Download presentation
Presentation is loading. Please wait.

1
皮肤粘膜淋巴结综合征 ( 川崎病 ) Mucocutaneous Lymphnode Syndrome,MCLS (Kawasaki Disease, KD ) 皮肤粘膜淋巴结综合征 ( 川崎病 ) Mucocutaneous Lymphnode Syndrome,MCLS (Kawasaki Disease, KD ) 新疆医科大学第一临床医学院儿科教研室
 Mucocutaneous Lymphnode Syndrome,MCLS (Kawasaki Disease, KD ) 皮肤粘膜淋巴结综合征 ( 川崎病 ) Mucocutaneous Lymphnode Syndrome,MCLS (Kawasaki Disease, KD ) 新疆医科大学第一临床医学院儿科教研室")
2
教 学 大 纲 教 学 大 纲 教学目的: 在了解川崎病的病因和病理过程的基础上 掌握该病的临床表现、诊断标准和治疗。 教学要求: 1 、了解本病的病因和病理过程。 2 、掌握本病的临床表现与诊断标准和治疗。

3
Dr.Kawasaki

4
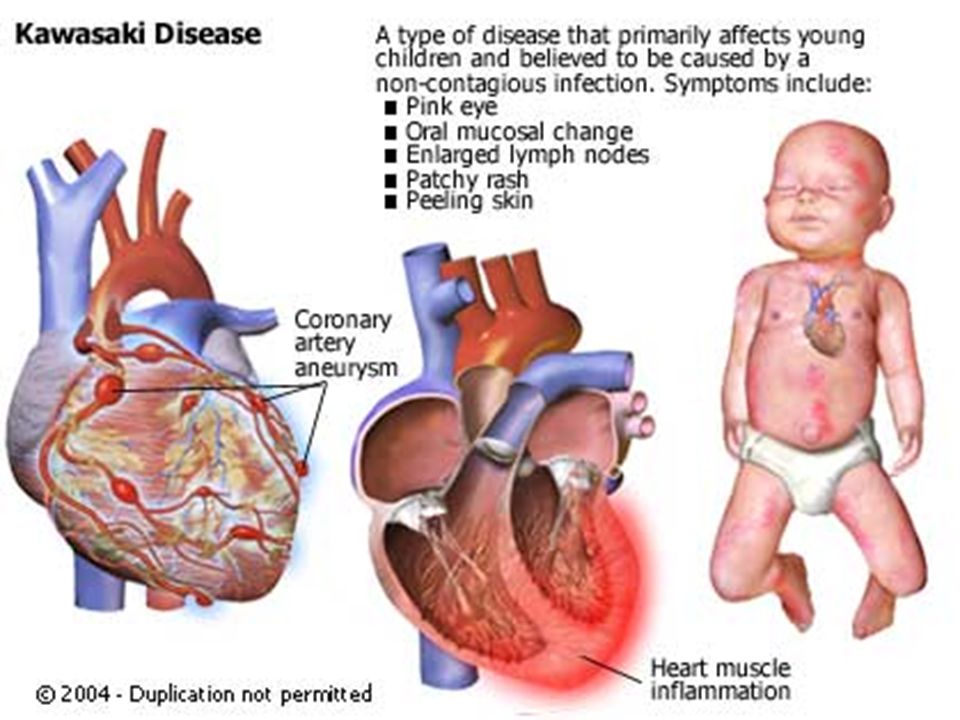
概 况 Outline 全身血管炎 ( 中、小动脉 ) 为主要病理改变 Generalized systemic vasculitis 急性发热性出疹性疾病 An acute, febrile disease with rash 儿童后天获得性心脏病的主要病因之一 One of the leading causes of acquired heart disease in children
 为主要病理改变 Generalized systemic vasculitis 急性发热性出疹性疾病 An acute, febrile disease with rash 儿童后天获得性心脏病的主要病因之一 One of the leading causes of acquired heart disease in children")
5
可并发缺血性心脏病或猝死 May lead to ischemic heart disease or sudden death 1967 年日本学者首先报道 First described in Japan in 1967 by Dr.Kawasaki

6
发病率 ( Annual incidence) : 日本 — 108-111.7/10 万 (97 - 98 年 ) 澳大利亚- 5.5/10 万 (93-94 年) 瑞典- 6.2/10 万( 91-92 年) 智利- 2.9/ 10 万( 92-94 年) 美国白种人- 9/10 万 美国亚裔 32.5/10 万 临床流行病学资料
 : 日本 — /10 万 (97 - 98 年 ) 澳大利亚- 5.5/10 万 (93-94 年) 瑞典- 6.2/10 万( 年) 智利- 2.9/ 10 万( 年) 美国白种人- 9/10 万 美国亚裔 32.5/10 万 临床流行病学资料")
7
中国 北京- 18.2-27.8 /10 万( 95-99 年) 上海- 16.2-36.7/10 万( 85-03 年) 香港- 25.4/ 10 万 (89-94 年) 台湾- 24.8 / 10 万 (86 年) 亚裔人种发病率较高
 上海- /10 万( 年) 香港- 25.4/ 10 万 (89-94 年) 台湾- 24.8 / 10 万 (86 年) 亚裔人种发病率较高")
8
年龄: 约 80 %病例 < 5 岁 About 80% cases are < 5 years old 性别: 男 : 女之比 1:1.5-1.7 Boys outnumber girls by 1:1.5-1.7

9
流行病学资料 (2) 发病有一定的家庭集聚现象 兄弟姐妹、双胎发病率相对较高 提示:有遗传倾向与致病或环境因素相互作用 Higher rates of KD in the siblings and twins suggest a possible role for genetic predisposition that interacts with exposure to the etiologic agent or agents in the environments
 发病有一定的家庭集聚现象 兄弟姐妹、双胎发病率相对较高 提示:有遗传倾向与致病或环境因素相互作用 Higher rates of KD in the siblings and twins suggest a possible role for genetic predisposition that interacts with exposure to the etiologic agent or agents in the environments")
10
流行病学资料 (3) 季节:冬春季发病居多 More common in winter and early spring months 流行趋势:呈一定的区域流行 Occurring in both endemic and community-wide epidemic forms
 季节:冬春季发病居多 More common in winter and early spring months 流行趋势:呈一定的区域流行 Occurring in both endemic and community-wide epidemic forms")
11
冠状动脉瘤或扩张发生率 : 15%-25% Coronary artery aneurysms or ectasia develop in 15%-25% of untreated cases 住院病死率 : 约 0.17% In-hospital mortality rate is about 0.17% 再发率 : 1-3% Recurrence rate is reported to be 1-3%

12
病 因 Etiology 病因仍不明确 The etiology of KD remains unknown 临床和流行病学资料提示感染是可能的病因 或触发因子 Clinical and epidemiological features suggest infection is etiology or trigger

13
细菌毒素:超抗原学说 Bacterial toxin: There is a hypothesis that KD is related with superantigen 可能与免疫异常有关 It is possible that KD results from an immunologic response triggered by some microbial agents

14
病 理 Pathology 全身性血管炎 Generalised systemic vasculitis involving blood vessels throughout body. 动脉瘤形成 Aneurysms occurring in arteries

16
病理(续) 动脉重塑 狭窄 Arteial remodeling Stenosis
 动脉重塑 狭窄 Arteial remodeling Stenosis")
17
MCLS 全身小 动脉血管炎 肱 A 、髂 A(2%) 肾 A (1%) 肾性 高血压 肠系膜 A ( < 1%) 肠梗阻休克 破裂 脑血管 肺A肺A 肺 A 高压 肺梗塞 视力障碍 脑梗塞
 肾 A (1%) 肾性 高血压 肠系膜 A ( < 1%) 肠梗阻休克 破裂 脑血管 肺A肺A 肺 A 高压 肺梗塞 视力障碍 脑梗塞")
18
川崎病心血管相关病变的病理分期 ( 1 ) 分期病程特征性病理改 变 死因 I期I期 1-9 日 小血管炎,较大 的冠状动脉急性 心内膜炎及周围 血管炎,全心炎 心力衰竭及心 律失常 II 期 12-25 日 较大的冠状动脉 炎,冠状动脉瘤 及血栓栓塞,冠 状动脉内膜增生 ,全心炎 同 I+ 心梗,冠 状动脉瘤破裂
 分期病程特征性病理改 变 死因 I期I期 1-9 日 小血管炎,较大 的冠状动脉急性 心内膜炎及周围 血管炎,全心炎 心力衰竭及心 律失常 II 期 日 较大的冠状动脉 炎,冠状动脉瘤 及血栓栓塞,冠 状动脉内膜增生 ,全心炎 同 I+ 心梗,冠 状动脉瘤破裂")
19
川崎病心血管相关病变的病理分期( 2 ) 分期 病程特征性病理改变 死因 III 期 28-31 日 冠状动脉肉芽增生, 血管内膜增厚,小血 管炎消失 心梗 IV 期数月 - 数年 较大的冠状动脉疤痕 形成狭窄,钙化及血 管再通,心内膜及心 肌纤维化 心梗
 分期 病程特征性病理改变 死因 III 期 日 冠状动脉肉芽增生, 血管内膜增厚,小血 管炎消失 心梗 IV 期数月 - 数年 较大的冠状动脉疤痕 形成狭窄,钙化及血 管再通,心内膜及心 肌纤维化 心梗")
20
临床表现 Clinical Findings

21
发热持续 5 天以上 Fever persisting at least 5 days +

22
双侧球结膜充血, 无渗出物 Bilateral nonexudative conjunctivitis

23
周围肢体变化 : Changes in extremities : 初期:掌跖红斑、手足硬肿 Acute:Erythema of palms,soles;edema of hands,feet

24
恢复期:病程 2-3 周指、趾膜状脱皮 Subacute: Periungual peeling of fingers,toes in weeks 2 and 3

25
常见红斑性、斑丘疹样 皮疹, 躯干为主 The erythematousrash or maculopapular eruption is common,mainly with involvement of the trunk

26
口唇及口腔改变 : Changes of the lips and oral cavity: 口唇干裂、剥脱、出血 Dryness,fissuring,peeling and bleeding of the lips

27
草莓舌 “Strawberry tongue”

28
颈部淋巴结肿大 Cervical lymphadenopathy 单侧性、非化脓性 直径 >1.5cm Unilateral Non-suppurative Diameter>1.5cm

29
肛周及会阴部变化

30
其它表现 Other clinical findings 心血管系统:心肌炎、心包炎、心律失常、心衰 Cardiovascular system: myocarditis, pericarditis, arrythmia, heart failure 消化系统:腹痛、腹泻、肝功能损害 Gastrointestinal tract: abdominal pain, diarrhea, hepatic dysfunction 泌尿生殖系统:尿道炎 Genitourinary system: urethritis

31
其它表现 ( 续) Other clinical findings ( continued) 中枢神经系统:易激惹,无菌性脑膜炎 Central nervous system: extreme irritability, aseptic meningitis 肌肉骨骼系统:关节炎、关节痛 Musculoskeletal system: Arthritis, arthralgia
 Other clinical findings ( continued) 中枢神经系统:易激惹,无菌性脑膜炎 Central nervous system: extreme irritability, aseptic meningitis 肌肉骨骼系统:关节炎、关节痛 Musculoskeletal system: Arthritis, arthralgia")
32
实验室检查 Laboratory findings 白细胞计数增高,粒细胞为主 Leukocytosis with neutrophilia 血沉增快 Elevated erythrocyte sedimentation rate (ESR) C 反应蛋白增高 Elevated C- reactive protein (CRP) 血小板计数增高 Thrombocytosis
 C 反应蛋白增高 Elevated C- reactive protein (CRP) 血小板计数增高 Thrombocytosis")
33
实验室检查 Laboratory findings 贫血,低白蛋白血症 Anemia, Hypoalbuminemia 血清转氨酶增高 Elevated serum transaminases 血清 IgG,IgM,IgA,IgE, 循环免疫复合物增高 Elevated serum IgG,IgM,IgA,IgE and CIC

34
心电图 Electrocardiogram 窦性心动过速, S-T 段抬高,T 波倒置及 异常的 Q 波 Sinus tachycardia, elevated S-T segment 超声心动图 Echocardiogram 心包积液 , 瓣膜反流 Pericardial effusion, valvular regurgitation

35
冠状动脉瘤(扩张) Coronary aneurysm (ectasia)
 Coronary aneurysm (ectasia)")
36
冠状动脉造影 Coronary angiogram A BC

37
?

38
临床诊断标准 Clinical criteria for diagnosis A. 不明原因发热 5 天以上 Fever with unknown reasons persisting 5 + days B. 其它主要临床表现 Other principal clinical features 1. 周围肢体变化: Changes in extremities: a. 掌跖红斑,手足硬肿 Erythema of palms,soles;edema of hands, feet b. 指、趾膜状脱皮 Periungual peeling of fingers, toes

39
临床诊断标准 Clinical criteria for diagnosis 2. 多形性皮疹 Polymorphous exanthem 3. 双眼球结膜充血(无渗出) Bilateral bulbar conjunctival injection(without exudate) 4. 口唇潮红、皲裂、草莓舌、口咽粘膜充血 Erythema,dryness,cracking(,bleeding) of the lips; strawberry tongue; diffuse injection of oral and pharyngeal mucosae
 Bilateral bulbar conjunctival injection(without exudate) 4. 口唇潮红、皲裂、草莓舌、口咽粘膜充血 Erythema,dryness,cracking(,bleeding) of the lips; strawberry tongue; diffuse injection of oral and pharyngeal mucosae.")
40
临床诊断标准 Clinical criteria for diagnosis 5. 非化脓性颈部淋巴结肿大 ( 常为单侧) Cervical lymphadenopathy without suppuration 诊断: 1. 发热 + 其它至少四项主要标准 Diagnosis bsaed on > 5 days fever and at least 4 principal criteria 或 2. 发热 + 四项以下主要标准+冠脉病变 > 5 days fever and < 4 principal criteria when coronary artery abnormalities are detected
 Cervical lymphadenopathy without suppuration 诊断: 1. 发热 + 其它至少四项主要标准 Diagnosis bsaed on > 5 days fever and at least 4 principal criteria 或 2. 发热 + 四项以下主要标准+冠脉病变 > 5 days fever and < 4 principal criteria when coronary artery abnormalities are detected.")
41
l 鉴别诊断 Differential diagnosis 败血症 Septicemia 猩红热 Scarlet fever 全身型幼年类风湿关节炎 Syetemic juvenile rheumatoid arthritis 渗出性多形红斑 Exudative polymorphous erythema

42
治疗 Treatment 一. 控制炎症 Anti-inflammation 1. 阿司匹林 Aspirin 30-50mg/kg.d 每日 2-3 次 ,具抗炎、抗血小 板作用 With activities of anti-inflammation and anti-platelet 不能降低冠脉病变的发生 Not lowering the frequency of the development coronary abnormalities

43
关于阿司匹林使用的疗程 Duration of Aspirin administration 满 14 天,热退后 2-3 天逐渐减量至 3-5mg/kg.d (High dose) redused to 3-5mg/kg.d after 14 days of illness and the child has been afebrile for 48-72 hrs a. 无冠脉病变,维持 6-8 周 maintained for 6-8 weeks if no coronary abnormalities detacted

44
b. 有冠脉病变,维持至恢复 Continued indefinitely till recover 注意 瑞氏(肝脑脂肪变性)综合征 Reye syndrome 消化道不良反应
综合征 Reye syndrome 消化道不良反应")
45
2. 丙种球蛋白静脉滴注 IVIG 2g/kg.d 一次静脉滴注 8-12 小时 2g/kg.d in a single infusion for 8-12hrs 与阿司匹林合用 Together with aspirin 病程 10 天内使用(若可能, 7 天内使用) Started within first 10 days of illness. (If possible, within 7 days of illness)
 Started within first 10 days of illness. (If possible, within 7 days of illness).")
46
3. 皮质激素 Steroids 一般不用于初治, 剂量 2mg/kg.d ,用药 2-4 周 Not used for the initial treatment of KD 对冠脉病变的疗效不确切 The effects on coronary artery abnormalities still uncertain 与静脉丙球和阿司匹林合用, 或用于 Used to combind with IVIG and aspirin or 初治失败的病例 To the cases failed to respond to initial therapy

47
二. 抗血小板、抗凝治疗 Anti-platelet and anticoagulant therapy 双嘧达莫 ( 潘生丁 ) Dipyridamole (Persantin) 华法林 Warfarin 低分子肝素 Low-molecular-weight heparin 三. 对症治疗 Symptomatic treatment
 Dipyridamole (Persantin) 华法林 Warfarin 低分子肝素 Low-molecular-weight heparin 三. 对症治疗 Symptomatic treatment.")
48
并发冠状动脉瘤的危险因素 Risk factors for coronary aneurysms 男孩 Male sex 年龄 3 岁 Age >6 months or >3 yrs 发热持续 2 周以上 Fever more than 2 wks 血沉 > 100mm/h ESR>100mm/h 血红蛋白 <80g/L Hemoglobin<80g/L 白细胞 >16x10 9 /L WBC>16x10 9 /L

49
长期随访 Long-term follow-up 无冠脉病变者 出院 1 、 3 、 6 、 12 月随访 有冠脉病变者 在上述基础上每 6-12 个月随访,直至消失

Similar presentations




 解春红.>")
. 急性发热,皮肤粘膜病损和淋巴结肿大 为特点的血管炎综合征。又称皮肤粘膜淋 巴结综合征。常累及心血管系统,是儿童 期缺血性心脏病的主要原因 50% 在 2y 内发病,80% 病例在 5y 内 四季均可发病,4-5 月份和 11-1 月份 发 病相对较多.>")

 Mucocutaneous Lymphnode Syndrome(MCLS) Kawasaki disease 上海交通大学医学院附属新华医院 陈笋.>")



 病理生理学系 Department of Pathophysiology 高远生.>")
.>")


 重庆医科大学附属第二医院 熊正爱.>")
 重庆医科大学 儿科学院 刘恩梅.>")



![[病例1] 患者A,女,38岁,工人,头晕,乏力半年,加重一周,月经量多,否认胃病史。PE:贫血貌,睑结膜苍白,浅表淋巴结未及。B100d~Rt:WBC7.0×109/L N72%,RBC4.5×1012/L,HB72g/L,MCV60fl,MCHC32%,PLT109×109/L [病例2] 患者B,男,18岁,学生,乏力,牙龈渗血伴发热一周。既往无特殊病史。PE,T38.5℃,贫血貌,皮肤结膜苍白。胸骨无叩痛,肝脾肋下未及。B100d~Rt,WBC1.2×109/L,N20%,L75%,N0.24×1](/60/11239239/big_thumb.jpg "[病例1] 患者A,女,38岁,工人,头晕,乏力半年,加重一周,月经量多,否认胃病史。PE:贫血貌,睑结膜苍白,浅表淋巴结未及。B100d~Rt:WBC7.0×109/L N72%,RBC4.5×1012/L,HB72g/L,MCV60fl,MCHC32%,PLT109×109/L [病例2] 患者B,男,18岁,学生,乏力,牙龈渗血伴发热一周。既往无特殊病史。PE,T38.5℃,贫血貌,皮肤结膜苍白。胸骨无叩痛,肝脾肋下未及。B100d~Rt,WBC1.2×109/L,N20%,L75%,N0.24×1>")