Download presentation
Presentation is loading. Please wait.

1
Chapter 8. Excretion of kidney
第八章 肾脏的排泄 中山大学基础医学院生理学教研室 王庭槐 Department of physiology of SUMS Wang Tinghuai

2
The Latest information from WHO the incidence rate of urinary system(%)
0.1 0.3 慢性肾功能不全(chronic renal) 0.2 糖尿病肾病(diabetic nephropathy) < 0.1 结核(tubercle) 0.4 多囊肾(polycystic kidney) 肿瘤(Tumor) 2.0 1.3 结石(Calculus0 2.9 8.6 肾炎(nephritis) 9.6 泌尿系感染(Infectious disease) 7.8 19.7 泌尿系统疾病(Disease of urinary system) Developed country Developing country
 0.2. 糖尿病肾病(diabetic nephropathy) < 0.1. 结核(tubercle) 0.4. 多囊肾(polycystic kidney) 肿瘤(Tumor) 结石(Calculus 肾炎(nephritis) 9.6. 泌尿系感染(Infectious disease) 泌尿系统疾病(Disease of urinary system) Developed country. Developing country.")
3
发展中国家泌尿系统疾病发病率高,主要是高发的泌尿系感染、急性肾炎、间质性肾炎、结核等,其主要原因包括:
评价: (evaluation) 发展中国家泌尿系统疾病发病率高,主要是高发的泌尿系感染、急性肾炎、间质性肾炎、结核等,其主要原因包括: The incidence rate of urinary system is high in developing country,especially infectious diseases、acute nephritis, interstitial nephritis,tubercle,etc.the main causes are as follows: 1. 感染性疾病未得到足够控制,导致泌尿系感染、急性肾炎、间质性肾炎和结核的发病率高。 Infectious diseases are not be controlled enough,so the incidence rate of infectious diseases、acute nephritis、 interstitial nephritis、tubercle is high.
 发展中国家泌尿系统疾病发病率高,主要是高发的泌尿系感染、急性肾炎、间质性肾炎、结核等,其主要原因包括: The incidence rate of urinary system is high in developing country,especially infectious diseases、acute nephritis, interstitial nephritis,tubercle,etc.the main causes are as follows: 1. 感染性疾病未得到足够控制,导致泌尿系感染、急性肾炎、间质性肾炎和结核的发病率高。 Infectious diseases are not be controlled enough,so the incidence rate of infectious diseases、acute nephritis、 interstitial nephritis、tubercle is high.")
4
2. 严重的环境污染和生活毒素未得到控制,导致肾小球和肾间质炎症的发病率高,也与高发的肾肿瘤有关。
Heavy environment pollution and toxin are not be controlled enough. 3. 对遗传性疾病缺乏生育控制,与多囊肾等先天性疾病的多发有关。 Birth control are not carried out effectively for preventing genetic disease.So the incidence rate of congenital diseases such as polycystic kidney is high.

5
4. 社会医疗服务经费的缺乏,使得较多患者的疾病发展到慢性肾功能衰竭。
The deficiency of social funds for medicine service leads to many diseases developing into chronic renal failure. 5. 透析和移植治疗的缺乏,使得慢性肾功能衰竭不能得到纠正,引起更多的感染和肿瘤发生。 Chronic renal failure isn’t be corrected because of the deficiency of dialyse and transplantation , so more infectious diseases and tumors occur.

6
概述(Introduction) 排泄(excretion)——机体将物质代谢尾产 物和机体不需或过剩的物质排出体外的 过程
the process that the cellular waste products or extra nutrients、minerals and water leaving the body.

7
排泄的四个途径:(Four excretory pathways)
由呼吸器官排出(By respiratory organ) 由大肠排出(By intestinal tract) 由皮肤排出(By skin) 由肾脏排出(By kidney)
 由大肠排出(By intestinal tract) 由皮肤排出(By skin) 由肾脏排出(By kidney)")
8
排泄的功能意义 The functional significance of excretion:
排除代谢尾产物、异物 Elimination of waste products and foreign material 排除过剩的电解质、H+ 维持酸碱平衡 Elimination of extra electrolure、 H+ so to maintain acid-based balance.

9
调节细胞外液量和血液的渗透压 Regulation of extracellular fluid and osmotic pressur in blood. 保留体液中某些重要成份:如Na+、K+、HCO3-、Cl - Reservation of important materials in body fluid such as Na+、K+、HCO3- and Cl -

10
泌尿功能和非泌尿功能 The renal function:
泌尿功能——尿生成过程 1.肾小球的滤过(glomeruluar filtration) 2.肾小管和集合管的重吸收(reabsorption in renal tubule and collect tubule) 3.肾小管与集合管的排泄(excretion of tubule and collect tubule)
 2.肾小管和集合管的重吸收(reabsorption in renal tubule and collect tubule) 3.肾小管与集合管的排泄(excretion of tubule and collect tubule)")
11
非泌尿功能——分泌生物活性物质 肾分泌的活性物质: A.促红细胞生成素(erythropoietin,EPO)—促RBC生成 B. 肾素(renin)——①调节醛固酮(aldosterone)分泌②调节血量③调节电解质浓度 C. 羟化VitD3——钙磷代谢 D. PGA——舒血管

12
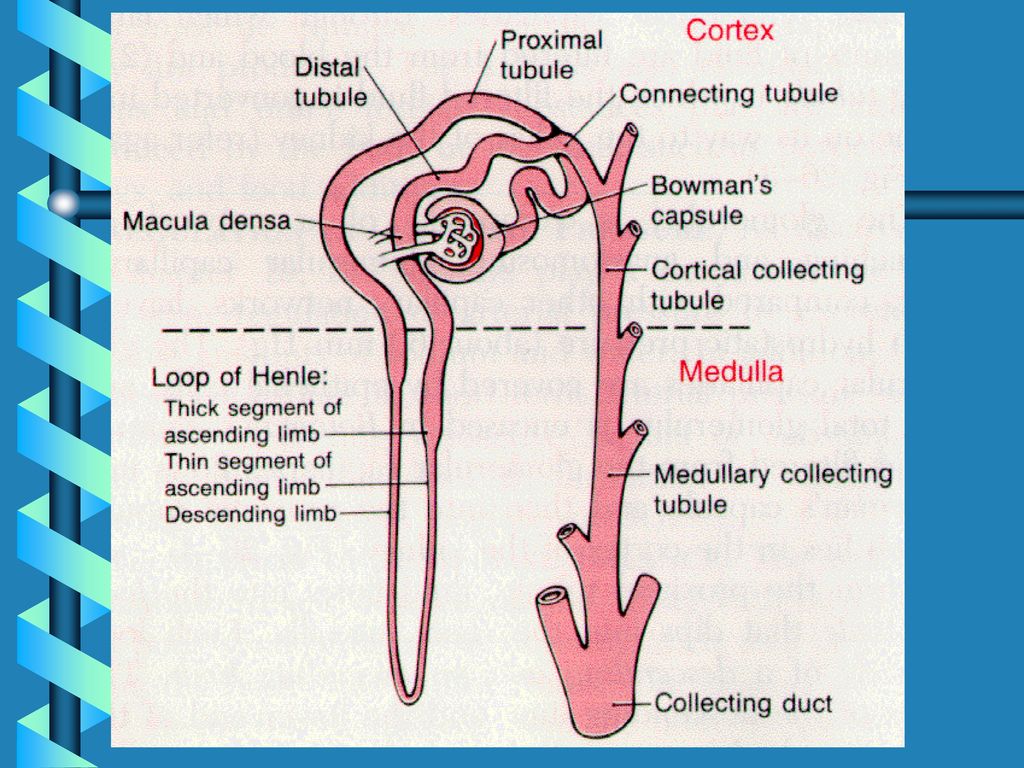
第一节 肾脏的结构与功能特点 肾小球glomerulus(毛细血管球) 一、 肾小体
一、 肾小体 renal corpuscle 肾小囊renal capsule (内层、囊腔、外层) 肾单位 (Nephron) 近球小管proximal tubule 200万个 肾小管 髓袢medullary loop renal tubule 远球小管distal tubule
 肾单位. (Nephron) 近球小管proximal tubule. 200万个. 肾小管 髓袢medullary loop. renal tubule. 远球小管distal tubule.")
14
集合管(Collecting tubule):不包括在肾单位内,在尿液浓缩功能中起作用。
:不包括在肾单位内,在尿液浓缩功能中起作用。")
15
肾单位 ( cortical nephron) 入小球小A口径 >出球 类型
皮质肾单位:占85~90%,肾小球小, 肾单位 ( cortical nephron) 入小球小A口径 >出球 小A 类型 近髓肾单位(juxtamedullary nephron): 占10~15%,肾小球大,入球小A口 径≈出球小A,位于皮质深部1/3处, 出球小A 网状小血管 直小血管U形
 入小球小A口径 >出球. 小A. 类型. 近髓肾单位(juxtamedullary nephron): 占10~15%,肾小球大,入球小A口. 径≈出球小A,位于皮质深部1/3处, 出球小A 网状小血管. 直小血管U形.")
16
二、近球小体(juxtaglomerular apparatus)
入球小A(afferent arteriole)的近球细胞(颗粒细胞 juxtaglomerular cells)——分泌肾素(renin) 系膜细胞(间质细胞 ) 远曲小管的致密斑(macular densa)——感受小管内Na+含量的变化——近球细胞——调节肾素(renin)分泌
的近球细胞(颗粒细胞 juxtaglomerular cells)——分泌肾素(renin) 系膜细胞(间质细胞 ) 远曲小管的致密斑(macular densa)——感受小管内Na+含量的变化——近球细胞——调节肾素(renin)分泌.")
18
三、肾脏血液循环的特点 (一)肾脏的血液供应 (renal blood supply) 1.血供丰富 成人安静时1200ml /min
皮质(cortex) 94% 外髓(outer zone) 5~6% 内髓(inner zone) 1%
 94% 外髓(outer zone) 5~6% 内髓(inner zone) 1%")
19
2.两套毛细血管网 肾A(renal artery)——叶间A(interlobar arteries)——弓形A(arcuate arteries)——小叶间A(interlobular arteries)——入球小A(afferent arterioles)——毛细血管网(golmerular capillaries)——出球小A(efferent arterioles)——毛细血管(peritubular capillaries)—— 小叶间V(interlobular vein)——弓形V(arcuate vein)——叶间V(interlobar vein)——肾静脉(renal vein)
——叶间A(interlobar arteries)——弓形A(arcuate arteries)——小叶间A(interlobular arteries)——入球小A(afferent arterioles)——毛细血管网(golmerular capillaries)——出球小A(efferent arterioles)——毛细血管(peritubular capillaries)—— 小叶间V(interlobular vein)——弓形V(arcuate vein)——叶间V(interlobar vein)——肾静脉(renal vein)")
20
-

21
3.肾内血流量分布不均匀 (maldistribution of blood flow in kidney)
皮质血流量>髓质 blood flow in the vasa recta of the renal medulla is very low compared with flow in the renal cortex 皮质肾单位入球小A口径 > 出球小A (阻力小) (阻力大—肾小球内 压高—利于滤过) 髓质血流量少 直小血管阻力大 原因 髓质部高阻力 管内血粘滞也较高
 (阻力大—肾小球内. 压高—利于滤过) 髓质血流量少. 直小血管阻力大. 原因 髓质部高阻力. 管内血粘滞也较高.")
22
(二)肾血流量的调节(regulation of blood flow in kidney) 1.肾血流的 自身调节
Autoregulation 灌注压(perfusion pressure)20~80mmHg(2.7~10.7Kpa)时,肾血流量随肾A 压升高而升高 灌注压80~180mmHg(10.7~24Kpa)时,肾血流量稳定在一个水平不变 灌注压>180mmHg(>24Kpa)时,肾血流量又随肾A压升高而升高
20~80mmHg(2.7~10.7Kpa)时,肾血流量随肾A. 压升高而升高. 灌注压80~180mmHg(10.7~24Kpa)时,肾血流量稳定在一个水平不变. 灌注压>180mmHg(>24Kpa)时,肾血流量又随肾A压升高而升高.")
23
罂粟硷(Papaverine)、水合氯醛(Chloral Hydrate)—抑制血管平滑肌后自身调节(autoregulation)现象消失,提示自身调节与血管平滑肌活动有关。
机制:细胞分流学说、组织压力学说、肌原反应学说、反馈调节学说

24
肌原学说(myogenic mechanism)
stretch of the vascular wall allows increased movement of calcium ions from the extracellular fluid into the cells,causing them to contract.This contraction pervents overdistention of the vessel and at the same time,by raising vascular resistance,helps to prevent excessive increases in renal blood flow when arterial pressure increases. (反之亦然)
")
25
2.肾血流的神经和体液调节(sympathetic nervous system and hormonal or autacoid control of renal circulation)
肾N(发自T12 L2)属交感神经系统,入球小A的N末梢分布密度大——收缩血管效应;肾素分泌。 迷走N纤维对尿生成的影响尚未肯定。 体位性肾血液量改变,可能是反射性交感N兴奋所致 体液因素:肾上腺素(adnephrin)与去甲肾上腺素(norepinephrine)、升压素、血管紧张素(angiotensin)——肾血管收缩(静滴Adr.10微克/分,肾血流量减少30%)
属交感神经系统,入球小A的N末梢分布密度大——收缩血管效应;肾素分泌。 迷走N纤维对尿生成的影响尚未肯定。 体位性肾血液量改变,可能是反射性交感N兴奋所致. 体液因素:肾上腺素(adnephrin)与去甲肾上腺素(norepinephrine)、升压素、血管紧张素(angiotensin)——肾血管收缩(静滴Adr.10微克/分,肾血流量减少30%)")
26
意义(significance) 安静正常:通过自身调节使肾血流量相对稳定,泌尿活动正常进行。
The autoregulation maitains the renal blood flow and activity of excretion at rest. 运动或异常如高温、出血缺氧时:通过神经、体液调节使血流量减少,保证重要器官的血流供应。 During severe,acute disturbances such as hyperthermia and hypoxia it ensures the blood flow of important organs by decreasing the renal blood flow.

27
第二节 尿生成过程(urine formation)
滤过(glomerular filtration) 选择性重吸收(selective reabsorportion) 分泌与排泄(secretion)
 选择性重吸收(selective reabsorportion) 分泌与排泄(secretion)")
28
一、肾小球的滤过作用(glomerular filtration)
1.血浆(plasm)、滤液(filtrate)、尿成份的比较 微穿刺技术 (micropuncture technique) 获取囊内液, 微量化学分析 表明系血浆的 超滤液(ultrafiltrate)
、滤液(filtrate)、尿成份的比较. 微穿刺技术. (micropuncture technique) 获取囊内液, 微量化学分析. 表明系血浆的. 超滤液(ultrafiltrate)")
29
2.肾小球滤过率(glomerular filtration rate): 单位时间内(每分钟)两肾生成的超滤液量。
125ml/min/1.73m2 125×1440(24h)= L/24h GFR=Kf·Puf(Kf:滤过系数, Puf :有效滤过压)
= L/24h. GFR=Kf·Puf(Kf:滤过系数, Puf :有效滤过压)")
30
3.滤过分数(filtration fraction):肾小球滤过率和肾血浆流量的比值
125 / 660×100%=19% ml/min 可见流过肾脏的血浆约1/5由肾小球滤到肾小囊腔中,GFR与FF是衡量肾功能的指标。

31
二、滤过膜及其通透性(the glomerular capillary membrane and its permeability)
肾小球毛细血管内皮细胞 ( Glomerular capillary endothelium) 滤过膜 基膜(basal lamina) Glomerular filtration barrier 肾小囊内层上皮细胞(epithelium)
 滤过膜. 基膜(basal lamina) Glomerular filtration. barrier. 肾小囊内层上皮细胞(epithelium)")
34
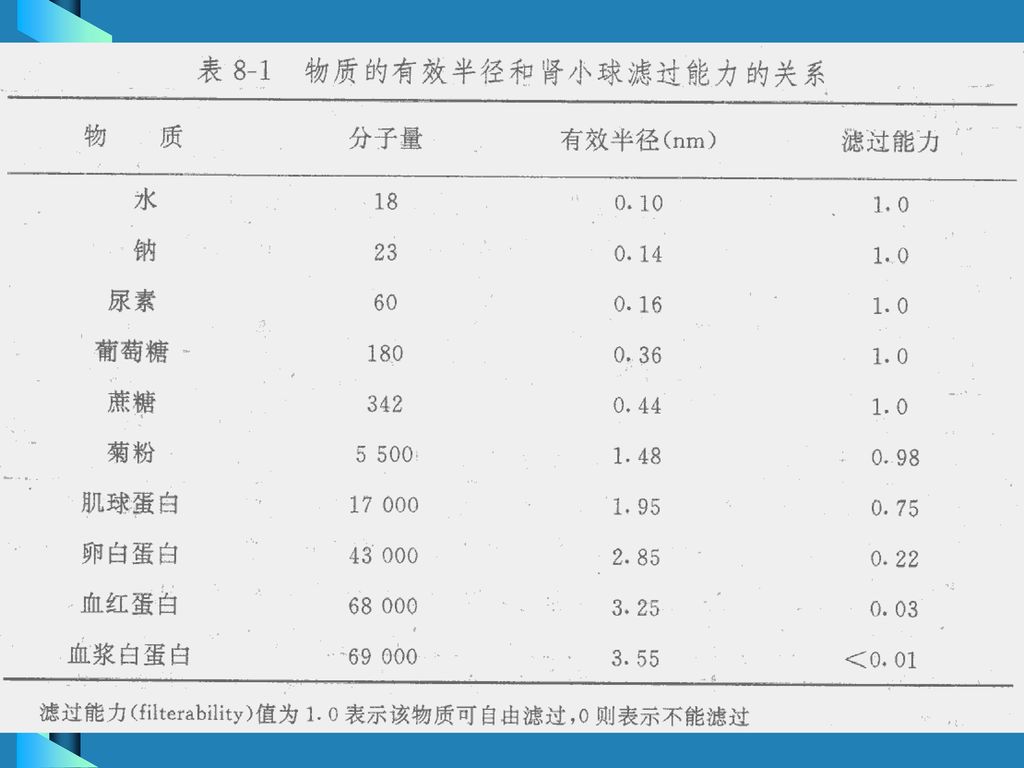
1.分子量大小的选择性滤器(the filtrum of solutes is related to their size)
有效半径<1.8nm可完全通过, >3.6nm不能滤过 葡萄糖glucose(180)可通过, 白蛋白albumin(69000)不能通过
可通过, 白蛋白albumin(69000)不能通过.")
36
2.分子电荷的选择性滤器(the filterability of solutes is related to their electrical charge)
右旋糖酐dextran (+)——易通过滤过膜 右旋糖酐(-) ——难通过滤过膜
——易通过滤过膜. 右旋糖酐(-) ——难通过滤过膜.")
37
上皮和内皮细胞上的酸性糖蛋白,涎基带负电基团和基膜上的硫酸肝素的负离子基团构成了滤过的电学屏障,限制负电荷的滤过。
The negative charges of the basement membrane provide an important means for restricting large negatively charged molecules.

38
电中性分子(neutral moleculars):通透性决定于分子的大小
带负电大分子(moleculars with negative charges):内层细胞层和基膜内侧部的带负电结构可阻止它通过。 带正电大分子(moleculars with positive charges):虽然可能通过内皮细胞层和基膜内侧部,但基膜外侧部和裂孔膜是它的主要屏障。
:内层细胞层和基膜内侧部的带负电结构可阻止它通过。 带正电大分子(moleculars with positive charges):虽然可能通过内皮细胞层和基膜内侧部,但基膜外侧部和裂孔膜是它的主要屏障。")
39
病理:肾炎(nephritis)、肾病综合征(nephrotic syndrom)——蛋白尿(Proteinuria)
滤过膜带负电荷的涎基 或消失,导致带负电荷的血浆白蛋白滤过 ——蛋白尿

40
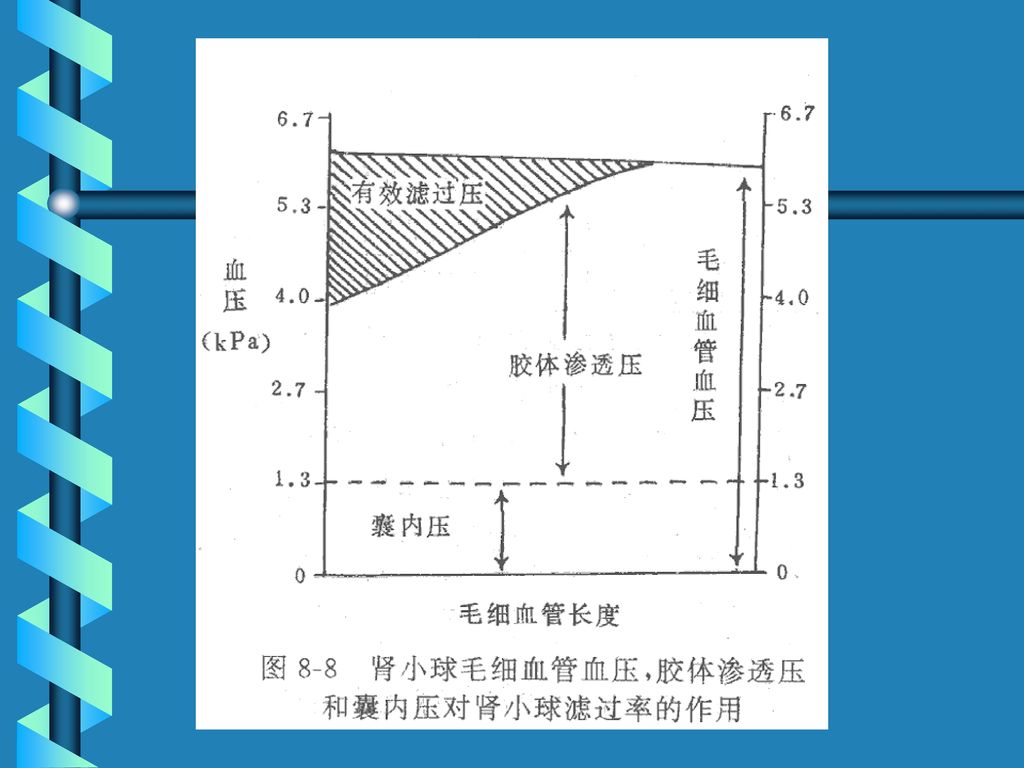
三、有效滤过压EFP(effective filtration pressure)
是肾小球 滤过作用的动力。 有效滤过压=肾小球毛细血管压 -(血浆胶体渗透压+肾小囊内压) EFP=glomerular hydrostatic pressure—(glomerular colloid osmotic pressure+Bowman’s capsule pressure) 用直接法测出,肾小球毛细血管压平均值约45mmHg (6.0Kpa) 40%主A平均压
 EFP=glomerular hydrostatic pressure—(glomerular colloid osmotic. pressure+Bowman’s capsule pressure) 用直接法测出,肾小球毛细血管压平均值约45mmHg (6.0Kpa) 40%主A平均压.")
41
入球端与出球端毛细血管压基本相等(下降1~2mmHg)
血浆胶体渗透压25mmHg,入球端20 mmHg,2.6Kpa 出球端35 mmHg,4.5Kpa 肾小囊内压 10 mmHg(1.3KPa) 入球端有效滤过压=45 -(20+10)=15 mmHg (1.4Kpa) 出球端有效滤过压=45 -(35+10)=0 mmHg
 入球端有效滤过压=45 -(20+10)=15 mmHg (1.4Kpa) 出球端有效滤过压=45 -(35+10)=0 mmHg.")
43
滤过平衡(filtration equilibrium)
通常超滤液(ultrafiltrate)在入球端毛细血管段中滤过产生,出球端有效滤过压为零,无法生成超滤液。 滤过平衡(filtration equilibrium)
在入球端毛细血管段中滤过产生,出球端有效滤过压为零,无法生成超滤液。 滤过平衡(filtration equilibrium)")
44
四、影响肾小球滤过的因素 ①滤膜通透性(permeability of glomerular capillary membrane)
②滤膜面积(area of glomerular capillary membrane) ,正常1.5m2以上 ③有效滤过压改变(the changes of EFP)
 ,正常1.5m2以上. ③有效滤过压改变(the changes of EFP)")
45
1.肾小球毛细血管的血压(Glomerular hydrostatic pressure)
全身动脉血压(artery pressure of total body)改变: 波动在80~180mmHg(10.7~24Kpa)时,通过自身调节,入球小A口径改变,使肾小球毛细血管压相对稳定,GFR基本保持不变。 AP<80mmHg(10.7KPa),肾小球毛细血管压相应 AP<40~50mmHg(5.3~6.7Kpa)时,有效滤过压为零,GFR=0,无尿 高血压(hypertension)晚期,入球小A硬化(sclerosis),GFR
改变: 波动在80~180mmHg(10.7~24Kpa)时,通过自身调节,入球小A口径改变,使肾小球毛细血管压相对稳定,GFR基本保持不变。 AP<80mmHg(10.7KPa),肾小球毛细血管压相应. AP<40~50mmHg(5.3~6.7Kpa)时,有效滤过压为零,GFR=0,无尿. 高血压(hypertension)晚期,入球小A硬化(sclerosis),GFR.")
46
2.肾小囊内压(bowman’s capsule pressure)
正常情况下比较稳定 病理情况如: 肾盂、输尿管结石(calculus of ureter)、肿瘤(tumor)——肾小囊内压 , 有效滤过压 ——GFR
、肿瘤(tumor)——肾小囊内压 , 有效滤过压 ——GFR.")
47
3.血浆胶体渗透压(glomerular colloid osmotic pressure)
正常情况下变化不大,如全身血浆蛋白(plasma protein) ——血浆胶渗压 (glomerular colloid osmotic pressure) ——EFP ——GFR
 ——血浆胶渗压 (glomerular colloid osmotic pressure) ——EFP ——GFR.")
48
4.肾小球血浆流量:对GFR影响较大 增大——血浆胶渗压在入球—出球小A之间的上升速度慢,具有滤过作用的毛细血管段加长,GFR
应激状态(如严重缺氧,中毒性休克)——交感N兴奋——肾内血管收缩——肾血流量 ——肾血浆流量 ——GFR
——交感N兴奋——肾内血管收缩——肾血流量 ——肾血浆流量 ——GFR.")
49
尿的一般理化特性 尿量(urine volume): 1000~2000ml/日 >2500ml/日 多尿(polyuria)
100~500 ml/日 少尿(oliguresis) <100ml/日 无尿(anuresis) 尿色:淡黄色 浓缩时变深 比重(specific density):1.015~1.025 波动范围:1.001~1.035
 <100ml/日 无尿(anuresis) 尿色:淡黄色 浓缩时变深. 比重(specific density):1.015~ 波动范围:1.001~")
50
pH: 5.0~7.0 正常最大波动范围4.5~8.0 成份 无机盐:NaCl、硫酸盐等 3~5%固体物 荤素杂食——尿呈酸性,pH约6.0
素食——尿呈碱性,碱基排出多 95~97%水 成份 无机盐:NaCl、硫酸盐等 3~5%固体物 有机物:尿素aquacare、 肌酐creatinine、马尿酸 hippuric acid、尿胆素urobilin

Similar presentations







,排出氢离子,维持酸.>")

 张明.>")

. 病因( Etiologe ) Primery Glomerular Diseases (60%) Hypertensive Nephrosclerosis Diabetic Glomerulosclerosis >")


>")

 基本内容:肾和排尿管道的一般结构、肾单位的组织结构与尿液生成的关系。>")

 Renal failure(RF)>")



 学 时:48 主讲人 姜文华.>")