be effectively prevented by bedside leucocyte depletion. To reduce the risk of CMV transmission. Transfusion transmitted CMV infection can cause significant morbidity and mortality in the fetus, neonate or immunocompromised CMV seronegative patient. The use of CMV seronegative blood components has been shown to significantly reduce the incidence of CMV infection in at risk groups. Although conclusive evidence from randomized trials proving equivalence of leucocyte depleted and CMV seronegative blood products is lacking, when CMV seronegative products are not available, leucocyte depleted products should be selected. In this setting, leucocyte depleted products offer a high level of safety in preventing CMV transmission. Leucocyte depletion using current technology is inadequate for preventing Transfusion Associated-Graft Versus Host Disease (TA-GVHD). TA-GVHD is prevented by gamma irradiation of blood products. See Irradiation of Blood Products.")
64
Blood product modifications
Leucocyte depletion - 2 Which patients? Immunocompromised patients Hematology/Oncology patients Malignancy Transplant recipients (bone marrow and solid organ) Severe Combined Immune Deficiency Syndrome (SCIDS), Common Variable Immune Deficiency (CVID) Patients requiring chronic transfusion Patients less than 12 months of age Intrauterine and exchange transfusions
 Severe Combined Immune Deficiency Syndrome (SCIDS), Common Variable Immune Deficiency (CVID) Patients requiring chronic transfusion. Patients less than 12 months of age. Intrauterine and exchange transfusions.")
65
Blood product modifications
Leucocyte depletion - 3 Which filter should I use?

66
Blood product modifications
Leucocyte depletion - 4 Fresh Frozen Plasma (FFP) and cryoprecipitate have extremely low numbers of viable cells and do not require leucocyte depletion - they should be administered via a standard filter.
 and cryoprecipitate have extremely low numbers of viable cells and do not require leucocyte depletion - they should be administered via a standard filter.")
67
白血球去除過濾器之使用

68
白血球去除過濾器之使用

69
Accumulation of extracellular sVEGF (ng/unit) in WB and SAGM blood during storage for 35 days at 4°;C. Transfusion, Vol. 39, No. 10, , October 1999

70
有這樣舒服嗎?

71
Outline Blood provision About blood products
Blood Groups and Compatibilities Blood Component Therapy Blood product modifications Irradiation of blood products Leucocyte depletion of blood products Blood administration

72
Blood administration Patient preparation Pretransfusion check
Blood Transfusion Record Transfusion Tag Care and monitoring of transfused patients

73
Blood administration Patient Preparation appropriate IV access
written order for transfusion benefits/risks of transfusion discussed an opportunity to have any questions answered

74
Blood administration Pretransfusion check - 1 Safe transfusion
a final patient identity check at the patient bedside before blood administration to ensure the right blood is given to the right patient. Signing the blood transfusion record the check has been completed prior to transfusion no discrepancy was identified

75
Blood administration Pretransfusion check - 2
Check blood product for any signs of leakage, clumps or abnormal color Patient identification Check name, DOB and UR on the Blood Transfusion Record and pack tag/label and on the patient's wristband. Are they identical? Blood product identification Check the pack number on the Blood Transfusion Record, pack tag/label and the product. Are they identical?

76
Blood administration Pretransfusion check - 3 Blood Group
Check the blood group (ABO and RhD) on the Blood Transfusion Record (this form reports compatibility), pack tag/label and the product. Do they match? Check expiry date on the pack Check medical orders product type, special requirements (eg irradiation, leucocyte depletion) administration requirements (eg volume, rate) Complete documentation sign, date, time the Blood Transfusion Record file in the patient's medical record
 on the Blood Transfusion Record (this form reports compatibility), pack tag/label and the product. Do they match Check expiry date on the pack. Check medical orders. product type, special requirements (eg irradiation, leucocyte depletion) administration requirements (eg volume, rate) Complete documentation. sign, date, time the Blood Transfusion Record. file in the patient s medical record.")
77
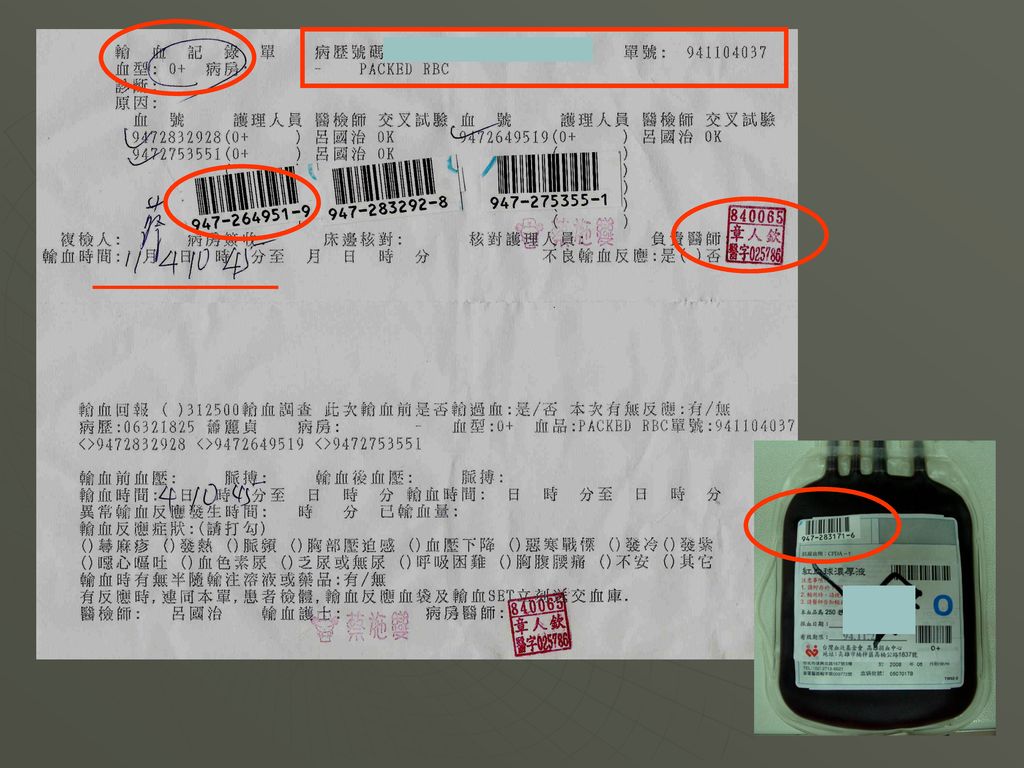
Blood administration Blood Transfusion Record
The Blood Transfusion Record is a legal document and must be filed in the patient medical record at the completion of transfusion. The record must be available for at least 20 years.

78
Blood administration Transfusion Tag
The Blood Transfusion Record is a legal document and must be filed in the patient medical record at the completion of transfusion. The record must be available for at least 20 years.

80
Blood administration Care and monitoring
temperature, pulse, respiratory rate and blood pressure should be measured and recorded: before the start of each pack of blood or blood product at 15 minutes after commencement hourly during transfusion at the completion of each pack may require more frequent observations particularly in unstable or unconscious patients

81
Blood administration Care and monitoring
more frequent vital signs should be taken if the patient has an unstable underlying condition or the patient becomes unwell or shows signs of a transfusion reaction Patients should be observed during the first 15 minutes of transfusion as some life-threatening reactions may occur after the infusion of only a small amount of blood. Where possible, patients should be informed of possible symptoms of a transfusion reaction and should inform staff immediately if they feel unwell during transfusion.

82
General Transfusion Practices

83
How to manage blood transfusion?
Pretransfusion-IV route and sampling Manage Blood transfusion

84
謝謝聆聽 !! 捐血快樂 用血安全

Similar presentations

家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")

 病理生理学系 Department of Pathophysiology 高远生.>")







: Free Response idea: 你周末做了什么?>")


是一种病死率极高的严重传染病—世纪温疫和超级癌症,目前还没有治愈的药物和方法,也没有疫苗预防。>")



>")
