Download presentation
Presentation is loading. Please wait.

1
Approach to bleeding

2
Cellular elements of blood arise from hematopoietic stem cells in the bone marrow.
2

3
止血機制 1. Local Vascular Constriction:血管收縮減少血流量,且使得血流變慢。
Local reflex:完全不受中樞調控。 血管收縮物質: i. Angiotensin II:由Arterial wall 分泌。 ii. Serotonin、Thromboxane A2:由Platelet分泌。 檢測Platelet count 與bleeding time:判定凝血過程是否在此一階段出問題。

4
止血機制 2. Platelet-Vessel Wall Interaction:較慢的血流讓血小板有更高機率與曝露出來的
受損部位作接觸黏合,產生Hemostatic Plug。

5
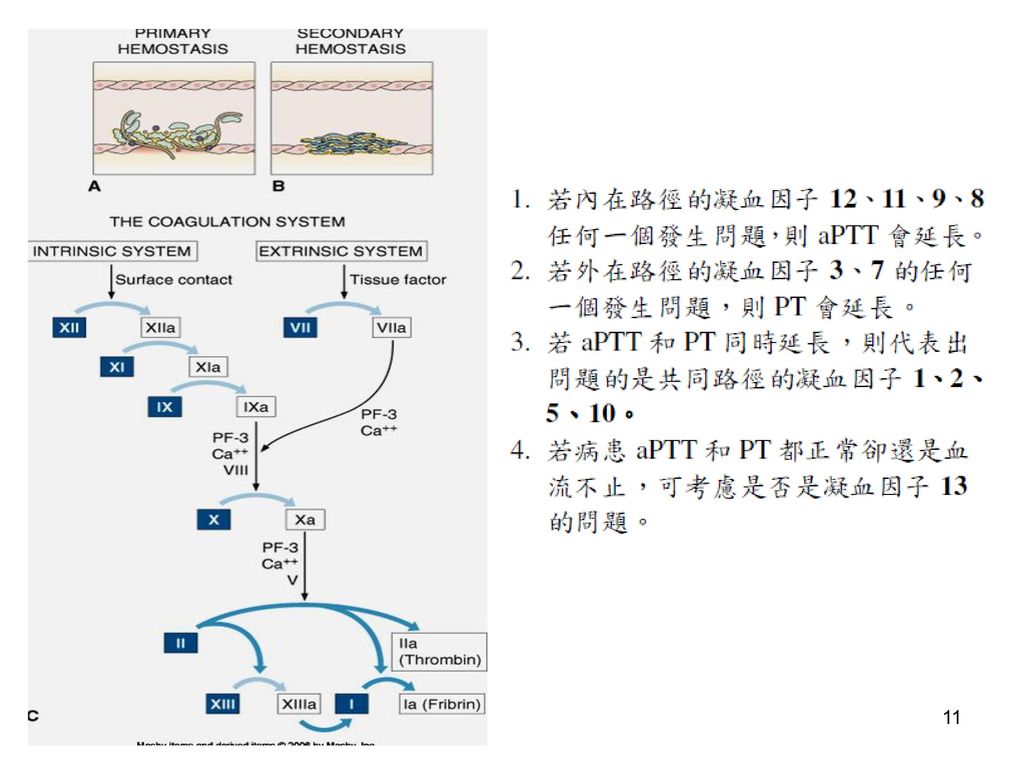
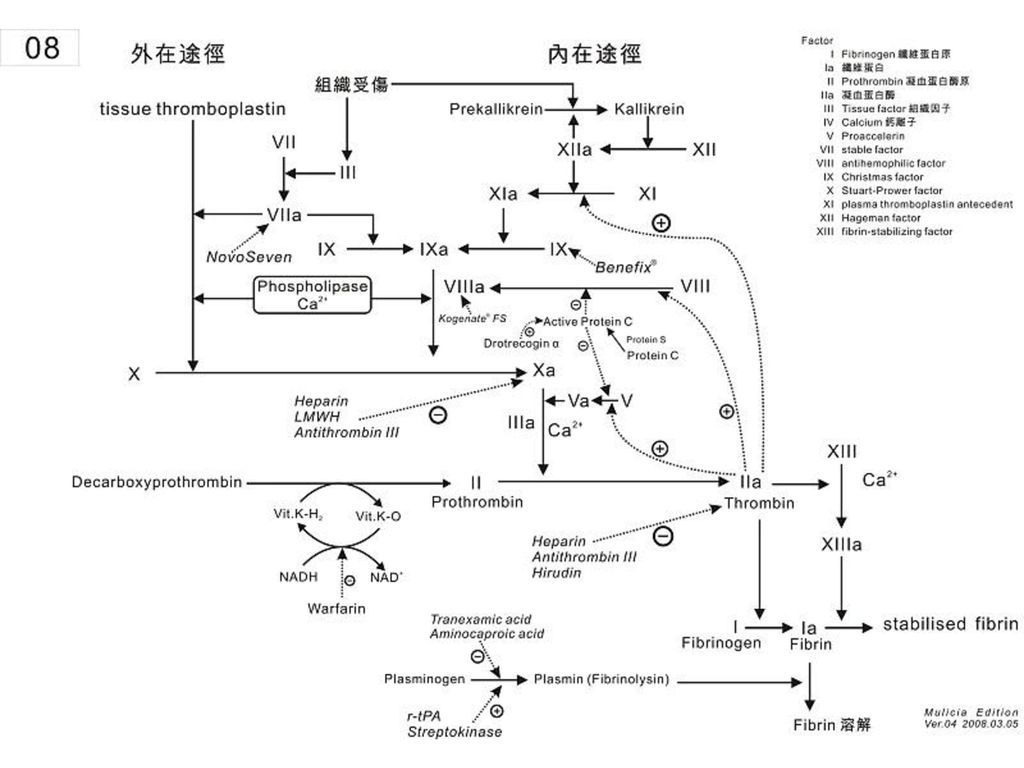
止血機制 3. Local Blood Coagulation:活化凝血的內外路徑(活化凝血因子),形成Fibrin Clot 而成功止血。
a. Intrinsic System: i. 啟動較慢:需要數秒到數分鐘的時間去活化此路徑。 ii. 活化因子:血液接觸到非血管內皮細胞表面。 b. Extrinsic System: i. 啟動迅速:立刻反應。 ii. 活化因子:Tissue factor(=凝血因子3) c. 檢測PT 與aPTT(activated Partial Thromboplastin Time):判定凝血過程中在內在途徑(主要以aPTT 來評估)或者外在途徑(主要以PT 來評估)是否異常。
 c. 檢測PT 與aPTT(activated Partial Thromboplastin Time):判定凝血過程中在內在途徑(主要以aPTT 來評估)或者外在途徑(主要以PT 來評估)是否異常。")
6
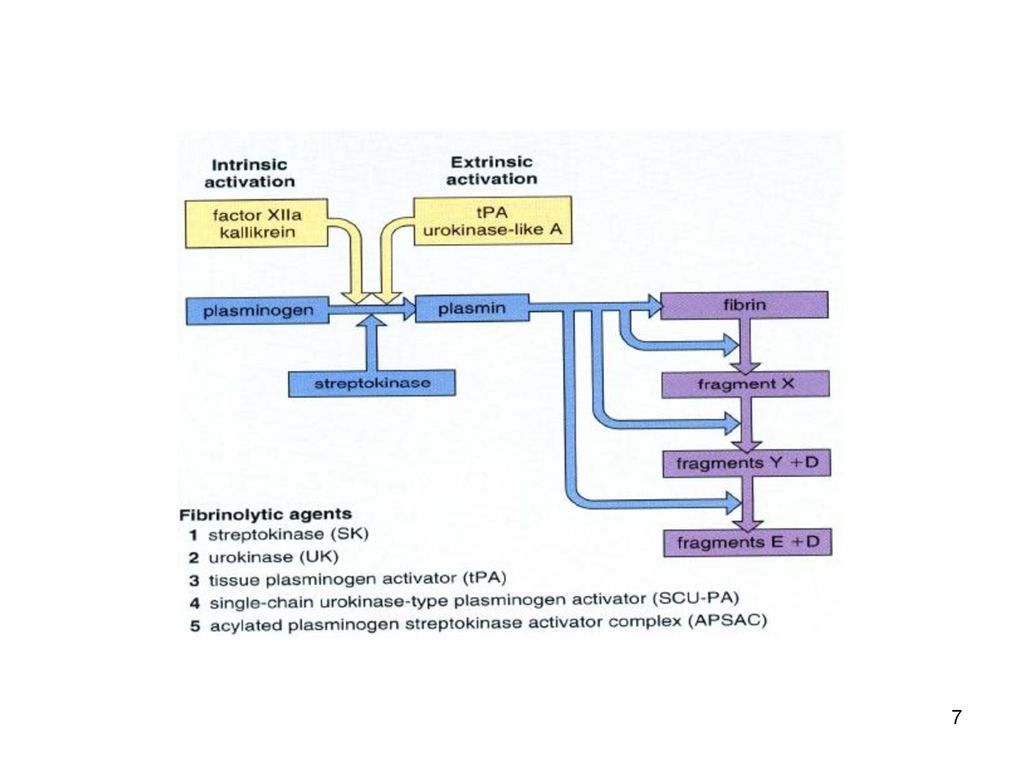
止血機制 4. Appropriate Fibrinolytic Activity:一段時間過後,啟動血塊溶解的機制→血塊被溶解而消失。
a. fibrin clot 的穩定:藉由凝血因子13(Fibrin-stabilizing factor)來加強其穩定度,避免fibrin clot 被強力血流沖刷掉。 b. 一旦凝血穩固後,就會同時並行fibrinolysis 機制 c. 血塊溶解的啟動是相當緩慢的(避免再度出血) d. 檢測Thrombin time、FDP、D-dimer 來判斷此一階段是否出錯。
來加強其穩定度,避免fibrin clot 被強力血流沖刷掉。 b. 一旦凝血穩固後,就會同時並行fibrinolysis 機制. c. 血塊溶解的啟動是相當緩慢的(避免再度出血) d. 檢測Thrombin time、FDP、D-dimer 來判斷此一階段是否出錯。")
10
因子 I, 纖維蛋白原 因子 II, 凝血素 因子 III, 凝血酶原酶 因子 IV, 鈣(Ca2+) 因子 因子 V, 促凝血球蛋白原,易變因子 因子 VII, 轉變加速因子前體,促凝血酶原激酶原,輔助促凝血酶原激酶 因子 VIII, 抗血友病球蛋白A (AHG A), 抗血友病因子A (AHFA),血小板 輔助因子 I, 血友病因子 VIII 或 A, 因子 IX, 抗血友病球蛋白B (AHG B),抗血友病因子B (AHF B),血友病 因子 IX 或 B 因子 X, STUART(-PROWER)-F, 自體凝血酶原C 因子 XI, ROSENTHAL因子,抗血友病球蛋白C 因子 XII, HAGEMAN因子, 表面因子 因子 XIII, 血纖維穩定因子
, 抗血友病因子A (AHFA),血小板. 輔助因子 I, 血友病因子 VIII 或 A, 因子 IX, 抗血友病球蛋白B (AHG B),抗血友病因子B (AHF B),血友病. 因子 IX 或 B. 因子 X, STUART(-PROWER)-F, 自體凝血酶原C. 因子 XI, ROSENTHAL因子,抗血友病球蛋白C. 因子 XII, HAGEMAN因子, 表面因子. 因子 XIII, 血纖維穩定因子.")
13
Vascular Disorders 血管管壁的問題最常見,不可以忽略這一 項的重要性,當遇到一個病人血流不止時應該擺在第一順位去討論。
1. Simple Easy Bruising:大撞擊力導致血管管壁破裂。 2. Senile Purpura:老年人的管壁組織脆弱,可能輕觸就會受損。 3. Vascular malformation; Hemangioma

14
Local tissue disorder Scar tissue Fragile tissue Granulation tissue
Tumor Infection Inflammation

15
Assessment of bleeding risk
Patient’s history+physical examination+screening hemostatic tests often provide a tentative diagnosis. Patients with a moderate to severe bleeding disorder invariably have recurrent bleeding.

16
Questions to detect an increased risk of bleeding
Have you ever had a nose bleed that lasted for 5 minutes or longer without reason? Have you ever had bruises (hematoma) on your body without trauma? Do you have bruises more than 1 to 2 times per week? Did you ever have bleeding of gums without apparent cause? Do you have the impression that you have prolonged bleeding after minor wounds? Have you had prolonged bleeding after or during an operation (tonsillectomy, appendectomy, or during delivery)? Did you have prolonged bleeding with a tooth extraction? Have you ever received a blood transfusion during an operation? Is there a history of bleeding disorders in your family? Do you take any aspirin, NSAIDs, or anticoagulants? Do you have the impression that you have prolonged menstruation (longer than 7 days) and/or a high frequency of tampon change?
 on your body without trauma Do you have bruises more than 1 to 2 times per week Did you ever have bleeding of gums without apparent cause Do you have the impression that you have prolonged bleeding after minor wounds Have you had prolonged bleeding after or during an operation (tonsillectomy, appendectomy, or during delivery) Did you have prolonged bleeding with a tooth extraction Have you ever received a blood transfusion during an operation Is there a history of bleeding disorders in your family Do you take any aspirin, NSAIDs, or anticoagulants Do you have the impression that you have prolonged menstruation (longer than 7 days) and/or a high frequency of tampon change")
17
Type of bleeding vs. Underlying cause
Hemarthroses and intramuscular hematomas: coagulation disorder (hemophilia) Mucocutaneous bleeding (epistaxis, gingival bleeding, or menorrhagia): platelet disorder or von Willebrand disease (VWD) Bleeding isolated to a single site (menorrhagia or hematuria): anatomic, infectious, or inflammatory
 Mucocutaneous bleeding (epistaxis, gingival bleeding, or menorrhagia): platelet disorder or von Willebrand disease (VWD) Bleeding isolated to a single site (menorrhagia or hematuria): anatomic, infectious, or inflammatory.")
18
Medication history Prescription medicines
Over-the-counter medications: aspirin, NSAIDs Herbal and alternative agents: Ginkgo (銀杏) 、Ginseng (人參) All supplemental agents and over-the-counter pain relievers (acetaminophen 除外) should be discontinued 2 weeks before an elective surgical procedure.
 、Ginseng (人參) All supplemental agents and over-the-counter pain relievers (acetaminophen 除外) should be discontinued 2 weeks before an elective surgical procedure.")
19
Objective confirmation of a bleeding disorder
Personal history and Family history: Prolonged surgical bleeding Previous treatment with RBC transfusions Anemia or treatment with iron Physical examination: Ecchymosis, petechiae, or persistent oozing from a venipuncture site

20
Screening laboratory tests
Patients without a known history of bleeding 5649 patients undergoing surgery, a negative bleeding history was found in 88.8% of the patients; this was confirmed by laboratory testing Testing is not needed when there is no history of abnormal bleeding.

21
Screening laboratory tests
Patients with a known history of bleeding or with a suspected bleeding disorder CBC: anemia and thrombocytopenia PT (prothrombin time) or INR aPTT (activated partial thromboplastin time) Platelet function: bleeding time test; PFA (platelet function analyzer) von Willebrand factor: 1.6% of the general population Hematology consultation: reproducible history of unexplained bleeding
 or INR. aPTT (activated partial thromboplastin time) Platelet function: bleeding time test; PFA (platelet function analyzer) von Willebrand factor: 1.6% of the general population. Hematology consultation: reproducible history of unexplained bleeding.")
22
Inherited Bleeding Disorders
Hemophilia A (Factor VIII的活性缺失) Hemophilia B (Factor IX的活性缺失) VWD 與vW factor 的不足或不正常有關。 vW factor 存於血管內皮細胞細胞質的Weibel-palade體內,被釋放到內皮下組織與血漿。血管內皮細胞受傷時,內皮下vWf會和platelets 結合,提高platelets的黏著性,封閉血管內皮傷口。血漿中,vWf會結合並保護factor VIII。缺乏vWf,會造成factor VIII的活性缺失。 外傷或外科手術後常出現大量出血 可利用FFP或冷沉澱物治療
 Hemophilia B (Factor IX的活性缺失) VWD. 與vW factor 的不足或不正常有關。 vW factor 存於血管內皮細胞細胞質的Weibel-palade體內,被釋放到內皮下組織與血漿。血管內皮細胞受傷時,內皮下vWf會和platelets 結合,提高platelets的黏著性,封閉血管內皮傷口。血漿中,vWf會結合並保護factor VIII。缺乏vWf,會造成factor VIII的活性缺失。 外傷或外科手術後常出現大量出血. 可利用FFP或冷沉澱物治療.")
23
Acquired Hemorrhagic Disorders
Liver disease: decreased synthesis of clotting factors, thrombocytopenia, DIC Renal disease: platelet dysfunction (The bleeding risk is lessened with dialysis and the use of DDAVP)
")
24
Thrombocytopenia: Definition: <150,000 cells/μL Surgical bleeding: <50,000 cells/μL Possible spontaneous bleeding: <20,000 cells/μL Spontaneous bleeding: <10,000 cells/μL

25
Thrombocytopenia Decrease in PLT production Altered PLT function
Peripheral destruction of PLT Sequestration of PLT in the spleen In patient with splenomegaly, PLT transfusions often do not produce an increase in the PLT count. Thrombocytopenia in the presence of normal RBC and WBC counts is typically caused by increased PLT destruction (autoimmune mechanism, e.g. ITP).
.")
26
Decreased production of platelets
Aplastic anemia: decreased production of megakaryocyte in bone marrow Infiltration diseases of bone marrow Drugs; Radiation; Viral infection Chemotherapy (most common)
")
27
Increased destruction of platelets
Idiopathic (Immune) thrombocytopenia purpura (ITP) Progenitor of megakaryocyte or platelets被自身抗體IgG破壞 Acute ITP: 會出現在感染病毒之後的兒童身上, 可能是病毒引發platelets抗原改變 Chronic ITP: 主要發生在成人身上,與collagen diseases (SLE)或lymphoma, leukemia 有關 治療: 藥物、脾切除
 thrombocytopenia purpura (ITP) Progenitor of megakaryocyte or platelets被自身抗體IgG破壞. Acute ITP: 會出現在感染病毒之後的兒童身上, 可能是病毒引發platelets抗原改變. Chronic ITP: 主要發生在成人身上,與collagen diseases (SLE)或lymphoma, leukemia 有關. 治療: 藥物、脾切除.")
28
Increased destruction of platelets
Drug-induced Thrombocytopenia Quinidine, sulfonamides, penicillin, β-lactam, digoxin 會與platelets表面蛋白質結合產生新的抗原,誘發抗體破壞platelets。 Heparin是引發thrombocytopenia 最普遍的藥物,會引影響約5%利用抗凝血劑治療的病患,停藥後會痊癒

29
Increased destruction of platelets
Thrombotic thrombocytopenic purpura (TTP) Platelets群集廣泛沉積在微血管,成為透明血栓 可能是受傷的血管內皮細胞不當釋放vW factor導致 也可能是auto-immune disease, drug-induced allergic reaction, infection, chemotherapy, pregnancy 併發症
 Platelets群集廣泛沉積在微血管,成為透明血栓. 可能是受傷的血管內皮細胞不當釋放vW factor導致. 也可能是auto-immune disease, drug-induced allergic reaction, infection, chemotherapy, pregnancy 併發症.")
31
Qualitative disorder of PLT
The most common cause of inhibited PLT function is drugs For patient with a bleeding disorder or an abnormal PLT function screen who are considering elective surgery, the first approach is to discontinue all unnecessary medications, including nutritional supplements and over-the-counter agents.

Similar presentations

血管壁的作用 (二)血小板的作用 (三)凝血因子的作用 (四)抗凝血系统的作用 (五)纤维蛋白溶解(纤溶)系统的作用 (六)血液流变学改变.>")
. 【定义】 出血性疾病是止血功能障碍所致 的自发性出血或损伤后出血不止为 主要表现的一组疾病,常表现为全 身多部位出血。 出血性疾病是止血功能障碍所致 的自发性出血或损伤后出血不止为 主要表现的一组疾病,常表现为全 身多部位出血。>")

是因机体止血或凝血功障 碍所引起,通常以全身性或局限性皮肤 粘膜自发性出血或损伤后难以止血为临 床特征。>")
 第三节 生理性止血 (Hemostasis) 基础医学院病理生理教研室.>")

 的制定及临床应用体会 北京朝阳医院 呼吸与危重症医学科 曹志新 2009-10-27.>")
 病理生理学系 Department of Pathophysiology 高远生.>")

 Disseminated Intravascular Coagulation>")







![[病例1] 患者A,女,38岁,工人,头晕,乏力半年,加重一周,月经量多,否认胃病史。PE:贫血貌,睑结膜苍白,浅表淋巴结未及。B100d~Rt:WBC7.0×109/L N72%,RBC4.5×1012/L,HB72g/L,MCV60fl,MCHC32%,PLT109×109/L [病例2] 患者B,男,18岁,学生,乏力,牙龈渗血伴发热一周。既往无特殊病史。PE,T38.5℃,贫血貌,皮肤结膜苍白。胸骨无叩痛,肝脾肋下未及。B100d~Rt,WBC1.2×109/L,N20%,L75%,N0.24×1](/60/11239239/big_thumb.jpg "[病例1] 患者A,女,38岁,工人,头晕,乏力半年,加重一周,月经量多,否认胃病史。PE:贫血貌,睑结膜苍白,浅表淋巴结未及。B100d~Rt:WBC7.0×109/L N72%,RBC4.5×1012/L,HB72g/L,MCV60fl,MCHC32%,PLT109×109/L [病例2] 患者B,男,18岁,学生,乏力,牙龈渗血伴发热一周。既往无特殊病史。PE,T38.5℃,贫血貌,皮肤结膜苍白。胸骨无叩痛,肝脾肋下未及。B100d~Rt,WBC1.2×109/L,N20%,L75%,N0.24×1>")
 河南中医学院第一附属医院 杜正光>")