Download presentation
1
急性毛细支气管炎的治疗现状与策略 新疆医科大学第一附属医院 小儿内二科 李敏

2
细支气管病变分类 原发性细支气管炎 -非特异性细支气管炎(阻塞性和急、慢性细支气管炎) 继发性细支气管病变(合并存在于大气道和肺实质病变)
-特征性细支气管炎(滤泡性细支气管炎、嗜酸性细支 气管炎) -特异性细支气管炎(弥漫性泛细支气管炎) 继发性细支气管病变(合并存在于大气道和肺实质病变)
 -特异性细支气管炎(弥漫性泛细支气管炎) 继发性细支气管病变(合并存在于大气道和肺实质病变)")
3
毛细支气管炎定义 感染性细支气管炎 “bronchiolitis”的译法尚不统一,有者译成“细支气管炎”,有者译为“毛细支气管炎”
急性细支气管炎(acute bronchiolitis) “bronchiolitis”的译法尚不统一,有者译成“细支气管炎”,有者译为“毛细支气管炎” 近年来,包括儿科教科书及实用儿科学等国内权威儿科专著,皆译为“毛细支气管炎” 3
 bronchiolitis 的译法尚不统一,有者译成 细支气管炎 ,有者译为 毛细支气管炎 近年来,包括儿科教科书及实用儿科学等国内权威儿科专著,皆译为 毛细支气管炎 3.")
4
毛细支气管炎(Bronchiolitis)
Bronchiolitis is a disorder most commonly caused in infants by viral lower respiratory tract infection; It is characterised by acute inflammation,oedema and necrosis of epithelial cells lining small airways,increased mucus production and bronchospasm ——American Academy of Pediatrics subcommittee 为婴儿期最常见的病毒性下呼吸道感染性疾病,其特征是细支气管的急性炎症、黏膜水肿、上皮细胞坏死脱落、黏液分泌增加和支气管痉挛。主要临床表现包括典型鼻炎、呼吸急促、喘息、咳嗽、肺部湿啰音、三凹征和(或)鼻翼扇动。 RSV is the most common respiratorypathogen in infancy, infecting nearly all children during the first years of life. About 40% of the infants develop a prominent inflammatory lung response, such as bronchiolitis or pneumonia Early RSV infection in life may be an important risk factor for the development of asthma and recurrent wheezing in childhood, especially children who are born premature have a greater susceptibility for serious infection. The risk of severe wheezing after RSV infection declines with age and is no longer significant after the first decade of life Five factors contribute to airway obstruction in bronchiolitis—oedema, inflammation, mucous plugging, bronchospasm, and necrosis— Bronchospasm:支气管痉挛 RSV毛细支气管炎典型的病理生理变化包括细支气管粘膜细胞肿胀,粘膜下水肿,细支气管周围单核细胞浸润,上皮细胞坏死,杯状细胞粘液分泌增加,大量粘液栓形成并阻塞小气道,导致气流受限,并产生一系列临床症状体征。 Wainwright C. Acute viral bronchiolitis in children – a very common condition with few therapeutic options. Paediatr Respir Rev 2010; 11: 39-45 Acute viral bronchiolitis is a clinically diagnosed condition causing significant morbidity and mortality in infancy. Children typically have a prodrome of coryzal symptoms including rhinorrhea and fever and develop increased work of breathing with wheeze and cough. There may be difficulty feeding and very young infants may present with apnoea. It is the most common lower respiratory tract condition and most common cause of admission to hospital in the first 12 months of life.1 Hospitalisation with bronchiolitis peaks between 3 and 6 months of life.2 Most children have a self limiting illness and are managed in the community although around 1-3% of all infants require admission to hospital. Over the last 20 years there has been an increase in the number of children admitted to hospital with bronchiolitis which is unexplained and the cause is likely to be multifactorial although it is possible that the use of pulse oximetry is related to the increased admission rates.3 Bronchiolitis is generally seasonal and associated with respiratory viral infections, most commonly respiratory syncytial virus (RSV).4 Death from bronchiolitis is thought to be rare although the risk of death increases substantially with pre-existing medical conditions.5 There are approximately 2.9 deaths per 100,000 population per year in infants infected with RSV and a respiratory cause of death under 12 months in the UK6 and around 5.3 deaths per 100,000 in the USA.7 Around 40-50% of infants requiring hospital admission with bronchiolitis will have recurrent episodes of wheeze4,8 and many infants have prolonged or relapsing symptoms of wheeze and cough lasting weeks or months following the acute episode.9 4
鼻翼扇动。 RSV is the most common respiratorypathogen in infancy, infecting nearly all children during the first years of life. About 40% of the infants develop a prominent inflammatory lung response, such as bronchiolitis or pneumonia. Early RSV infection in life may be an important risk factor for the development of asthma and recurrent wheezing in childhood, especially children who are born premature have a greater susceptibility for serious infection. The risk of severe wheezing after RSV infection declines with age and is no longer significant after the first decade of life. Five factors contribute to airway obstruction in bronchiolitis—oedema, inflammation, mucous plugging, bronchospasm, and necrosis— Bronchospasm:支气管痉挛. RSV毛细支气管炎典型的病理生理变化包括细支气管粘膜细胞肿胀,粘膜下水肿,细支气管周围单核细胞浸润,上皮细胞坏死,杯状细胞粘液分泌增加,大量粘液栓形成并阻塞小气道,导致气流受限,并产生一系列临床症状体征。 Wainwright C. Acute viral bronchiolitis in children – a very common. condition with few therapeutic options. Paediatr Respir Rev. 2010; 11: Acute viral bronchiolitis is a clinically diagnosed condition causing significant morbidity and mortality in infancy. Children typically have a prodrome of coryzal symptoms including rhinorrhea and fever and develop increased work of breathing with wheeze and cough. There may be difficulty feeding and very young infants may present with apnoea. It is the most common lower respiratory tract condition and most common cause of admission to hospital in the first 12 months of life.1 Hospitalisation with bronchiolitis peaks between 3 and 6 months of life.2 Most children have a self limiting illness and are managed in the community although around 1-3% of all infants require admission. to hospital. Over the last 20 years there has been an increase in the number of children admitted to hospital with bronchiolitis which is unexplained and the cause is likely to be multifactorial although it is possible that the use of pulse oximetry is related to the increased admission rates.3 Bronchiolitis is generally seasonal and associated with respiratory viral infections, most commonly respiratory syncytial virus (RSV).4 Death from bronchiolitis is thought to be rare although the risk of death increases substantially with pre-existing medical conditions.5 There are approximately 2.9 deaths per 100,000 population per year in infants infected with RSV and a respiratory cause of death under 12 months in the UK6 and around 5.3 deaths per 100,000 in the USA.7 Around 40-50% of infants requiring hospital admission with bronchiolitis will have recurrent episodes of wheeze4,8 and many infants have prolonged or relapsing symptoms of wheeze and cough lasting weeks or months following the acute episode")
5
毛细支气管炎(Bronchiolitis)
Bronchiolitis is a seasonal viral illness characterised by fever, nasal discharge and dry wheezy cough. On examination there are fine inspiratory crackles and/or wheeze 2006The Scottish Intercollegiate Guidelines Network RSV is the most common respiratorypathogen in infancy, infecting nearly all children during the first years of life. About 40% of the infants develop a prominent inflammatory lung response, such as bronchiolitis or pneumonia Early RSV infection in life may be an important risk factor for the development of asthma and recurrent wheezing in childhood, especially children who are born premature have a greater susceptibility for serious infection. The risk of severe wheezing after RSV infection declines with age and is no longer significant after the first decade of life Five factors contribute to airway obstruction in bronchiolitis—oedema, inflammation, mucous plugging, bronchospasm, and necrosis— Bronchospasm:支气管痉挛 RSV毛细支气管炎典型的病理生理变化包括细支气管粘膜细胞肿胀,粘膜下水肿,细支气管周围单核细胞浸润,上皮细胞坏死,杯状细胞粘液分泌增加,大量粘液栓形成并阻塞小气道,导致气流受限,并产生一系列临床症状体征。 Wainwright C. Acute viral bronchiolitis in children – a very common condition with few therapeutic options. Paediatr Respir Rev 2010; 11: 39-45 Acute viral bronchiolitis is a clinically diagnosed condition causing significant morbidity and mortality in infancy. Children typically have a prodrome of coryzal symptoms including rhinorrhea and fever and develop increased work of breathing with wheeze and cough. There may be difficulty feeding and very young infants may present with apnoea. It is the most common lower respiratory tract condition and most common cause of admission to hospital in the first 12 months of life.1 Hospitalisation with bronchiolitis peaks between 3 and 6 months of life.2 Most children have a self limiting illness and are managed in the community although around 1-3% of all infants require admission to hospital. Over the last 20 years there has been an increase in the number of children admitted to hospital with bronchiolitis which is unexplained and the cause is likely to be multifactorial although it is possible that the use of pulse oximetry is related to the increased admission rates.3 Bronchiolitis is generally seasonal and associated with respiratory viral infections, most commonly respiratory syncytial virus (RSV).4 Death from bronchiolitis is thought to be rare although the risk of death increases substantially with pre-existing medical conditions.5 There are approximately 2.9 deaths per 100,000 population per year in infants infected with RSV and a respiratory cause of death under 12 months in the UK6 and around 5.3 deaths per 100,000 in the USA.7 Around 40-50% of infants requiring hospital admission with bronchiolitis will have recurrent episodes of wheeze4,8 and many infants have prolonged or relapsing symptoms of wheeze and cough lasting weeks or months following the acute episode.9 5
.4 Death from bronchiolitis is thought to be rare although the risk of death increases substantially with pre-existing medical conditions.5 There are approximately 2.9 deaths per 100,000 population per year in infants infected with RSV and a respiratory cause of death under 12 months in the UK6 and around 5.3 deaths per 100,000 in the USA.7 Around 40-50% of infants requiring hospital admission with bronchiolitis will have recurrent episodes of wheeze4,8 and many infants have prolonged or relapsing symptoms of wheeze and cough lasting weeks or months following the acute episode")
7
毛细支气管炎 支气管:解剖上把直径在1mm以上有结缔组织鞘包绕的管道称为支气管(bronchi);
细支气管:管径小于1mm又无结缔组织包绕的称为细支气管(bronchioles 终末细支气管(呼吸性细支气管):内经在0.5mm以下的十七至十九级的气管, 7
:内经在0.5mm以下的十七至十九级的气管, 7.")
8
细支气管解剖生理特点 气管-主支气管-肺叶支气管-肺段、亚段支气管-小支气管-细支气管
第1~16级构成气体传导区,细支气管则是传导区的终点。 第17~19级是移行区,包括终末细支气管、呼吸性细支气管,此处已有部分呼吸功能。 从细支气管开始无软骨支撑,故呼气时易狭窄; 细支气管平滑肌发达呈环状,在各种刺激下易痉挛,造成呼气受阻、气体滞留(air trapping)和喘鸣。
和喘鸣。")
9
毛细支气管炎好发于冬春季 希腊的研究 Bronchiolitis is seasonal and appears more often in the fall and winter months. It is a very common reason for infants to be hospitalized during winter and early spring. 9 Arch Med Sci. 2012,8(3):
:")
10
Arch Pediatr Adolesc Med. 2012 Aug;166(8):700-6.
RSV是导致毛细支气管炎的常见病毒 美国一项关于毛细支气管炎病原学的前瞻性、多中心、连续3年的队列研究:共纳入2207例年龄小于2岁,第1次喘息发作的毛细支气管炎患儿 Slide 5 RSV是导致儿童毛细支气管炎的一种常见因素: 在阿根廷的一项多中心的临床研究中,包括1,278例小于5岁的急性下呼吸道感染住院患儿。在病毒阳性病例中78.2%检测到RSV(在所有病例中,有32%表现为病毒感染阳性) 。RSV检出率经统计学分析显著高于其他病毒(p<0.001).4 在北卡罗莱纳州一家私立儿科诊所的研究中,包括在超过11年的时间里( )来此接受急性呼吸道疾病治疗的患儿(年龄<15岁). 共有6,155例次, 其中1,851例次与喘息有关. 其中, RSV是最常见的病原, 在所有喘息病例中,有34%(135/1,851)可分离得到RSV,而年龄小于2岁的幼儿中有44% (90/909)发现RSV感染.5 另一项研究于1957至1970年,在华盛顿特区儿童医院开展,共分析了14,293例因呼吸道疾病接受治疗的婴儿及6岁以下儿童的咽拭子样品,其中4,387例还接受了血清样品的分析。病毒分离和血清学检测从总体上证实了,在所有呼吸道疾病住院患儿中,有25%感染了RSV,>40%的毛细支气管炎有RSV感染.6 A growing number of viruses have been associated with bronchiolitis although RSV remains the most commonly isolated virus (up to 75% of cases) and cases of bronchiolitis increase in peak RSV season.4 Reinfection with RSV is also common even in the same RSV season, although the primary infection is usually the most severe. Rhinovirus (RV) is the next most commonly associated virus16 although other viruses including human metapneumovirus (hMPV),17 human bocavirus,18 enteroviruses,adenovirus, influenza, human coronavirus and parainfluenza infection have also been associated with bronchiolitis.16 Although many viruses may cause the constellation of symptoms and signs that characterise bronchiolitis, 60–85% of cases are caused by respiratory syncytial virus (RSV).8 9 Every year between and children less than 5 years of age are hospitalised in the USA with RSV infections. Arch Pediatr Adolesc Med Aug;166(8):700-6. 4
 。RSV检出率经统计学分析显著高于其他病毒(p<0.001).4. 在北卡罗莱纳州一家私立儿科诊所的研究中,包括在超过11年的时间里( )来此接受急性呼吸道疾病治疗的患儿(年龄<15岁). 共有6,155例次, 其中1,851例次与喘息有关. 其中, RSV是最常见的病原, 在所有喘息病例中,有34%(135/1,851)可分离得到RSV,而年龄小于2岁的幼儿中有44% (90/909)发现RSV感染.5. 另一项研究于1957至1970年,在华盛顿特区儿童医院开展,共分析了14,293例因呼吸道疾病接受治疗的婴儿及6岁以下儿童的咽拭子样品,其中4,387例还接受了血清样品的分析。病毒分离和血清学检测从总体上证实了,在所有呼吸道疾病住院患儿中,有25%感染了RSV,>40%的毛细支气管炎有RSV感染.6. A growing number of viruses have been associated with bronchiolitis although RSV remains the most commonly isolated virus (up to 75% of cases) and cases of bronchiolitis increase in peak. RSV season.4 Reinfection with RSV is also common even in the same RSV season, although the primary infection is usually the most severe. Rhinovirus (RV) is the next most commonly. associated virus16 although other viruses including human metapneumovirus (hMPV),17 human bocavirus,18 enteroviruses,adenovirus, influenza, human coronavirus and parainfluenza. infection have also been associated with bronchiolitis.16. Although many viruses may cause the constellation of symptoms and signs that characterise bronchiolitis, 60–85% of cases are caused by respiratory syncytial virus (RSV).8 9 Every year between and children less than 5 years of age are hospitalised in the USA with RSV infections. Arch Pediatr Adolesc Med Aug;166(8):")
11
由于RSV 感染后机体不会出现长期或永久的免疫力,因此常常出现重复感染。
Although many viruses may cause the constellation of symptoms and signs that characterise bronchiolitis, 60–85% of cases are caused by respiratory syncytial virus (RSV).8 9 Every year between and children less than 5 years of age are hospitalised in the USA with RSV infections. 由于RSV 感染后机体不会出现长期或永久的免疫力,因此常常出现重复感染。 其他病毒如人类偏肺病毒(hMPV)、流感病毒、腺病毒和副流感病毒也可导致细支气管炎。 Nair H,, et al. Lancet ,2010;375:
.8 9 Every year between and children less than 5 years of age are hospitalised in the USA with RSV infections. 由于RSV 感染后机体不会出现长期或永久的免疫力,因此常常出现重复感染。 其他病毒如人类偏肺病毒(hMPV)、流感病毒、腺病毒和副流感病毒也可导致细支气管炎。 Nair H,, et al. Lancet ,2010;375:")
12
毛细支气管炎现有治疗 对症支持治疗 潜在治疗手段 氧疗 其他 喂养、补液 支气管扩张剂 气道湿化、吸痰 糖皮质激素口服或静脉滴注
针对毛细支气管炎的处理在全世界而言还未得到像哮喘那样很好的共识。对于毛细支气管炎的处理方案有许多不同观点和看法。加拿大、美国或澳大利亚治疗毛细支气管炎的方案与我国不完全一样,但总体上都给予干预,先对症处理。 其次是适当氧疗,尤其在美国,十分重视氧疗,在毛细支气管炎何种状况下给予什么程度的氧疗,如何间断,如何调节氧压等问题可以参照非常完善的指南。 关于喘憋控制,仍是首选支气管扩张剂(β2受体激动剂),欧美偏向于使用乙酰胆碱M受体阻滞剂(迷走神经兴奋抑制剂)来治疗,现在认为两者单用都不如联合应用疗效好。也有应用激素、硫酸镁。美国在激素使用方面十分慎重,尤其对于第一次喘息发作的患者,是担心低龄儿使用过多或者全身激素后影响肾上腺皮质将来的发育。 对于病毒本身的治疗至今未有理想的抗病毒药物。不提倡广泛使用病毒唑。因为病毒唑有消化道、血液、肝肾方面的副作用。 生物制品的研究以抗IgE单克隆抗体研究最为成功。丙种球蛋白有一定疗效,但远不如美国用于临床的抗IgE单克隆抗体对疾病的疗效肯定。但单克隆抗体价格昂贵,这是阻碍进一步推广的主要因素。 Sometimes, no treatment is necessary. Most medications do not help treat bronchiolitis. Antibiotics do not work against viral infections. Supportive therapy can include: Drinking plenty of fluids. Breast milk or formula are okay for children younger than 12 months. Electrolyte-balanced drinks, such as Pedialyte, are also okay to use in infants. Breathing moist (wet) air to help loosen sticky mucus. You can use a humidifier to moisten the air your child is breathing. Follow the directions that come with the humidifier. Getting plenty of rest. Not letting anyone smoke in the house, car, or anywhere near your child. Children in the hospital may need oxygen therapy and fluids given through a vein (IV). Rarely, antiviral medications, such as ribavirin, may be used to treat extremely ill children. 对症支持治疗 喂养、补液 气道湿化、吸痰 避免呼吸道不良刺激 清洁双手、隔离患者 氧疗 鼻导管、面罩吸氧 无创CPAP通气 机械通气 潜在治疗手段 支气管扩张剂 糖皮质激素口服或静脉滴注 高渗盐水雾化吸入 肾上腺素雾化吸入 白三烯受体拮抗剂 抗病原体制剂 其他 胸部物理治疗
,欧美偏向于使用乙酰胆碱M受体阻滞剂(迷走神经兴奋抑制剂)来治疗,现在认为两者单用都不如联合应用疗效好。也有应用激素、硫酸镁。美国在激素使用方面十分慎重,尤其对于第一次喘息发作的患者,是担心低龄儿使用过多或者全身激素后影响肾上腺皮质将来的发育。 对于病毒本身的治疗至今未有理想的抗病毒药物。不提倡广泛使用病毒唑。因为病毒唑有消化道、血液、肝肾方面的副作用。 生物制品的研究以抗IgE单克隆抗体研究最为成功。丙种球蛋白有一定疗效,但远不如美国用于临床的抗IgE单克隆抗体对疾病的疗效肯定。但单克隆抗体价格昂贵,这是阻碍进一步推广的主要因素。 Sometimes, no treatment is necessary. Most medications do not help treat bronchiolitis. Antibiotics do not work against viral infections. Supportive therapy can include: Drinking plenty of fluids. Breast milk or formula are okay for children younger than 12 months. Electrolyte-balanced drinks, such as Pedialyte, are also okay to use in infants. Breathing moist (wet) air to help loosen sticky mucus. You can use a humidifier to moisten the air your child is breathing. Follow the directions that come with the humidifier. Getting plenty of rest. Not letting anyone smoke in the house, car, or anywhere near your child. Children in the hospital may need oxygen therapy and fluids given through a vein (IV). Rarely, antiviral medications, such as ribavirin, may be used to treat extremely ill children. 对症支持治疗. 喂养、补液. 气道湿化、吸痰. 避免呼吸道不良刺激. 清洁双手、隔离患者. 氧疗. 鼻导管、面罩吸氧. 无创CPAP通气. 机械通气. 潜在治疗手段. 支气管扩张剂. 糖皮质激素口服或静脉滴注. 高渗盐水雾化吸入. 肾上腺素雾化吸入. 白三烯受体拮抗剂. 抗病原体制剂. 其他. 胸部物理治疗.")
13
缺乏特异性治疗 2011年系统回顾荟萃分析、近年文献、AAP指南,均一致性地认为现有的治疗药物对疾病结局未产生积极影响,包括全身使用或雾化吸入糖皮质激素、支气管舒张剂、口服白三烯受体拮抗剂等,抗菌药物无常规使用的指征,而利巴韦林吸入的疗效也有质疑。

14
缺乏特异性治疗 有推荐口服地塞米松、雾化吸入肾上腺素和雾化吸入3%高渗盐水等疗法,研究结果也不尽一致。
文献均推荐要细致观察、动态评估病情,首要治疗是支持疗法,保证及时的氧供和维持体液内环境平衡。强烈推荐监测经皮脉搏血氧饱和度(SPO2),当其低于92%应予吸氧。
,当其低于92%应予吸氧。")
15
48 trials (4897 patients, 13 comparisons) were included.
Only adrenaline (epinephrine) reduced admissions on day 1combined dexamethasone and adrenaline reduced admissions on day 7 A mixed treatment comparison supported adrenaline alone or combined with steroids as the preferred treatments for outpatients None of the interventions examined showed clear efficacy for length of stay among inpatients. RTC of children aged 24 months or less with a first episode of bronchiolitis with wheezing comparing any bronchodilator or steroid, alone or combined, with placebo or another intervention 48 trials (4897 patients, 13 comparisons) were included. 15
 reduced admissions on day 1combined. dexamethasone and adrenaline reduced admissions on day 7. A mixed treatment comparison supported adrenaline alone or combined with steroids as the preferred treatments for outpatients. None of the interventions examined showed clear efficacy for length of stay among inpatients. RTC of children aged 24 months or less with a first episode of bronchiolitis with wheezing comparing any bronchodilator or steroid, alone or combined, with placebo or another intervention. 48 trials (4897 patients, 13 comparisons) were included. 15.")
16
Results from meta-analysis of direct comparisons for admission rates from emergency department (day 1 and day 7) in outpatients. Only comparisons with quantitative results are shown

17
有证据表明急诊病人吸入肾上腺素可以降低1天后的住院率 有证据表明急诊病人吸入肾上腺素联合地塞米松可以降低7天 后的住院率
尚无有力的证据证实急性毛细支气管炎治疗的有效方法 有证据表明急诊病人吸入肾上腺素可以降低1天后的住院率 有证据表明急诊病人吸入肾上腺素联合地塞米松可以降低7天 后的住院率 对于住院病人无有效的干预措施可以缩短住院天数,但肾上腺 素联合糖皮质激素和沙丁氨醇可以改善症状评分

19
毛细支气管炎病理改变特点 Five factors contribute to airway obstruction in bronchiolitis—oedema, inflammation, mucous plugging, bronchospasm, and necrosis ——细支气管阻塞、细支气管周围炎,喘憋性呼吸困难 Five factors contribute to airway obstruction in bronchiolitis—oedema, inflammation, mucous plugging, bronchospasm, and necrosis—yet trials have focused on reversing only one or two of them. If each factor accounts for an equal proportion of obstruction, it is not surprising that reversal of one factor has a minimal effect on overall obstruction, whereas targeting two factors has a greater, yet still suboptimal, effect. Presumably, the combined α adrenergic and β adrenergic effects of adrenaline target oedema and bronchospasm; β agonists target only bronchospasm, dexamethasone targets inflammation, hypertonic saline decreases mucous plugging, and none of the current treatments reverses or prevents necrosis. Ascertaining the relative contribution of each factor for a given patient and its evolution over time is a major challenge. Yet,the findings imply that oedema, bronchospasm, and inflammation make an important contribution to acute and subacute airway obstruction in patients with mild and moderate bronchiolitis. In children admitted to hospital perhaps mucous plugging and necrosis play a greater role; 主要在直径为75~300μm的气道

20
诊断中的误区 哮喘的早发型或是病毒感染诱发的喘息很可能和毛细支气管炎的诊断重叠
由于毛细支气管炎与早发哮喘容易混淆,导致了一系列针对哮喘的试验性治疗,包括支气管扩张剂或是激素 但是,这两类药对于毛细支气管炎的患者均不能提供临床上的重要作用,并且增加了药物副作用的风险及费用

21
毛细支气管炎的治疗策略 正确诊断与鉴别诊断——试验性治疗 客观的病情评估——制定治疗方案 有效避免交叉感染——清洁双手,隔离患者
保持气道通畅、保证氧合——对症支持治疗 增强前瞻性——早期干预治疗

22
安全有效的治疗源于对疾病的正确诊断与病情评估

23
毛细支气管炎的诊断既简单又复杂 第1次出现喘息: 出现2次以上的喘息: 喘息迁延不愈: RSV感染引起的毛细支气管炎?(绝大多数为首次喘息)
哮喘第1次发作? 其他? 出现2次以上的喘息: RSV重复感染(在同一个RSV流行的季节,二次感染RSV的情况也很常见)? 哮喘? 喘息迁延不愈: 治疗不当? 合并感染? 诊断(哮喘?其他?)?
? 哮喘? 喘息迁延不愈: 治疗不当? 合并感染? 诊断(哮喘?其他?)?")
24
毛细支气管炎的诊断程序 1 季节、年龄 特质、病史 发热、喘息 体征、检查 病原、影像 2 3 临床特征 治疗反应 除外其他疾病
支气管炎患儿出现严重细菌感染的几率较低,因此血常规检查对细支气管炎的诊断和治疗毫无作用 流行季节进行RSV病毒检测具有很高的预测价值,但是对大多数经临床诊断的患儿的治疗及预后并无影响 细支气管炎患儿胸片可出现异常,但其与病情严重程度的关系也不确定,因此临床上不推荐常规行胸片检查。 住院患儿若对治疗的反应欠佳,需进一步评估病情严重程度或怀疑其他诊断时,则应行影像学检查 鉴别诊断:应与该年龄段引起喘憋或呼吸困难的相关疾病鉴别细细支气管炎患儿出现严重细菌感染的几率较低, 1a. Clinicians should diagnose bronchiolitis and assess disease severity on the basis of history and physical examination. Clinicians should not routinely order laboratory and radiologic studies for diagnosis (recommendation). 1 季节、年龄 特质、病史 发热、喘息 体征、检查 病原、影像 2 清洁双手、隔离患者 吸氧、呼吸道管理 高渗盐水雾化吸入 肾上腺素雾化吸入 支气管扩张剂 糖皮质激素 白三烯受体拮抗剂 3 哮喘;哮吼、百日咳、肺炎、粟粒性结核;喉气管软化、先天性肺疾病或膈、支气管囊肿、气管食管瘘;气管异物;囊性纤维化;胃食管反流、、先心病、心内弹、血管环、过敏反应 临床特征 治疗反应 除外其他疾病
. 1. 季节、年龄. 特质、病史. 发热、喘息. 体征、检查. 病原、影像. 2. 清洁双手、隔离患者. 吸氧、呼吸道管理. 高渗盐水雾化吸入. 肾上腺素雾化吸入. 支气管扩张剂. 糖皮质激素. 白三烯受体拮抗剂. 3. 哮喘;哮吼、百日咳、肺炎、粟粒性结核;喉气管软化、先天性肺疾病或膈、支气管囊肿、气管食管瘘;气管异物;囊性纤维化;胃食管反流、、先心病、心内弹、血管环、过敏反应. 临床特征. 治疗反应. 除外其他疾病.")
25
男,8月,咳嗽喘息20余天 右主支气管软化 右主支气管软化 8月、男 以“反复喘息4个月”为主诉入院
出生后4月起无明显诱因反复出现喘息,喉部可闻及“呼噜声”,曾诊断“毛细支气管炎”、“哮喘”,持续吸入普米克,每次半支日2次,联合口服顺尔宁近3个月,喘息症状时好时坏,运动后喉部喘鸣音明显,经常需间断联合可必特吸入,改用辅舒酮+储雾罐吸入1个月,喘息症状仍无明显好转 既往无湿疹史;无药物及食物过敏史;否认家族过敏性疾病病史 查体发现剧烈运动后可闻及喘鸣音(双相) 右主支气管软化 25
26
病情的评估 1. 喂养、吃奶情况;2. 有无呼吸困难及程度;3. 是否需要吸氧4. 有无呼吸暂停;5. 有无意识改变 26
Dominic A. Bronchiolitis: assessment and evidence-based management MJA 2004; 180 (8): 26
:")
27
严重毛细支气管炎的危险因素 ——环境与宿主
Clinicians should assess risk factors for severe disease such as age less than 12 weeks, a history of prematurity, underlying cardiopulmonary disease,or immunodeficiency when making decisions about evaluation and management of children with bronchiolitis (recommendation). 越来越多的临床研究也发现,大多数重症RSV感染患儿并不存在明确的危险因素 环境因素: 生活贫困、被动吸烟、空气污染、居住拥挤、幼儿园长托 宿主因素:早产儿、低出生体重儿、先天性心脏病、早产儿慢性肺疾病、神经系统疾病、6个月以下婴儿(尤其年龄<12周)、免疫功能低下、缺乏母乳喂养 Green RG, et al. South African guideline for the diagnosis, management and prevention of acute viral bronchiolitis in children S Afr Med J 2010 27
. 越来越多的临床研究也发现,大多数重症RSV感染患儿并不存在明确的危险因素. 环境因素: 生活贫困、被动吸烟、空气污染、居住拥挤、幼儿园长托. 宿主因素:早产儿、低出生体重儿、先天性心脏病、早产儿慢性肺疾病、神经系统疾病、6个月以下婴儿(尤其年龄<12周)、免疫功能低下、缺乏母乳喂养. Green RG, et al. South African guideline for the diagnosis, management and prevention of acute viral bronchiolitis in children S Afr Med J")
28
严重毛细支气管炎的危险因素 ——混合感染 对于免疫功能正常的儿童,毛细支气管炎通常是自限性疾病,继发细菌感染并不常见 免疫功能不全的儿童,或是比较病情严重的儿童,继发细菌感染的比率增加。合并有细菌性下呼吸道感染是否是严重疾病的原因或标志还不清楚

29
RSV引起的毛细支气管炎的儿童中,发生菌血症的危险因素包括:
严重毛细支气管炎的危险因素 ——混合感染 RSV引起的毛细支气管炎的儿童中,发生菌血症的危险因素包括: 严重的临床表现 入重症监护室 院内感染的RSV 紫绀型先天性心脏病 在呼吸道病毒中合并非典型细菌感染(如肺炎支原体、沙眼衣原体等)后,可能会导致儿童急性细支气管炎的病情加重
后,可能会导致儿童急性细支气管炎的病情加重.")
30
病情的动态评价 1 2 3 4 呼吸症状对进食脱水情况的影响 患儿对治疗的反应 患儿家庭照料患儿的能力及能否及时复诊
毛细支气管炎病程多变,且呈动态进展,轻者可表现为短暂性发作,重者则可发展至进行性呼吸衰竭。因此,需动态评价病情 1 呼吸症状对进食脱水情况的影响 2 患儿对治疗的反应 3 患儿家庭照料患儿的能力及能否及时复诊 4 是否存在早产、心肺疾病、免疫缺陷状态和先前喘息发作病史等

31
根据病情制定治疗方案

32
The management of children with bronchiolitis.
关于小儿毛细支气管炎的治疗 The management of children with bronchiolitis.

33
轻症毛支的处理 多数急性病毒性毛细支气管炎为自限性疾病,多为轻症,患儿可以在家护理,应注意患儿的喂养和呼吸状况
Paediatr Respir Rev Mar;11(1):39-45; quiz 45. Epub 2009 Nov 26. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Wainwright C. Source Department of Paediatrics and Child Health, Queensland Children's Respiratory Centre, Royal Children's Hospital, University of Queensland, Herston Rd, Herston, Queensland, Australia Abstract Acute viral bronchiolitis remains a cause of substantial morbidity and health care costs in young infants. It is the most common lower respiratory tract condition and most common reason for admission to hospital in infants. Many respiratory viruses have been associated with acute viral bronchiolitis although respiratory syncytial virus (RSV) remains the most frequently identified virus. Most infants have a mild self limiting illness while others have more severe illness and require hospital admission and some will need ventilatory support. Differences in innate immune function in response to the respiratory viral insult as well as differences in the geometry of the airways may explain some of the variability in clinical pattern. Young age and history of prematurity remain the most important risk factors although male gender, indigenous status, exposure to tobacco smoke, poor socioeconomic factors and associated co-morbidities such as chronic lung disease and congenital heart disease increase the risks of more severe illness. Supportive therapy remains the major treatment option as no specific treatments to date have been shown to provide clinically important benefits except for inhaled hypertonic saline. Prophylaxis of high risk infants with palivizumab should be considered although the cost effectiveness is still unclear. Many questions remain regarding optimal management approaches for infants requiring hospitalisation with bronchiolitis including use of nasogastric feeding, the optimal role of supplemental oxygen, optimal use of hypertonic saline and the role of combinations of therapies, the use of heliox or modern physiotherapy approaches. Copyright 2009 Elsevier Ltd. All rights reserved. 轻症毛支的处理 多数急性病毒性毛细支气管炎为自限性疾病,多为轻症,患儿可以在家护理,应注意患儿的喂养和呼吸状况 主要处理为很好的对症支持治疗,而无需特殊的处理 Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews 2010 Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews 2010 Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews 2010 Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews 2010
:39-45; quiz 45. Epub 2009 Nov 26. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Wainwright C. Source. Department of Paediatrics and Child Health, Queensland Children s Respiratory Centre, Royal Children s Hospital, University of Queensland, Herston Rd, Herston, Queensland, Australia Abstract. Acute viral bronchiolitis remains a cause of substantial morbidity and health care costs in young infants. It is the most common lower respiratory tract condition and most common reason for admission to hospital in infants. Many respiratory viruses have been associated with acute viral bronchiolitis although respiratory syncytial virus (RSV) remains the most frequently identified virus. Most infants have a mild self limiting illness while others have more severe illness and require hospital admission and some will need ventilatory support. Differences in innate immune function in response to the respiratory viral insult as well as differences in the geometry of the airways may explain some of the variability in clinical pattern. Young age and history of prematurity remain the most important risk factors although male gender, indigenous status, exposure to tobacco smoke, poor socioeconomic factors and associated co-morbidities such as chronic lung disease and congenital heart disease increase the risks of more severe illness. Supportive therapy remains the major treatment option as no specific treatments to date have been shown to provide clinically important benefits except for inhaled hypertonic saline. Prophylaxis of high risk infants with palivizumab should be considered although the cost effectiveness is still unclear. Many questions remain regarding optimal management approaches for infants requiring hospitalisation with bronchiolitis including use of nasogastric feeding, the optimal role of supplemental oxygen, optimal use of hypertonic saline and the role of combinations of therapies, the use of heliox or modern physiotherapy approaches. Copyright 2009 Elsevier Ltd. All rights reserved. 轻症毛支的处理. 多数急性病毒性毛细支气管炎为自限性疾病,多为轻症,患儿可以在家护理,应注意患儿的喂养和呼吸状况. 主要处理为很好的对症支持治疗,而无需特殊的处理. Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews")
34
住院标准 年龄 病程 有无高危因素 呼吸困难的严重程度 有无进食及喂养困难 社会及经济状况 进食喂养困难 嗜睡
Any of the following features should lead to further review and referral for hospital admission:43 a history of apnoea difficulty feeding may require supportive care and if infants have taken less than 50% of their usual fluid intake in the preceding 24 hours hospital admission is required severe respiratory distress with accessory muscle use or grunting Respiratory rate greater than 60 diagnostic uncertainty cyanosis/ haemoglobin saturation 92% in room air Around 1–3% of infants may require admission to paediatric intensive care. Criteria for referral and admission to intensive care will vary between hospitals however infants with severe respiratory distress, exhaustion, failure to maintain haemoglobin saturation above 92–94% with supplemental oxygen or with recurrent apnoea should be considered for intensive care consultation. 住院标准 进食喂养困难 嗜睡 呼吸频率>70次/min 出现鼻翼煽动和/或呻吟 三凹症 血氧饱和度<95% 年龄 病程 有无高危因素 呼吸困难的严重程度 有无进食及喂养困难 社会及经济状况 Wainwright C. Acute viral bronchiolitis in children- a very common condition with few therapeutic options. Paediatric Respiratory Reviews 2010

35
防止交叉感染 ——清洁双手,隔离患者 洗手是预防RSV院内传播的最重要措施:在与患儿直接接触前后,接触邻近患儿的物体后,以及摘手套后,均应洗手(B级) 首选以酒精为主的擦手剂,其次为有抗微生物作用的肥皂(B级) 医师应教育患儿及其家庭成员注意手部卫生(B级) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):
 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):")
36
支持治疗——鼻饲和静脉输液 对患儿的吃奶进食、饮水情况及有无脱水进行评估非常重要 少量多次喂养 母乳喂养 鼻饲 静脉输液 尽量减不良少刺激
Inadequate feeding is usually due to respiratory distress and the resulting increased work of breathing. The combination of tachypnoea, bouts of coughing and increased upper airway secretions can result in inadequate fluid intake. Furthermore,tachypnoea increases fluid loss, potentially hasteningd ehydration. It is strongly recommended that clinicians should assess hydration and ability to take fluids orally [1] Frequent small foods are often used but nasogastric or intravenous fluids may be required to maintain hydration. However, fluid replacement strategies have not been validated in randomised controlled trials (RCTs). A recent study comparing management of acute viral bronchiolitis between different centres in Australia and New Zealand concluded that practice is equally split between nasogastric and intravenous hydration, reflecting the current lack of evidence [10]. 【1】American Academy of Pediatrics. Diagnosis and management of bronchiolitis. Pediatrics 2006; 118: 对患儿的吃奶进食、饮水情况及有无脱水进行评估非常重要 少量多次喂养 母乳喂养 鼻饲 静脉输液 尽量减不良少刺激
. A recent study comparing management of acute viral bronchiolitis between different centres in Australia and New Zealand concluded that practice is equally split between nasogastric and intravenous hydration, reflecting the current lack of evidence [10]. 【1】American Academy of Pediatrics. Diagnosis and management of bronchiolitis. Pediatrics 2006; 118: 对患儿的吃奶进食、饮水情况及有无脱水进行评估非常重要. 少量多次喂养. 母乳喂养. 鼻饲. 静脉输液. 尽量减不良少刺激.")
37
呼吸支持—— 吸痰、吸氧 吸痰、吸氧是毛细之气管炎最主要和最基本的治 疗 鼻部吸痰,操作轻柔 俯卧位可以改善氧合 鼻部吸痰,操作要轻柔
血氧饱和度(SpO2) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4): 37
 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):")
38
呼吸支持—— 吸痰、吸氧 SpO2降至90%以下为氧疗指征,若SpO2持续低于90%, 则应通过足够的氧疗使SpO2升至90%或以上
若患儿的SpO2≥90%,且进食良好,仅有轻微呼吸窘迫, 则可停用氧疗(D级) 若患儿临床状况改善,则无需持续监测SpO2(D级) 对于有明显血流动力学异常的心肺疾病史或早产史的患儿 在准备停用氧疗时应给予密切监测(B级) 鼻部吸痰,操作要轻柔 血氧饱和度(SpO2) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4): 38
 若患儿临床状况改善,则无需持续监测SpO2(D级) 对于有明显血流动力学异常的心肺疾病史或早产史的患儿 在准备停用氧疗时应给予密切监测(B级) 鼻部吸痰,操作要轻柔. 血氧饱和度(SpO2) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):")
39
支气管扩张剂 目前对于支气管扩张剂的应用仍有争议 不推荐常规应用支气管扩张剂 (B级)
Kellner等的一项系统评价对8项随机对照研究(RCT,共计394例患儿)进行了分析。 结果显示,每4例应用支气管扩张剂的患儿中最多有1例的临床评分可获得短暂改善,但临床意义还不清楚。 Clinicians should assess risk factors for severe disease such as age less than 12 weeks, a history of prematurity, underlying cardiopulmonary disease, or immunodeficiency when making decisions about evaluation and management of children with bronchiolitis (recommendation). 目前对于支气管扩张剂的应用仍有争议 不推荐常规应用支气管扩张剂 (B级) 可谨慎地试验性应用α肾上腺素能或β肾上腺素能类药物;仅在客观评估表明吸入支气管扩张剂有效时,方可持续应用这类药物 (B级) 评估支气管扩张剂对长期转归的影响的研究显示,应用支气管扩张剂对总病程并无影响 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):
进行了分析。 结果显示,每4例应用支气管扩张剂的患儿中最多有1例的临床评分可获得短暂改善,但临床意义还不清楚。 Clinicians should assess risk factors for severe disease such as age less than 12 weeks, a history of prematurity, underlying cardiopulmonary disease, or immunodeficiency when making decisions about evaluation and management of children with bronchiolitis (recommendation). 目前对于支气管扩张剂的应用仍有争议. 不推荐常规应用支气管扩张剂 (B级) 可谨慎地试验性应用α肾上腺素能或β肾上腺素能类药物;仅在客观评估表明吸入支气管扩张剂有效时,方可持续应用这类药物 (B级) 评估支气管扩张剂对长期转归的影响的研究显示,应用支气管扩张剂对总病程并无影响. American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):")
40
支气管扩张剂 对不同支气管扩张剂进行的研究显示,门诊短期应用沙丁胺醇可改善患儿的氧饱和度和(或)临床评分,但住院患儿应用此类药物不能显著改善临床表现,对病程和住院时间也没有影响 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4): 40
:")
41
肾上腺素雾化吸入治疗 门诊应用肾上腺素有一定短期疗效,但肾上腺素对门诊及住院患儿均无长期疗效 肾上腺素作用略优于沙丁胺醇
Its treatment by epinephrine was first suggested in 1987 by Wohl and Chernick[5] 肾上腺素雾化吸入治疗 门诊应用肾上腺素有一定短期疗效,但肾上腺素对门诊及住院患儿均无长期疗效 肾上腺素作用略优于沙丁胺醇 可能与其作用于α肾上腺素能受体引起气道粘膜血管收缩,减轻气道粘膜水肿有关 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4): 41
:")
42
肾上腺素组:肾上腺0.1ml/kg(1:10000),雾化吸入
舒喘灵组:0.15mg/kg,雾化吸入 间隔20min 1次,连续3次 结论:肾上腺素雾化吸入可以缩短住院时间、降低RDAI评分, 用肾上腺素替代舒喘灵治疗急性毛细支气管炎可能更有效。

43
高渗盐水雾化吸入治疗 增加黏膜纤毛的清除功能,减轻气道水肿、稀释痰液减少黏液阻塞,刺激咳嗽反射等增加气道清除能力
11篇同质论文,包括8556例轻-中度毛支炎,与生理盐水雾化比较,3%盐水雾化4-6次/天,于治疗1-3天时减轻临床评分,减少住院率,缩短住院时间,安全性好 Bialy L Foisy M, Smith M,et al. Evidence-Based Child health 2011, 43

44
糖皮质激素 关于糖皮质激素治疗毛细支气管炎存在争议 地塞米松口服治疗毛细支气管炎无效
——Mesquita M, et al. Allergol lmmunopathol (Madr). 2009Mar-Apr;37(2):63-7 地塞米松治疗毛细支气管炎无效 —Patel H,Platt R,Lozano JM. Cochrane Database Syst Rev.2010;10:CD004878 泼尼松治疗婴幼儿博卡病毒性喘息无效 ——Jartti T, Pediatr Infect Dis J Jun;30(6):521-3 口服泼尼松龙可减轻病毒感染性喘息的症状 ——Jartti T, et al. Allergy Immunol.2007 Jun;18(4):326-34 口服泼尼松龙可降低病毒性毛细支气管炎后反复喘息发作,合并湿疹者的效果更好 ——Lehtinen P, et al. Allergy Clin Immunol Mar;119(3):570-5.Epub 2006 Dec 27)
. 2009Mar-Apr;37(2):63-7. 地塞米松治疗毛细支气管炎无效. —Patel H,Platt R,Lozano JM. Cochrane Database Syst Rev.2010;10:CD 泼尼松治疗婴幼儿博卡病毒性喘息无效. ——Jartti T, Pediatr Infect Dis J Jun;30(6): 口服泼尼松龙可减轻病毒感染性喘息的症状. ——Jartti T, et al. Allergy Immunol.2007 Jun;18(4): 口服泼尼松龙可降低病毒性毛细支气管炎后反复喘息发作,合并湿疹者的效果更好. ——Lehtinen P, et al. Allergy Clin Immunol Mar;119(3):570-5.Epub 2006 Dec 27)")
45
皮质激素药物不作为毛细支气管炎的常规治疗
糖皮质激素 RECOMMENDATION 3 皮质激素药物不作为毛细支气管炎的常规治疗 Corticosteroid medications should not be used routinely in the management of bronchiolitis (recommendation: evidence level B; based on RCTs with limitations and a preponderance of riskover benefit) 毛细支气管炎是否无需使用糖皮质激素?
 毛细支气管炎是否无需使用糖皮质激素?")
46
雾化吸入布地奈德治疗RSV毛细支气管炎的近期疗效
#第1个8周治疗结果未显示统计学差异 第2个8周#治疗后喘息症状发作情况 *与安慰剂组比较 P<0.05 16%* 19%* 47% 喘息发作患儿的比例(%) & && (n=34) (n=32) 一项随机、对照的研究,100名年龄<24月在医院接受治疗的急性毛细支气管炎患儿,34名接受雾化吸入色甘酸钠治疗,第1个8周,20mg,4次/日,第2个8周20mg,3次/日;34名患儿接受雾化吸入布地奈德治疗,第1个8周,500μg,2次/日,第2个8周250μg, 2次/日;对照组32名患儿不接受治疗。在家中,患儿可以按需使用口服支气管扩张剂(如硫酸特布他林或沙丁胺醇)。建议所有患儿急性毛细支气管炎后使用口服支气管扩张剂1周。如果研究期间有指征需要额外的维持治疗,建议口服茶碱缓释片。 &第1个8周,20mg,4次/日;第2个8周20mg,3次/日 & &第1个8周,500μg,2次/日;第2个8周250μg, 2次/日 Reijonen T et al Arch Pediatr Adolesc Med. 1996 46
 & && (n=34) (n=32) 一项随机、对照的研究,100名年龄<24月在医院接受治疗的急性毛细支气管炎患儿,34名接受雾化吸入色甘酸钠治疗,第1个8周,20mg,4次/日,第2个8周20mg,3次/日;34名患儿接受雾化吸入布地奈德治疗,第1个8周,500μg,2次/日,第2个8周250μg, 2次/日;对照组32名患儿不接受治疗。在家中,患儿可以按需使用口服支气管扩张剂(如硫酸特布他林或沙丁胺醇)。建议所有患儿急性毛细支气管炎后使用口服支气管扩张剂1周。如果研究期间有指征需要额外的维持治疗,建议口服茶碱缓释片。 &第1个8周,20mg,4次/日;第2个8周20mg,3次/日. & &第1个8周,500μg,2次/日;第2个8周250μg, 2次/日. Reijonen T et al Arch Pediatr Adolesc Med")
47
雾化吸入布地奈德治疗RSV毛细支气管炎的近期疗效
第2个8周治疗后因遗传性过敏体质发生喘息而住院的患儿比例 20 40 60 80 100 10%* 19%* 因遗传性过敏体质发生喘息而住院患儿的比例(%) 雾化吸入布地奈德组& 雾化吸入色甘酸钠&& 对照组 *与安慰剂组比较P<0.05 40% (n=34) (n=32) &第1个8周,20mg,4次/日;第2个8周20mg,3次/日 & &第1个8周,500μg,2次/日;第2个8周250μg, 2次/日 Reijonen T et al Arch Pediatr Adolesc Med. 1996
 雾化吸入布地奈德组& 雾化吸入色甘酸钠&& 对照组. *与安慰剂组比较P< % (n=34) (n=32) &第1个8周,20mg,4次/日;第2个8周20mg,3次/日. & &第1个8周,500μg,2次/日;第2个8周250μg, 2次/日. Reijonen T et al Arch Pediatr Adolesc Med")
48
关于白三烯调节剂 由于缺乏足够的资料,因此还无法评价白三烯调节剂在细支气管炎中的作用
American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):
:")
49
关于利巴韦林及抗生素 不推荐常规应用利巴韦林 菌血症在婴幼儿毛细支气管炎中非常少见 (<1%)
婴幼儿毛细支气管炎不推荐常规应用抗生素,除非有明确的指征证实存在呼吸机相关性肺炎 不恰当的抗生素应用使患儿暴露于药物相关的不良事件中,增加了抗生素耐药的风险,必须加以避免 抗生素仅用于有毛细支气管炎有明确的细菌混合性感染指征时

50
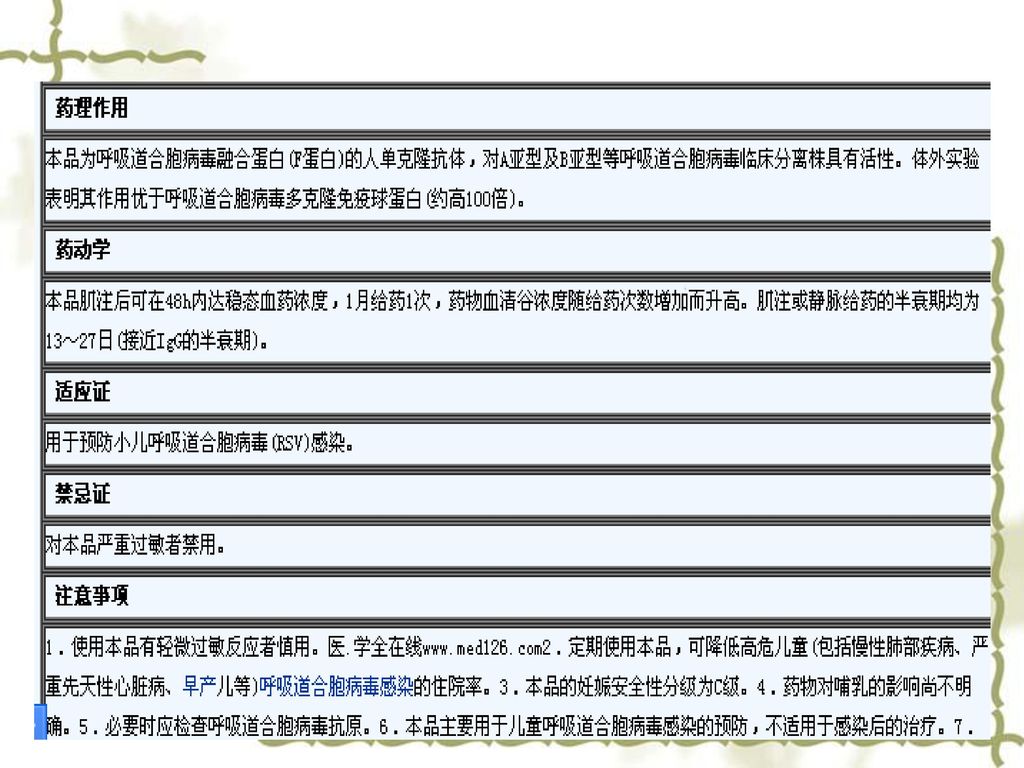
帕利珠单抗 帕利珠单抗用药方案为每次15 mg/kg肌注,1次/月,连用5个月,多始于每年的11月或12月(C级)
CLD、早产儿(<35周)或先天性心脏病患儿可给予帕利珠单抗预防治疗(A级) 帕利珠单抗用药方案为每次15 mg/kg肌注,1次/月,连用5个月,多始于每年的11月或12月(C级) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):
或先天性心脏病患儿可给予帕利珠单抗预防治疗(A级) 帕利珠单抗用药方案为每次15 mg/kg肌注,1次/月,连用5个月,多始于每年的11月或12月(C级) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis.Diagnosis and management of bronchiolitis. Pediatrics 2006; 118(4):")
52
沙丁胺醇 肾上腺素

53
总 结 毛细支气管炎是婴幼儿时期常见的、与季节相关的病毒性呼吸道感染性疾病,75%以上由RSV引起
总 结 毛细支气管炎是婴幼儿时期常见的、与季节相关的病毒性呼吸道感染性疾病,75%以上由RSV引起 大多数毛细支气管炎为自限性疾病 ,患儿可在家中处理,约10%的患儿需要住院治疗 早产、慢性肺疾病、先天性心脏病等是RSV感染毛细支气管炎患儿病情加重,甚至死亡的高危因素 目前尚无药物可以改变毛细支气管炎的自然病程,无特异性的治疗方案 There are few effective therapeutic options. Supportive care remains the cornerstone of management The use of hypertonic saline seems to be beneficial The use of heliox and non invasive ventilation for infants with severe disease appears promising There is no evidence that drug treatment alters its natural course. optimal supportive care including use of nasal suction,and optimal fluid management with nasogastric or intravenous fluids. The use of inhaled hypertonic saline seems to be beneficial in reducing clinical severity and hospital stay 毛细支气管炎是婴幼儿时期常见的、与季节相关的病毒性呼吸道感染性疾病,75%以上由呼吸道合胞病毒引起 大多数毛细支气管炎为自限性疾病 ,患儿可在家中处理,仅大约1~3%的患儿需要住院治疗 早产、先天性心脏病等是RSV感染毛细支气管炎患儿病情加重,甚至死亡的高危因素 目前尚无药物可以改变毛细支气管炎的自然病程,也缺乏有效的治疗方法 支持治疗仍然是治疗的基石,最佳的支持治疗包括:吸痰、液体疗法(鼻饲、静脉输液) 高渗盐水雾化吸入可以减轻疾病的严重程度和缩短住院时间 无创通气可减少重症毛细支气管炎患儿
 高渗盐水雾化吸入可以减轻疾病的严重程度和缩短住院时间. 无创通气可减少重症毛细支气管炎患儿.")
54
总 结 对症支持治疗仍然是毛细支气管炎治疗的基石,最佳的支持治疗包括:给氧、补液、保持气道通畅、防止交叉感染
总 结 对症支持治疗仍然是毛细支气管炎治疗的基石,最佳的支持治疗包括:给氧、补液、保持气道通畅、防止交叉感染 肾上腺素雾化吸入可能对门诊病人有效,减少住院率 B2受体激动剂和异丙托溴胺联合吸入治疗可能有效 国际上不推荐常规使用糖皮质激素治疗 无创通气可减少重症毛细支气管炎患儿气管插管的机会 个体化治疗、避免过度治疗

55
PDCA——一步一步的策略

56
Thank you for your attention !



家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")
 的制定及临床应用体会 北京朝阳医院 呼吸与危重症医学科 曹志新 2009-10-27.>")







是 一 种脂溶性抗氧化剂。其 分布非常广泛,几乎存在 身体所有的部分.>")







>")
