Download presentation
Presentation is loading. Please wait.

1
常見的身心科疾病 佛教新店慈濟醫院 身心醫學科 王耀賢 醫師

2
憂鬱症

3
肝若不好,人生是黑白的 心情若不好,人生是‥?

4
心情若不好,人生是 黑色的

5
彩色的人生

6
憂鬱症有那幾種? 重度憂鬱症 情緒低落症(輕度憂鬱症) 喪親反應 環境適應障礙併有憂鬱症狀
 喪親反應 環境適應障礙併有憂鬱症狀")
7
憂鬱症 憂鬱症的 “七” 律 每七位憂鬱症有一人自殺身亡 自殺者有70%患有憂鬱症 自殺者有70%在六週內尋求家庭醫師
自殺是美國的第七大死因

8
憂鬱症對生活品質之影響 “憂鬱症患者因其憂鬱症狀而導至之各 方面功能減退 …對患者之影響不亞於 甚至超過五個主要慢性疾病所造成之
影響: 糖尿病、心血管疾病、肺部疾 病、背部疾病、關節炎‧‧“ Wells KB, et al. JAMA 1989 (本張對醫師和藥局都一樣之演講內容) 過去社會一般大眾都知道的慢性的身體疾病,像是心血管疾病、糖尿病等等,這些疾病對病患個體都有極大程度的影響,可是,過去社會一般大眾比較少想到,憂鬱症的症狀對病人也會產生相當程度的影響,這個是根據美國的統計,憂鬱症對於病患在身體功能的影響,社交功能的影響,及對整體健康情形的影響,都不亞於一般慢性常見的疾病,例如,糖尿病,心血管疾病、肺部疾病或是關節炎,我們可以看到憂鬱症對於個體的影響都是相當大的,所以就病患個體來講,儘早將憂鬱症的症狀治療緩解,是有其必要性的。
 過去社會一般大眾都知道的慢性的身體疾病,像是心血管疾病、糖尿病等等,這些疾病對病患個體都有極大程度的影響,可是,過去社會一般大眾比較少想到,憂鬱症的症狀對病人也會產生相當程度的影響,這個是根據美國的統計,憂鬱症對於病患在身體功能的影響,社交功能的影響,及對整體健康情形的影響,都不亞於一般慢性常見的疾病,例如,糖尿病,心血管疾病、肺部疾病或是關節炎,我們可以看到憂鬱症對於個體的影響都是相當大的,所以就病患個體來講,儘早將憂鬱症的症狀治療緩解,是有其必要性的。")
9
憂鬱症經濟學層面之考量 總成本: 美金437億 (美國,1990)
生產力失去或降低 自殺 門診診療 藥物成本 住院診療 Greenberg PE et al. J Clin Psychiatry. 1993; 54:405

10
憂鬱症病人自殺的危險性 約有一半以上的重度憂鬱症病人企圖自殺過 約有15%以上的重度憂鬱症病人是死於自殺
參與研究的SSRIs包括fluoxetine,paroxetine,fluvoxamine。

11
盛行率

12
憂鬱症之流行病學 憂鬱症之終生流行率為: 17.1% (美國) 男性: 約 13% 女性: 約 22%
男性: 約 13% 女性: 約 22% (本張只對藥局:) 在流行病學呢,根據美國的資料憂鬱症的終身流行率,大約是 17%,其中男性大約是 13%,女性大約是 22%,所以女性大約是男性的兩倍 Kessler RC et al, Arch Gen Psychiatry, 1994, Weissman MM, et5 al JAMA. 1996
 在流行病學呢,根據美國的資料憂鬱症的終身流行率,大約是 17%,其中男性大約是 13%,女性大約是 22%,所以女性大約是男性的兩倍. Kessler RC et al, Arch Gen Psychiatry, 1994, Weissman MM, et5 al JAMA")
13
那些人容易得到憂鬱症? 危險因子 關聯性 性別 女性是男性的兩倍 年齡 好發的年紀是 20–40 歲 家族史 有1.5到 3.0倍的危險
危險因子 關聯性 性別 女性是男性的兩倍 年齡 好發的年紀是 20–40 歲 家族史 有1.5到 3.0倍的危險 婚姻狀況 分居、寡居、離婚者的 危險性較高 已婚男性較未婚男性的危險性更低 已婚女性較未婚女性的危險性更高 Major depression is approximately twice as common in women, regardless of race1 Current major depression is more likely among persons younger than 45 years than in those 45 to 54 years of age1 Evidence exists that depression may have a familial pattern Separated, widowed, or divorced persons are at higher risk for major depression.1 Interestingly, some studies have found that married females have higher rates of depression than never-married females2 References: 1. Blazer DG, Kessler RC, McGonagle KA, Swartz MS. The prevalence and distribution of major depression in a national community sample: the national comorbidity survey. Am J Psychiatry. 1994;151: Stahl SM. Depression. In: Stahl SM. Essential Psychopharmacology: Neuroscientific Basis and Practical Applications. New York, NY: Cambridge University Press; 2000. Blazer et al. Am J Psychiatry Stahl. Essential Psychopharmacology

14
症狀

15
憂鬱症的常見症狀 生理性症狀 精神性症狀 食慾或體重異常改變 失眠或嗜睡 思考行動躁動不安或思考行動遲緩呆滯 疲倦 憂鬱或低落的情緒
對事物失去興趣 覺得無存在的價值或有罪惡感 思考能力、注意力或決斷力降低 反覆想到死亡或自殺 (對醫師:) 根據美國精神醫學會所制定的診斷統計手冊第四版,憂鬱症的症狀分成九大項,其中四大項是屬於身體方面的症狀,五大項是屬於心理方面的症狀。 (對藥局:) 生理方面的症狀,包括了食慾或體重異常的改變,有些病患會食慾特別異常的增加,有些病患是完全的沒有食慾,有些病患是體重異常的增加,有些病患是異常的減輕,另外,在睡眠方面,有些病患有可能是失眠,有些病患有可能是嗜眠,行為表現上有可能是精神運動性的激昂,非常的躁動性,也有可能是遲滯性,他的行為及思考各方面都非常的遲緩,病患有可能會非常的疲倦。 在心理方面的症狀,病患有可能有極度低落的情緒,病患有可能會對事物失去興趣,或失去喜樂感,另外有可能會有毫無價值的感覺或是有罪惡感,他的思考力,有可能會降低,注意力難以集中,非常難以做決定,另外病患有可能反覆的想到死亡,或者是自殺,在這九大項的症狀裏,如果說有其中的五大項症狀持續了兩週以上,而且持續了兩週以上的症狀包括了極度低落的情緒,或者是對事物失去興趣,這其中一項的話,就符合了美國精神醫學會所制定的重鬱症的診斷依據。 Must include one of these. DSM-IV, Washington, DC: American Psychiatric Association, 1994
 根據美國精神醫學會所制定的診斷統計手冊第四版,憂鬱症的症狀分成九大項,其中四大項是屬於身體方面的症狀,五大項是屬於心理方面的症狀。 (對藥局:) 生理方面的症狀,包括了食慾或體重異常的改變,有些病患會食慾特別異常的增加,有些病患是完全的沒有食慾,有些病患是體重異常的增加,有些病患是異常的減輕,另外,在睡眠方面,有些病患有可能是失眠,有些病患有可能是嗜眠,行為表現上有可能是精神運動性的激昂,非常的躁動性,也有可能是遲滯性,他的行為及思考各方面都非常的遲緩,病患有可能會非常的疲倦。 在心理方面的症狀,病患有可能有極度低落的情緒,病患有可能會對事物失去興趣,或失去喜樂感,另外有可能會有毫無價值的感覺或是有罪惡感,他的思考力,有可能會降低,注意力難以集中,非常難以做決定,另外病患有可能反覆的想到死亡,或者是自殺,在這九大項的症狀裏,如果說有其中的五大項症狀持續了兩週以上,而且持續了兩週以上的症狀包括了極度低落的情緒,或者是對事物失去興趣,這其中一項的話,就符合了美國精神醫學會所制定的重鬱症的診斷依據。 Must include one of these. DSM-IV, Washington, DC: American Psychiatric Association,")
16
常見的症狀-失去歡樂的感覺
17
常見的症狀-食慾問題

18
常見的症狀-體重減輕

19
常見的症狀-注意力不集中

20
常見的症狀-便袐

21
常見的症狀-疲勞

22
常見的症狀-很難下決定

23
常見的症狀-失眠

24
常見的症狀-失去興趣

25
常見的症狀-壓力大、焦燥

26
常見的症狀-胸口悶、呼吸困難

27
常見主訴症狀 身體性症狀: * 胸口悶,有如大石頭壓住 頭痛 疲累 隱約腹痛或關節痛 睡眠障礙 性功能異常 – 失去 “ 性 ” 趣
* 胸口悶,有如大石頭壓住 頭痛 疲累 隱約腹痛或關節痛 睡眠障礙 性功能異常 – 失去 “ 性 ” 趣 整天疲倦, 喃喃自語 DSM-IV, Washington, DC: American Psychiatric Association; 1994 AHCPR, Depression in Primary Care , Vol 1: 1993 (本張只對藥局:) 病患經常抱怨的症狀為以下幾項:頭痛、疲累、隱約腹痛或關節痛、 睡眠障礙、性功能異常、人際關係不良甚至、 整天疲倦,喃喃自語。 病患可能不一定會說出精神症狀因為: 記憶力減退、難以集中注意力、 覺得恥辱而不願承認或說明。
 病患經常抱怨的症狀為以下幾項:頭痛、疲累、隱約腹痛或關節痛、 睡眠障礙、性功能異常、人際關係不良甚至、 整天疲倦,喃喃自語。 病患可能不一定會說出精神症狀因為: 記憶力減退、難以集中注意力、 覺得恥辱而不願承認或說明。")
28
常見主訴症狀 心理及社會學的症狀: 精神不集中 (沒頭神) 健忘或變笨了、變白痴 頭腦亂糟糟 (亂七八糟) 人生沒有意思
健忘或變笨了、變白痴 頭腦亂糟糟 (亂七八糟) 人生沒有意思 缺乏動力,整天躺床又睡不著 人際關係不良 不想出門,不理人,不接電話 (本張只對藥局:) 病患經常抱怨的症狀為以下幾項:頭痛、疲累、隱約腹痛或關節痛、 睡眠障礙、性功能異常、人際關係不良甚至、 整天疲倦,喃喃自語。 病患可能不一定會說出精神症狀因為: 記憶力減退、難以集中注意力、 覺得恥辱而不願承認或說明。
 人生沒有意思. 缺乏動力,整天躺床又睡不著. 人際關係不良. 不想出門,不理人,不接電話. (本張只對藥局:) 病患經常抱怨的症狀為以下幾項:頭痛、疲累、隱約腹痛或關節痛、 睡眠障礙、性功能異常、人際關係不良甚至、 整天疲倦,喃喃自語。 病患可能不一定會說出精神症狀因為: 記憶力減退、難以集中注意力、 覺得恥辱而不願承認或說明。")
29
病因及病程

30
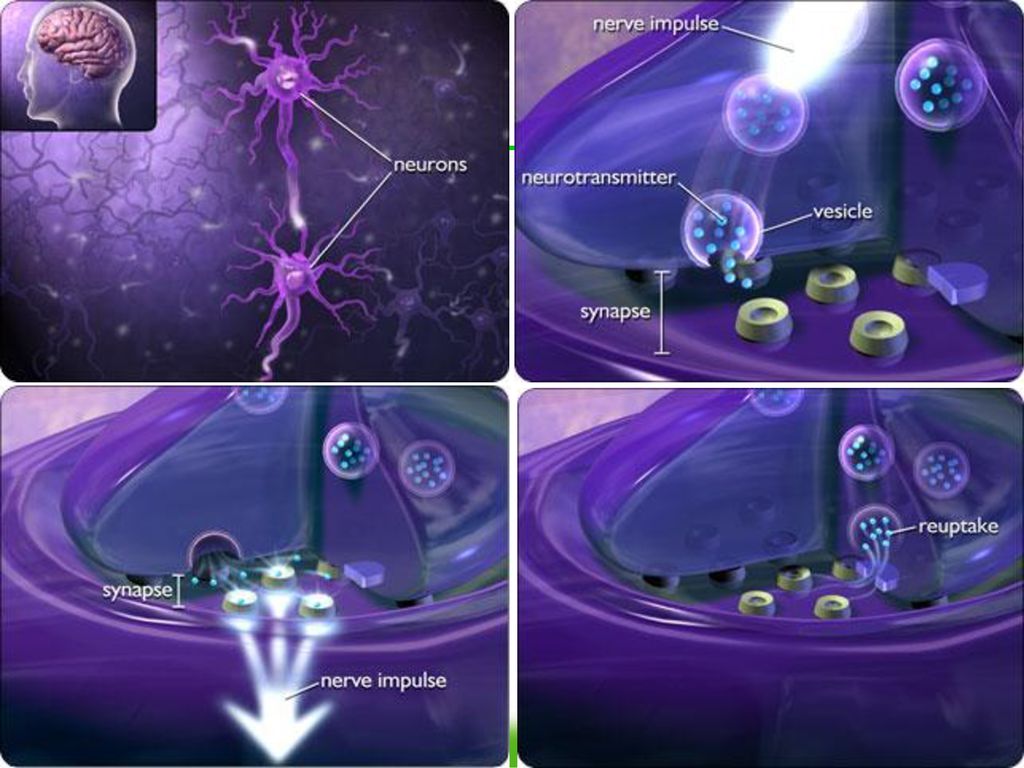
重憂鬱症的生病原因 先天不良 ─ 基因 後天失調 ─ 心理或社會壓力
先天不良 ─ 基因 後天失調 ─ 心理或社會壓力 Psychologic, biologic, and integrative models have been presented to explain the etiology of depression This slide illustrates the factors that may play a role in the etiology of depression1,2 Genetic factors, such as family history of depression Psychological and social factors, including psychosocial stressors Biochemical abnormalities, including an imbalance of neurotransmitters (norepinephrine, serotonin, and/or dopamine) Chronobiologic factors are not yet fully understood2 Psychiatric syndromes that are linked to disruption of circadian rhythms Seasonal affective disorder Premenstrual dysphoric disorder References: 1. Altemus M, Gold PW. Neurohormones in depression and anxiety. In: Schulkin J, ed. Hormonally Induced Changes in Mind and Brain. San Diego, Calif: Academic Press; McEachron DL, Schull J. Hormones, rhythms, and the blues. In: Schulkin J, ed. Hormonally Induced Changes in Mind and Brain. San Diego, Calif: Academic Press; 1993. Altemus et al. In: Schulkin. Hormonally Induced Changes in Mind and Brain McEachron et al. In: Schulkin. Hormonally Induced Changes in Mind and Brain
 Chronobiologic factors are not yet fully understood2. Psychiatric syndromes that are linked to disruption of circadian rhythms. Seasonal affective disorder. Premenstrual dysphoric disorder. References: 1. Altemus M, Gold PW. Neurohormones in depression and anxiety. In: Schulkin J, ed. Hormonally Induced Changes in Mind and Brain. San Diego, Calif: Academic Press; McEachron DL, Schull J. Hormones, rhythms, and the blues. In: Schulkin J, ed. Hormonally Induced Changes in Mind and Brain. San Diego, Calif: Academic Press; Altemus et al. In: Schulkin. Hormonally Induced Changes in Mind and Brain McEachron et al. In: Schulkin. Hormonally Induced Changes in Mind and Brain")
32
是因為想不開而出現憂鬱嗎? 其實是因為先得到憂鬱症而想不開的。 憂鬱症病患明知不應該想不開,但是就是沒有辦法不去想不開。
參與研究的SSRIs包括fluoxetine,paroxetine,fluvoxamine。

33
自殺 嚴重重鬱症患者中高達15%會死於自殺 憂鬱症患者自殺成功之危險因子包括: 男性 年齡小於 19 歲或是大於 45 歲
有慢性或嚴重身體疾病 本人或家屬中有藥物濫用者 (包括酒癮) 過去有過自殺病史 無助或絕望感 有精神病症狀 獨居、分居、寡居 (本張只對藥局:) 我們都知道,憂鬱症的患者有可能都會想到自殺,甚至嘗試自殺,其中嚴重的重鬱症患者,大約有 15% 會嘗試自殺,而他們自殺的成功危險因子,包括這幾大項,其中男性的危險因子比較高,因為他們的手段會比較激烈,另外年齡層特別低或是年齡層特別高的,他們如果嘗試自殺的話,也比較有可能會成功,因為他們的手段也是會比較激烈,另外本身是有慢性疾病,或是自己或家人有藥物濫用的情形,包括酒癮這些患者,也是屬於高危險群,另外就是過去有自殺病史的病患,還有極度絕望的病人,也是屬於高危險群,白種人比其他種族的人,也比較容易達到自殺成功的目的,另外就是他本身合併有精神性方面的症狀,還有就是獨居的憂鬱症患者,都是屬於比較高危險群,所以這些憂鬱症的患者,如果又有這些危險因子的話,他們提到要自殺的時候,我們都需要特別注意,因為如果他們一旦要自殺的話,往往較易成功。
 過去有過自殺病史. 無助或絕望感. 有精神病症狀. 獨居、分居、寡居. (本張只對藥局:) 我們都知道,憂鬱症的患者有可能都會想到自殺,甚至嘗試自殺,其中嚴重的重鬱症患者,大約有 15% 會嘗試自殺,而他們自殺的成功危險因子,包括這幾大項,其中男性的危險因子比較高,因為他們的手段會比較激烈,另外年齡層特別低或是年齡層特別高的,他們如果嘗試自殺的話,也比較有可能會成功,因為他們的手段也是會比較激烈,另外本身是有慢性疾病,或是自己或家人有藥物濫用的情形,包括酒癮這些患者,也是屬於高危險群,另外就是過去有自殺病史的病患,還有極度絕望的病人,也是屬於高危險群,白種人比其他種族的人,也比較容易達到自殺成功的目的,另外就是他本身合併有精神性方面的症狀,還有就是獨居的憂鬱症患者,都是屬於比較高危險群,所以這些憂鬱症的患者,如果又有這些危險因子的話,他們提到要自殺的時候,我們都需要特別注意,因為如果他們一旦要自殺的話,往往較易成功。")
34
何時最容易自殺? 當病情正在好轉時是比較容易出現自殺的時期
參與研究的SSRIs包括fluoxetine,paroxetine,fluvoxamine。

35
未治療之重度憂鬱症病程 正常 憂鬱 40% 復原 20% 變成輕度憂鬱或是部分復原 40%仍持續憂鬱 1 年
Most untreated episodes of depression last 6 to 24 months1 In two thirds of cases, symptoms remit completely1 In the remaining one third of cases1: 5% to 10% of untreated episodes last more than 2 years In 20% to 25% of cases, recovery is partial Studies of untreated depressed patients revealed that at 1-year follow-up2: Approximately 40% stay depressed 40% recover 20% either partly recover or develop the diagnosis of dysthymia, defined as a low-grade, chronic form of depression that lasts for more than 2 years References: 1. Depression Guideline Panel. Depression in Primary Care: Volume 1. Detection and Diagnosis. Clinical Practice Guideline, Number 5. Rockville, Md: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication ; April 1993: Stahl SM. Depression. In: Stahl SM. Essential Psychopharmacology: Neuroscientific Basis and Practical Applications. New York, NY: Cambridge University Press; 2000. 40%仍持續憂鬱 憂鬱 1 年 Stahl. Essential Psychopharmacology

36
重度憂鬱症復發的機率 大多數重度憂鬱症的病患終其一生都會至少有一次以上的復發 即便接受治療,重度憂鬱症的病患復發的機率依舊十分高
僅有過一次發作者,有50%的機率會復發 曾有過二次發作者,有70%的機率會復發 曾有過三次發作者,有90%的機率會復發 It is increasingly recognized that for most patients, major depression is a lifelong recurring disorder1 Most patients will have more than one episode of depression during their lifetime The risk that an additional episode will occur increases with successive episodes Approximately 50% of individuals who have had a single major depressive episode will experience a second episode, individuals who have had two episodes have a 70% chance of a third, and 90% who have experienced a third episode will develop a fourth2 References: 1. Kupfer DJ. Long-term treatment of depression. J Clin Psychiatry. 1991;52(suppl 5): American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994: Kupfer. J Clin Psychiatry APA Diagnostic and Statistical Manual of Mental Disorders
: American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994: Kupfer. J Clin Psychiatry APA Diagnostic and Statistical Manual of Mental Disorders")
37
治療

38
如何去治療呢? 不治療可以嗎? 抗憂鬱藥物治療 心理治療 輕度的可以不治療,但要冒可能惡化、自殺等風險 嚴重的一定要治療
對輕度憂鬱有效,療效與抗憂鬱藥物相當 單獨使用在中度或是重度憂鬱症效果不好,但是合併抗憂鬱藥物治療時可以有良好的反應 參與研究的SSRIs包括fluoxetine,paroxetine,fluvoxamine。

39
常用的憂鬱症治療藥物 百憂解 (Prozac) 克憂果 (Seroxat) 希普能 (Cipram) 樂復得 (Zoloft)
三環抗憂鬱劑 (TCA) 速悅 (Efexor) 樂活憂 (Remeron)
 速悅 (Efexor) 樂活憂 (Remeron)")
40
藥物治療的反應率 8 個星期 正常情緒 67% 反應良好 開始藥物 治療 33% 反應不佳 憂鬱情緒
接受藥物治療的憂鬱症病人,67%在治療八週後反應良好,但是仍然有33%治療無效 The majority of depressed patients respond favorably to treatment with antidepressants1 In two thirds of the cases, patients respond after 8 weeks of therapy. One third will not respond during that period of time Studies suggest that the treatment of depression should be vigorous and early1 The likelihood of a subsequent episode is increased in patients who achieve only a partial recovery Treatment should begin early in the episode, especially in patients with recurrent episodes of depression In general, the rate of response to antidepressant therapy, during a patient’s first episode of depression, is reported to be as high as 60%–70%; however, results in specific patients may vary2 References: 1. Stahl SM. Depression. In: Stahl SM. Essential Psychopharmacology: Neuroscientific Basis and Practical Applications. New York, NY: Cambridge University Press; American Psychiatric Association. Practice Guideline for Major Depressive Disorder in Adults. Washington, DC: American Psychiatric Association; 1993:10. 33% 反應不佳 憂鬱情緒 8 個星期 Stahl. Essential Psychopharmacology

41
常見的抗憂鬱藥物副作用 口乾、便袐 噁心、反胃、想吐 食慾不振或是增加 體重減少或增加 嗜睡或失眠 冒汗 性功能障礙

42
常見對抗憂鬱藥物的誤解 成癮 傷肝、傷腎 影響記憶力或是傷腦 很快見效 (其實多數需要二至六週才見效) 效果不好 長期使用可能有危險
不能與其他藥物併用

43
抗憂鬱藥物治療無效的常見原因 藥量不足、減量服用或是挑藥吃 只有心情不好時才吃 療效未出來即過早停服藥物 稍見效果即停用引起復發
因為感冒、腸胃炎之用藥而停用抗憂鬱藥物

44
憂鬱症病人是危險病人嗎? 沒有治療的憂鬱症病人是自殺的高危險病人 經過治療或是治療中的憂鬱症病人其自殺或是使用暴力的危險並不會比一般人高
包括自殺、帶家人或小孩去自殺 經過治療或是治療中的憂鬱症病人其自殺或是使用暴力的危險並不會比一般人高 參與研究的SSRIs包括fluoxetine,paroxetine,fluvoxamine。

45
如何協助憂鬱症病人 傾聽 陪伴 給予支持而非責難 協助病人正面思考 鼓勵病人接受專業治療 預防病人自殺

46
結論 憂鬱症是一個常見的疾病 憂鬱症會對生活帶來相當大的衝擊 憂鬱症是可以治療的 多數的自殺是可以預防的

47
Bipolar affective disorder
躁鬱症 Bipolar affective disorder 雙極性情感性疾病

48
Bi-Polar disorder

49
躁鬱症之流行病學(I) 終生盛行率: 1.2% 終生盛行率: 1.6% Epidemiological Catchment Study1
(3.3 million people in USA) Epidemiological Catchment Study1 終生盛行率: 1.6% (4 million people in USA) National Comorbidity Study2 1 Goodwin FK, Jamison KR, 1990 2 Kessler RC et al, 1994
 Epidemiological Catchment Study1. 終生盛行率: 1.6% (4 million people in USA) National Comorbidity Study2. 1 Goodwin FK, Jamison KR, Kessler RC et al,")
50
躁鬱症之流行病學 (II) 發病年齡: 男女分佈相同 SES: upper socioeconomic group
Wide range: teenager to 50 Mean: 30 y/o 男女分佈相同 SES: upper socioeconomic group 1 Goodwin FK, Jamison KR, 1990 2 Kessler RC et al, 1994

51
躁鬱症之致死率 至少 ¼ 嘗試自殺 約一半的躁鬱症混合型有自殺念頭
Goodwin FK, Jamison KR, 1990; Dilsaver SC et al, 1994

52
自殺的危險性比一般民眾高 15x 躁鬱症鬱期的自殺行為比躁期高出35x 1 GHarris and Barraclough, 1997
2 Dilsaver et al, 1997

53
PSYCHOTIC FEATURES

54
Manic Episodes 躁期之診斷 A. Duration more than 1 week (期間大於一星期)
B. Three (or more) of the following symptoms : 下列症狀大於 3 項或以上: (1) inflated self-esteem or grandiosity 自信心增高 (2) decreased need for sleep 睡眠需求減少 (3) more talkative than usual or pressure to keep talking 多話 (4) flight of ideas or subjective racing thoughts 跳躍性思考 (5) distractibility 易分心 (6) increase in goal-directed activity or psychomotor agitation 增加目的性行為或激躁不安 (7) excessive involvement in pleasurable activities that have a high potential for painful consequences 增加享樂性行為
 of the following symptoms : 下列症狀大於 3 項或以上: (1) inflated self-esteem or grandiosity 自信心增高. (2) decreased need for sleep 睡眠需求減少. (3) more talkative than usual or pressure to keep talking 多話. (4) flight of ideas or subjective racing thoughts 跳躍性思考. (5) distractibility 易分心. (6) increase in goal-directed activity or psychomotor agitation. 增加目的性行為或激躁不安. (7) excessive involvement in pleasurable activities that have a high potential for painful consequences 增加享樂性行為.")
55
Manic Episodes 躁期之診斷 C. Do not meet criteria for a mixed episode.
D. Cause marked impairment in occupational functioning or in usual social activities or relationships with others, or to necessitate hospitalization to prevent harm to self or others, or there are psychotic features. E. Not due to the direct physiological effects of a substance or a general medical condition (e.g., hyperthyroidism).
.")
56
Hypomanic Episode 輕躁期 Elevated or irritable mood lasting 4 days
Inflated self-esteem or grandiosity Decreased need for sleep More talkative Flight of ideas or racing thought Distractibility Increase in goal-directed activity or psychomotor agitation Excessive pleasurable activities Not cause marked functional impairment

57
Subtypes of MDP Bipolar I – Depression & Mania
Bipolar II – Depression & hypomania Bipolar III – Depression & family history of bipolar mood disorder

58
Bipolar Disorder 躁鬱症之特點
Common 常見的 Underdiagnosed 常未被診斷的 Delayed diagnosis - 8 years 診斷延遲 High suicide risk - 15% 高自殺危險性

59
Diagnosis and Recognition
US consumer survey: 60% untreated within 6 months of initial episode 35% do not seek treatment for 10 years 34% receive wrong diagnosis 50% unable to afford services

60
Recovery after first-episode mania Patients recovered (%)
通常臨床症狀緩解後功能尚未復原 Recovery after first-episode mania 100 80 60 40 20 Syndromal recovery: no longer meeting DSM-IV episode criteria Functional recovery: regaining baseline vocational and residential status Patients recovered (%) 這是一項為期2年的研究,追踪219位精神病性情感疾患患者(psychotic affective illness)在首次住院後症狀及功能恢復時間和比例. 症狀的恢復在第6,24個月,分別為83.7%和97.5%,通常病患症狀恢復較快的屬於30以上才發病,且少共病性,住院時間短且接受較少治療藥物的躁鬱症病患. 功能的恢復在第6,24個月,分別為30.4%和37.6%,比起症狀的恢復少了 倍;2年的追踪期發現63.1%的病患症狀已恢復但功能卻未達到恢復. 結論: 精神病性情感疾患患者在住院後大部份都能達到症狀恢復,但24個月後僅三分之一的病患能夠恢復功能,顯示這項常見疾患在首次發病及住院後,仍對病患功能有重大的影嚮. Syndromal Functional Tohen M et al. Am J Psychiatry 2000;157:220–8
 這是一項為期2年的研究,追踪219位精神病性情感疾患患者(psychotic affective illness)在首次住院後症狀及功能恢復時間和比例. 症狀的恢復在第6,24個月,分別為83.7%和97.5%,通常病患症狀恢復較快的屬於30以上才發病,且少共病性,住院時間短且接受較少治療藥物的躁鬱症病患. 功能的恢復在第6,24個月,分別為30.4%和37.6%,比起症狀的恢復少了 倍;2年的追踪期發現63.1%的病患症狀已恢復但功能卻未達到恢復. 結論: 精神病性情感疾患患者在住院後大部份都能達到症狀恢復,但24個月後僅三分之一的病患能夠恢復功能,顯示這項常見疾患在首次發病及住院後,仍對病患功能有重大的影嚮. Syndromal Functional. Tohen M et al. Am J Psychiatry 2000;157:220–8.")
61
躁鬱症自殺 一半的病患至少終其一生會有至少一次的嘗試自殺 1/5 死於自殺 躁鬱症自殺的危險因子 鬱期的嚴重程度 混合型躁鬱症
1/5 死於自殺 躁鬱症自殺的危險因子 鬱期的嚴重程度 混合型躁鬱症 合併有酒精濫用或酒精依賴 曾有自殺記錄 重要親友喪失 躁鬱症第二型

62
精神分裂症 Schizophrenia

63
精神分裂症之流行病學 終生盛行率: 1-1.5% 男女分佈相同 發病期 男性:15-25歲 女性:25-35 歲 50 歲後發病極少
發病期 男性:15-25歲 女性:25-35 歲 50 歲後發病極少 1 Goodwin FK, Jamison KR, 1990 2 Kessler RC et al, 1994

64
精神分裂症之診斷 I 至少一個月內大部分時間出現至少兩個以上之下列症狀: Delusion: 妄想 Hallucination: 幻覺
Diaorganized speech: (e.g. frequent derailment or incoherence) 混亂性話語 Grossly disorganized or catatonic behavior : 混亂性或僵直性行為 Negative symptoms (affective flattening, alogia or avolition) 負向症狀
 混亂性話語. Grossly disorganized or catatonic behavior : 混亂性或僵直性行為. Negative symptoms (affective flattening, alogia or avolition) 負向症狀.")
65
精神分裂症之診斷 II 其它診斷見條件: impairment in: work, interpersonal relationship, or self-care; marked below the level achieved prior to onset. Duration: Continuous signs of disturbance persist for at least 6 months, including prodromal phase, or in attenuated forms. Other exclusion criteria.

66
精神分裂症之典型的病程 青春期開始出現不明顯症狀
前驅病狀:evident in retrospective, weeks to months. 加速因子: 離家求學藥物濫用喪失親友 發病 第一次發病 逐漸恢復大部份功能 好好壞壞 常復發 前 5 年預測接下來復發 復發 功能逐漸喪失 ( DD mood disorder)
")
67
精神分裂症之預後 Only 10-20 % can be described as good outcome
50 % poor outcome: repeat hospitalization, exacerbation of symptoms, episodes of major depressive disorder, and suicide attempt. 20-30 %: able to lead somewhat normal lives.

68
精神分裂症之自殺 50% attempt suicide at least once in their life
10-15% die by suicide Risk factor: Depressive symptoms Young age High level of premorbid functioning ( especially a college education)
")
69
謝謝! 王耀賢 醫師

70
問題討論

Similar presentations

 資料整理:蔡淑慧 張瑋琪 楊施韻 湯智凱. 前言:現況 一、世界衛生組織 (WHO) ( 一 )1996 年 Today, there are an estimated 400 million people with anxiety disorders.>")





>")











