Download presentation
1
Perspectives & New developments in Postmenopausal HRT
台中榮總婦產部 楊曉君醫師

2
Symptoms and signs of the climacteric
Vasomotor symptoms psychosocial symptoms of perimenopausal women Menopausal symptoms The impact of menopause on urethra and vagina Sexual response: sexual appetite,arousal,orgasm

3
血管舒縮症狀 熱潮紅、盜汗、 失眠 疲倦、頭痛 情緒不穩

4
Psychosocial symptoms of perimenopausal women
Decreased energy and drive Irritability Nervous exhaustion Mood fluctuations Tension Depression Anxiety Headache Insomnia Decrease libido.

5
停經及雌激素缺乏時身體的問題
6
更年期初期症狀《1》 熱潮紅、盜汗、失眠、心悸 陰道萎縮、乾澀、性交疼痛 陰道感染增加 尿道萎縮、頻尿、尿失禁 尿道感染增加

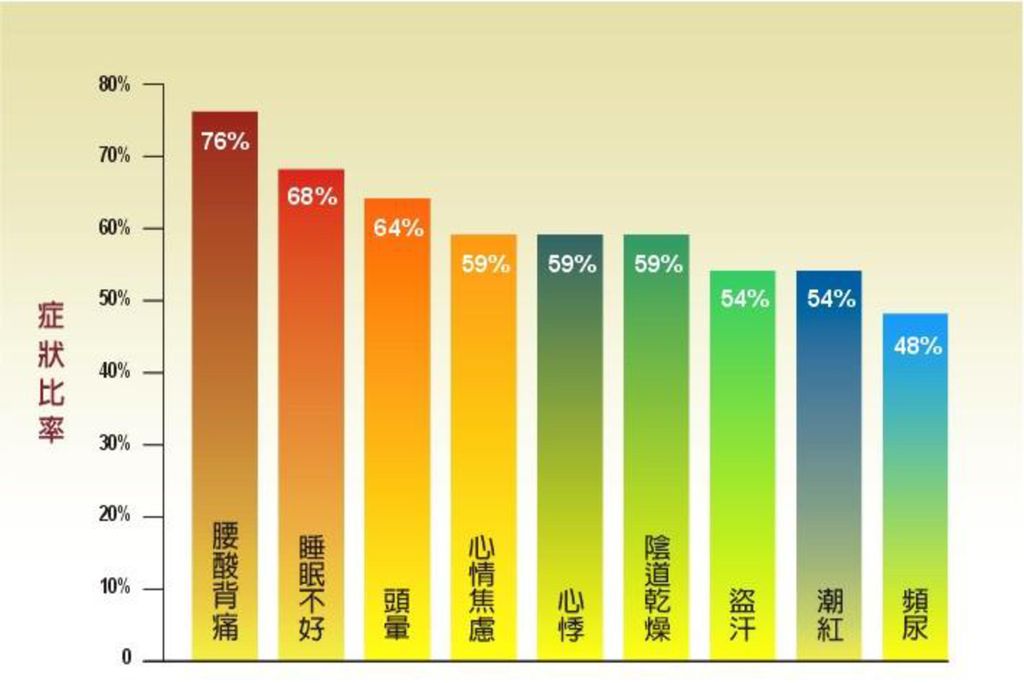
7
更年期初期症狀《2》 腰酸背痛、骨骼疼痛 疲倦感、失眠 情緒不穩、容易憂鬱 皮膚乾燥、老化、皺紋增加 乳房萎縮

9
婦女有更年期症狀的平均年數 1- 5年 56% 5年以上 26% 沒有症狀或有 症狀但不超過一年 18%
參考資料:Mckinlay and Jetterys Br J. Prov 800 Med 1974:28:

10
生殖道的變化 因為陰道上皮萎縮及黏膜萎 縮後容易創傷,性交時會疼 痛,也容易感染,導致陰道 發炎,白帶分泌 增加等等。

11
萎縮的陰道上皮細胞 雌激素缺乏:萎縮 正常

12
泌尿道的變化 因為泌尿道上皮萎縮,較容易 引起頻尿、尿失禁 尿道炎、膀胱炎等。

13
更年期晚期問題 骨骼系統 骨質流失、骨質疏鬆症。 脊椎骨、腕骨、髖部等處的骨折 危險性增加。 中樞神經系統 記憶力減退。 老年癡呆症。

14
更年期晚期問題-骨質疏鬆症 雌激素的缺乏導致骨質流失 骨質流失在停經後的頭幾年 平均每年流失 2 - 5%

15
荷爾蒙療法(HT) 更年期婦女,因為卵巢功能萎縮, 荷爾蒙分泌逐漸減少,導致身體出現一些症狀,須由外界供給才能維持身體需要的血中荷爾蒙濃度,這種療法稱之為「荷爾蒙療法」
 更年期婦女,因為卵巢功能萎縮, 荷爾蒙分泌逐漸減少,導致身體出現一些症狀,須由外界供給才能維持身體需要的血中荷爾蒙濃度,這種療法稱之為「荷爾蒙療法」")
16
「荷爾蒙療法」的意義 治療性-迅速減輕甚至完全緩解更年期症狀如: 預防性-預防骨質疏鬆症。 減少老年癡呆症的發生? 熱潮紅、盜汗、失眠、心悸
陰道乾澀、泌尿道萎縮、性交疼痛 預防性-預防骨質疏鬆症。 減少老年癡呆症的發生?

17
荷爾蒙療法的不適應症狀 子宮點狀或不規則出血 乳房脹痛 暫時性噁心 少許水腫

18
子宮出血 荷爾蒙療法,只要子宮還在,就有出血的可能。
持續性療法者,在使用初期可能會有3-6個月點 狀或不規則出血,但會隨使用時間延長而獲得改善。 週期性療法者,可產生類似月經的規則性出血。

19
Managing bleeding during postmenopausal HRT(I)
Options for persistent bleeding Sequential therapy Vaginal hysterectomy Endometrial ablation The progestin IUD Indications for pretreatment biopsy Characterstics associated with high risk of pathology Preious unposed estrogen therapy

20
Managing bleeding during postmenopausal HRT(II)
Indications for endometril biopsy during treatment Treatment with unopposed estrogen Past history of unopposed estrogen therapy Endometrial thickness greater than 4 mm Clinical anxiety Patient anxity

21
荷爾蒙療法之演進 1940 年代 Dr. Robert Wilson “雌激素缺乏使女性老化”‚ 補充雌激素可解決此問題。
了解雌激素在女性化過程扮演重要角色。 對更年期婦女的症狀有明顯改善作用。 醫療界使用雌激素改善婦女更年期症狀。

22
荷爾蒙療法之演進 1970 年代 發現單獨使用雌激素會使子宮內膜癌增加 2~11 倍。 雌激素使用明顯減少。 1980年代
證明只要在雌激素治療中加上黃體素‚ 便可減少罹患子宮內膜癌機率‚ 甚至降低發生率。 證明荷爾蒙療法可增加骨質密度‚ 預防骨質疏鬆症。

23
荷爾蒙療法之演進 1990 年代 陸續證明荷爾蒙療法可降低膽固醇‚ 對心血管疾病有利。
陸續證明荷爾蒙療法對失智症、大腸直腸癌、 落齒…等皆有利。 長期使用(五年以上)可能使乳癌機率增加。 認為荷爾蒙療法利大於弊‚ 百利僅有一害。 1998年 HERS Study 發現荷爾蒙對已有中度至重度心臟病婦女無預防效果。
可能使乳癌機率增加。 認為荷爾蒙療法利大於弊‚ 百利僅有一害。 1998年. HERS Study 發現荷爾蒙對已有中度至重度心臟病婦女無預防效果。")
24
荷爾蒙療法之演進 2002 年七月 美國 WHI Study發現 : 使用荷爾蒙 5.2 年‚ 會使乳癌、心血管疾病、中風增加; 對骨折、 大腸直腸癌有預防效果。認為長期使用弊大於利。 荷爾蒙療法依個人需求‚ 評估利與弊‚ 用於緩解更年期症狀、萎縮性陰道炎與尿道炎、 及預防骨質疏鬆症‚ 並作密切檢查追蹤。

25
Major osteoporosis risk factors
Oophorectomy Early menopause Low body weight Positive family history Calcium deficiency Cigarette smoking Extreme immobility Excessive use of alcohol Estrogen deficiency Prolonged/High dose corticosteroid therapy

26
骨質疏鬆症的危險因子 雌激素缺乏 缺乏運動 本人曾發生骨折 鈣質攝取不足 日曬不足 體型瘦小 長期使用類固醇藥物 家族老人曾發生骨折
抽煙酗酒

27
骨鬆性骨折好發部位

28
骨鬆性骨折好發部位 脊椎骨骨折圖 骨質密度比較 正常骨質 被壓垮的脊椎骨 骨折 骨質疏鬆 髖部骨折圖 股骨頸骨折 正常髖關節 大小轉子間骨折

29
HRT & osteoporosis Prophylactic use of HRT to prevent fracture had been documented by case-control and observational cohort studies Hip fracture are reduced by 40-60% Suggest that at least 6 years of treatment to achieve a significant reduction in fracture, benefit diminishes markedly within several years after discontinuting HRT WHI study :Randomized, placebo-controlled clinical trials: demonstrated a significant reduction in fracture FDA : prevent osteoporosis

30
荷爾蒙療法能預防骨質的流失,愈早補充效果愈好
參考資料:Christiansen C et al. Lancet 1981:1:459

31
使用雌激素在不同時期對 預防骨質流失的效果
參考資料:Lindsay R., Clin Obstet Gynecol 1987;30:847

32
補充雌激素加鈣比單獨補充鈣效果更好 參考資料:Lindsay R. et al. Obstet Gynecol 1990,76(2):290
:290")
33
停經後婦女髖部骨折的發生率 參考資料:Weiss N. et al., N Engl J Med 1980;303:1195.

34
運 動 適度並持之以恆的運動,可 以刺激維持骨骼中的鈣,緩 和骨質疏鬆的發生, 同時 可以增加肌肉彈性。

35
Estrogen and cardiovascular system possible beneficial actions of estrogen on CV
A favorable impact on the circulating lipid,decrease in total cholesterol and LDL-cholesterol and increase in HDL-cholesterol Direct antiatherosclerotic effect in arteries Augmentation of vasodilating and antiplatelet aggregation factors Vasodilation by means of endothelium-independent mechanisms Inhibition of macrophage foam cell formation Direct inotropic actions on the heart and large blood vessels Protection of endothelial cell from injury. Improvement of peripheral glucose metabolism with a subsequent decrease in circulating insulin levels

36
HT and cardiovascular disease(I)
A large body of observational clinical studies repeatedly demonstrated favorable associations between postmenopausal HRT and cardiovascular morbidity, mortality, and risk factors.

37
The Heart and Estrogen/progestin Replacement study(HERS)
HT and cardiovascular disease(II) The Heart and Estrogen/progestin Replacement study(HERS) A randomized,double-blind, placebo-controlled clinical trial; 2763 women(average age 66.7) with pre-existing coronar disease in 20 centers randomized to treatment with premarine 0.626mg+ provera 2.5mg or placebo 172 MI & coronary deaths in HRT group and 176 in placebo group No effect for decrease MI, but still safe for patient with cardiovascular disease
 The Heart and Estrogen/progestin Replacement study(HERS) A randomized,double-blind, placebo-controlled clinical trial; women(average age 66.7) with pre-existing coronar disease in 20 centers randomized to treatment with premarine 0.626mg+ provera 2.5mg or placebo. 172 MI & coronary deaths in HRT group and 176 in placebo group. No effect for decrease MI, but still safe for patient with cardiovascular disease.")
38
Advice to menopausal women in view of HERS
Healthy women HERS has no bearing on primary prevention Consideration of HRT is beneficial Women with established CAD currently taking HRT Continue therapy Support the benefit of long-time HRT as secondary prevention Women with established CAD not taking HRT Individualize the use of HRT according to patient profile

39
Peri- and postmenopausal unopposed estrogen therapy and risk of endometrial cancer
Difinite increase risk of endometrial cancer Relactive risk varies from 2 to 12 . Risk persist after discontinuation Opposed HRT regimens

40
Cell proliferative and carcinogenesis
Breast cancer estrogen-progestin hypothesis Endometrial cancer unopposed estrogen hypothesis Ovarian cancer -- incessant ovulation hypothesis --gonadotrophin hypothesis

41
Hormonal aspects of epithelial ovarian cancer: epidemillogical evidence ( I )
menstration early menarche and late natural menopause increase the risk of cancer “incessant ovulation” hypothesis parity and pregnancy pregnancy leads to anovulation and suppresses pituitary GN protective effect of increasing parity is established (Nationwide chhort case-control study in Sweden per pregnancy) full-term pregnancies -- protective effect incomplete pregnancies and abortion--conflicting results
 full-term pregnancies -- protective effect. incomplete pregnancies and abortion--conflicting results.")
42
Hormonal aspects of epithelial ovarian cancer:
epidemiological evidence ( I I ) lactation lactation suppresses the secretion of pituitary GN and lead to anovulation --most studies have found a decreased risk but little study with conflicting results Progestin only contraceptives prevents pregnancy through alterations of the cervical mucus and endometrium ,ovulatory cycles usually continuous. --study is limited
 lactation. lactation suppresses the secretion of pituitary GN and lead to anovulation. --most studies have found a decreased risk but little study with conflicting results. Progestin only contraceptives. prevents pregnancy through alterations of the cervical mucus and endometrium ,ovulatory cycles usually continuous. --study is limited.")
43
Hormonal aspects of epithelial ovarian cancer:
epidemillogical evidence ( III ) Combined oral contraceptives protect effect from suppressed mid-cycle gonadotrophin surge and inhibited ovulation --most studies with protection in 1960s with fixed and high estrogen and progestin doses. --low dose OC (equal or less than 35ug of ethinyl oestradiol) decreased the RR to 0.7 to 0.4 respectively. --ever users of OC: 30% protection , more than 5 years OC decline risk 50% . Protection persists at least 10 years after cessation of use.
 Combined oral contraceptives. protect effect from suppressed mid-cycle gonadotrophin surge and inhibited ovulation. --most studies with protection in 1960s with fixed and high estrogen and progestin doses. --low dose OC (equal or less than 35ug of ethinyl oestradiol) decreased the RR to 0.7 to 0.4 respectively. --ever users of OC: 30% protection , more than 5 years OC decline risk 50% . Protection persists at least 10 years after cessation of use.")
44
Hormonal aspects of epithelial ovarian cancer:
epidemillogical evidence ( IV ) Hormone replacement therapy HT decrease the secretion of pituitary gonadotrophins, according to “gonadotrophin” hypothesis a reduced risk is expected. --most study show no association.one study show significant increase risk with relactive risk 1.71 after 11 years usage,but the finding is disputed in other study
 Hormone replacement therapy. HT decrease the secretion of pituitary gonadotrophins, according to gonadotrophin hypothesis a reduced risk is expected. --most study show no association.one study show significant increase risk with relactive risk 1.71 after 11 years usage,but the finding is disputed in other study.")
45
Hormonal aspects of epithelial ovarian cancer:
epidemiological evidence ( V ) Tubal ligation and hysterectomy the cause of protective effect remains unclear detection bias : these procedure was performed at parous women and if ovaries that appear abnormal at surgery are removed. procedure decrease ovarian blood flow=> decrease ovarian hormone production decrease ovulation elevated gonodotropin Interrupted retrograde transport of contaminants or carcinogens through the Fallopian tube.
 Tubal ligation and hysterectomy. the cause of protective effect remains unclear. detection bias : these procedure was performed at parous women and if ovaries that appear abnormal at surgery are removed. procedure decrease ovarian blood flow=> decrease ovarian hormone production --decrease ovulation --elevated gonodotropin. Interrupted retrograde transport of contaminants or carcinogens through the Fallopian tube.")
46
Hormonal aspects of epithelial ovarian cancer:
epidemiological evidence ( VI ) Infertility and ovulation induction nulliparity is an established risk factor, When focus on infertility as a separate effect: --temporary fertility problems in parous women do not raise risk --the association between fertility drugs and epithelial oarian cancer risk is not necessarily causal, but causality cannot be excluded. --women who stayed nulliparous after the use of fertility drugs had a much high risk than women who became parous.
 Infertility and ovulation induction. nulliparity is an established risk factor, When focus on infertility as a separate effect: --temporary fertility problems in parous women do not raise risk. --the association between fertility drugs and epithelial oarian cancer risk is not necessarily causal, but causality cannot be excluded. --women who stayed nulliparous after the use of fertility drugs had a much high risk than women who became parous.")
47
HT & Ovarian ancer 12 case-control studies of of ovarian cancer risk factor, pooled analysis the literature, no consistent evidenc between HRT and ovarian cancer Meta-analysis study: ever users increase 14% risk HRT > 10 years, increase 27% risk Among 6 studies analysis duration and risk: only one report a statistically increase risk when HRT >10 years (HRT & Ovarian cancer, Am J Epidemio 141:828,1995)
")
48
荷爾蒙療法與乳癌

49
民國八十六年女性癌症年齡別發生率 每十萬婦女人口發生率 資料來源:衛生署統計報告

50
HRT & Breast cancer (A Re-analysis of the world’s literature –51 studies,meta-analysis)
51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer,Lancet 350:1049,1997 Ever users of HRT overall increase relative risk of 1.14 Current users>5 yrs,relative risk of 1.35, increase duration => increase risk. Current and recent users had evidence of having only localized disease, ever users had less metastatic disease The was no effect of a family history of breast cancer There was no increase risk in past users The increase in relative risk in current and recent users was greatest in lower body weight women.

51
HRT & Breast cancer All epidemiologic studies, short-term users=> no increase risk many observational studies have failed to develop evidence that long-term users increase risk of breast cancer Long-term of current users is associated with a slight inrease in risk, a risk is less than that associated with obsity or daily alcohol consumption. During HRT user develop breast cancer=>reduced risk of dying from breast cancer Increase surveillance and early detection Acceleration of pre-existing tumor growth =>tumor apper at less aggressive stage

52
乳癌的危險因子 資料來源:New England Journal of Medicine , 2001 , 344:

54
WHI Study (1) ( Women’s Health Initiative )
目的: 評估混合型荷爾蒙補充療法的 主要效益與危險性. 主要評估: 1. 冠狀動脈心臟病的預防,及侵入性乳癌的 發生率. 2. 中風,肺栓塞,子宮內膜癌,大腸直腸癌, 髖部骨折的發生率及其他原因之致死率.

55
WHI Study (2) ( Women’s Health Initiative )
婦女健康關懷研究:雌激素合併黃體素療法的相對及絕對風險或效益 (n = 16,608,對照組與研究用藥) 病症 5.2年後與對照組比較 每年每萬名婦女中 每年每萬名婦女中 相對風險 所增加的絕對風險 所增加的絕對效益 心臟病 中風 乳癌 血栓 直腸癌 髖部骨折 *資料來源:JAMA, July 17, 2002, 288:
 病症 5.2年後與對照組比較 每年每萬名婦女中 每年每萬名婦女中. 相對風險 所增加的絕對風險 所增加的絕對效益. 心臟病 中風 乳癌 血栓 直腸癌 髖部骨折 *資料來源:JAMA, July 17, 2002, 288:")
56
WHI Study (3) ( Women’s Health Initiative )
結論: 1. 為期平均 5.2 年的研究中, 總危險性超 過效益. 2. 所有原因造成的死亡率並無增加. 3. 此混合型荷爾蒙補充療法不該用於冠心臟病的預防.

57
細讀 WHI Study (1) 373,092 位婦女參與篩選. 18,845 婦女同意加入且無子宮切除. 16,608 位婦女隨機分配.
8,506 位婦女接受混合型荷爾蒙補充療法. 8,102位婦女接受安慰劑.

58
細讀 WHI Study (2) 雌激素加黃體素 安慰劑 亞太婦女 194人 (2.3%) 160人 (2.1%)
雌激素加黃體素 安慰劑 亞太婦女 人 (2.3%) 160人 (2.1%) 參加研究前使用荷爾蒙時間 (年) < 5 年 % % 5 – 10 年 % % > 10 年 % % 女性親屬曾罹患乳癌 1268人 (16.0%) 1175人 (15.3%)
 160人 (2.1%) 參加研究前使用荷爾蒙時間 (年) < 5 年 69.1% 70.6% 5 – 10 年 19.1% 17.2% > 10 年 11.8% 12.2% 女性親屬曾罹患乳癌. 1268人 (16.0%) 1175人 (15.3%)")
59
細讀 WHI Study (3) 膽固醇變化: 低密度膽固醇(LDL) -12.7 % 高密度膽固醇 (HDL) +7.3 %
三酸甘油脂(TG) %
 +6.9 %")
60
WHI Study之缺陷 (1) 平均年齡較高 (平均 63.3 歲). 只測試一種藥品. 並無評估更年期症狀與陰道萎縮的效益.
無法區分其結果為雌激素或黃體素的作用.

61
WHI Study之缺陷 (2) 治療組停藥比率高達42%, 另有 10.7%安慰劑組婦女停止服用安慰劑改用HRT.
研究太早停止,減少對長期效益評估的準確性.

62
Women’s Health Initiative
資料來源:JAMA, 2002, 288:

63
WHI 總結 WHI 研究之美國的研究, 其人種與生活習慣與我國不盡相同, 不一定能完全引用於國人.
此單項研究結過未必足以推翻以前的研究結果而說荷爾蒙療法一定有問題. WHI 研究有 Risk - Breast Cancer, CVD. WHI研究有 Benefit - Hip Fracture, Colorectal Cancer. WHI 未將更年期症狀與萎縮性陰道炎/尿道炎列入效益評估. HRT 是緩解更年期症狀與萎縮性陰道炎/尿道炎與預防骨質疏鬆症最有效的方法, 應列入效益評估, 再作成結論. HRT短期使用( < 4 年)利大於弊. HRT使用四年以上需請醫師評估症狀需求, 骨質狀態與相關危險因子後再做決定, 並做定期檢查.
利大於弊. HRT使用四年以上需請醫師評估症狀需求, 骨質狀態與相關危險因子後再做決定, 並做定期檢查.")
64
WHI 總結 婦女應在醫師處方下服用荷爾蒙,由婦產科醫師評估處方才能保障用藥安全。 此研究提醒醫師未來使用荷爾蒙補充療法時需更加謹慎。
研究負責人強調,這種危險相當小,婦女無須驚慌,還建議其他婦友不要隨意停藥,宜請教醫師。

65
我們應該如何給婦女建議 使用荷爾蒙補充療法的主要適應症為治療更年期症候群使用期間越短越好,使用劑量越低越好。
荷爾蒙補充療法不應用於(初級或次級)預防心臟血管疾病 雖然美國食品藥物管理局核可荷爾蒙補充療法用於預防骨鬆症,且 WHI 也證實荷爾蒙補充療法可減少骨鬆引起的骨折。但荷爾蒙補充療法可能增加心臟血管疾病與乳癌,要用於預防骨鬆症應小心的做個別考量.要預防骨鬆症,美國預防醫學小組與美國婦產科醫學會不建議用荷爾蒙補充療法,可考慮其他方式來預防。在國內,荷爾蒙補充療法為健保局有幾付的唯一 ( 預防 ) 骨鬆症之藥物,其他藥物則只有在已發生骨鬆症骨折後才有給付使用.未有骨折的婦女,如要使用其他藥物預防骨鬆症,必須自費。
預防心臟血管疾病. 雖然美國食品藥物管理局核可荷爾蒙補充療法用於預防骨鬆症,且 WHI 也證實荷爾蒙補充療法可減少骨鬆引起的骨折。但荷爾蒙補充療法可能增加心臟血管疾病與乳癌,要用於預防骨鬆症應小心的做個別考量.要預防骨鬆症,美國預防醫學小組與美國婦產科醫學會不建議用荷爾蒙補充療法,可考慮其他方式來預防。在國內,荷爾蒙補充療法為健保局有幾付的唯一 ( 預防 ) 骨鬆症之藥物,其他藥物則只有在已發生骨鬆症骨折後才有給付使用.未有骨折的婦女,如要使用其他藥物預防骨鬆症,必須自費。")
66
我們應該如何給婦女建議 少數可考慮長期使用荷爾蒙補充療法的症狀如下: 已切除子宮 , 單獨使用雌激素的婦女可繼續使用荷爾蒙補充療法 .
(一)更年期症狀嚴重的婦女,經說明利弊後,仍覺得荷爾蒙補充療法對她來說好處多餘壞處者。 (二)有更年期症狀且有骨鬆症之風險之婦女。 (三)有骨鬆症之風險而又無法接受其他骨鬆症治療方式婦女。
更年期症狀嚴重的婦女,經說明利弊後,仍覺得荷爾蒙補充療法對她來說好處多餘壞處者。 (二)有更年期症狀且有骨鬆症之風險之婦女。 (三)有骨鬆症之風險而又無法接受其他骨鬆症治療方式婦女。")
67
我們應該如何給婦女建議 荷爾蒙補充療法有利有弊,每個婦女的需求(是否有更年期症狀),期望與危險因子(是否有心臟病、乳癌、靜脈栓塞、大腸直腸癌、骨鬆症的危險因子)都不同。需要作個別的考量,無一體適用的答案。停經婦女應與醫師商量,了解荷爾蒙補充療法對她的利弊後,再決定是否要使用。 使用荷爾蒙補充療法的婦女應於一段時間後(不超過半年)再做整體評估。看是否需要改變治療方式,針對停經婦女的需求。醫師也應與她討論荷爾蒙之外的其他處置方式。
再做整體評估。看是否需要改變治療方式,針對停經婦女的需求。醫師也應與她討論荷爾蒙之外的其他處置方式。")
68
Raloxifene safety summary: A selective estrogen receptor modulator (SERMs)
Antagonistic to estrogen receptor in myometrium and endometrim=> not associated with endometrial proliferative or vaginal bleeding Antagonistic to estrogen receptor of duct or alveoli of breast => reduces risk of breast cancer Is safe on cognitive and neuropsychomotor function Increase risk for hot fushes and leg cramps Increase risk of VTE, comparable to HRT

70
Thank you for your attention







 全球共同 聲明: 1. MHT( 即 HRT) 是與停經有關的血管收縮性神 經症狀的最有效的治療,但其好處在 60 歲後 或已停經超過.>")

 复旦大学附属妇产科医院 朱 瑾.>")
家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")
 分泌 逐漸減少,月經週期變得不規則,終至完 全停止,並且一年內不再有月經,稱做停 經。 更年期:婦女停經的前後一段日子, 也就 是婦女由具有生育能力進入到不能生育的 過渡時期稱為「更年期」>")





>")
 河南中医学院第一附属医院 杜正光>")




