Download presentation
Presentation is loading. Please wait.

1
常見腦血管疾病與腦部腫瘤 介紹與術後照顧 神經外科 戴世煌醫師

2
學習目標 了解常見腦血管疾病與不同分類的腦瘤 診斷及治療 術後照顧的注意重點

3
大綱 常見腦血管疾病 常見腦部腫瘤 術後照顧的注意重點 Q&A

5
How serious is hemorrhagic stroke in Taiwan?
About 73 per one hundred thousand occur each year 22% in all stroke 30 days mortality: 26-30% The first leading cause of serious long-term disability in adults Before my topic, let me show how serious is hemorrhagic stroke in Taiwan. Generally, there is 73 per patients in hemorrhagic stroke at Taiwan each year. Hemorrhagic type stroke accounts for 22% of all strokes a d is associated with higher mortality rate than cerebral infarctions. The 30 days morality rate is up to 30%. It is also the first leading cause of serious long-term disability in adults in Taiwan. Taiwan Guidelines for the Management of Stroke 2008

6
Taiwan Guidelines for the Management of Stroke 2008
The secondary leading cause of death Male: 4.67/1000 Female: 3.32/1000 Taiwan Guidelines for the Management of Stroke 2008

7
Cerebrovascular accidents(CVA)(腦中風)
15% hemorrhage 85% infarcts Risk factors: arteriosclerosis, DM, H/T, heavy smoking, fat, heart valve disease, vasculopathy, coagulopathy, peripartum

8
腦中風(stroke) 梗塞性中風(Infarction) 出血性中風(Hemorrhagic stroke)
Cerebral thrombosis (血管硬化,管腔狹窄後阻塞) Cerebral embolism (血管栓塞) Hemodynamic insufficiency (大血管狹窄使腦內血流不足引起腦組織缺血) Hypovolemic insufficiency (休克、心衰竭…等,引起腦組織缺血) 出血性中風(Hemorrhagic stroke) 腦出血 (intracerebral hemorrhage) 蜘蛛膜下腔出血 (Spontaneous subarachnoid hemorrhage,SAH)
 Cerebral embolism (血管栓塞) Hemodynamic insufficiency (大血管狹窄使腦內血流不足引起腦組織缺血) Hypovolemic insufficiency (休克、心衰竭…等,引起腦組織缺血) 出血性中風(Hemorrhagic stroke) 腦出血 (intracerebral hemorrhage) 蜘蛛膜下腔出血 (Spontaneous subarachnoid hemorrhage,SAH)")
9
致病因(Etiology) Hypertension
Acutely increased CBF, especially to area previously rendered ischemic Vascular anomalies Arteriopathies Coagulation disorder Infection Venous or dural sinus thrombosis Drug abuse Post-traumatic eclampsia

11
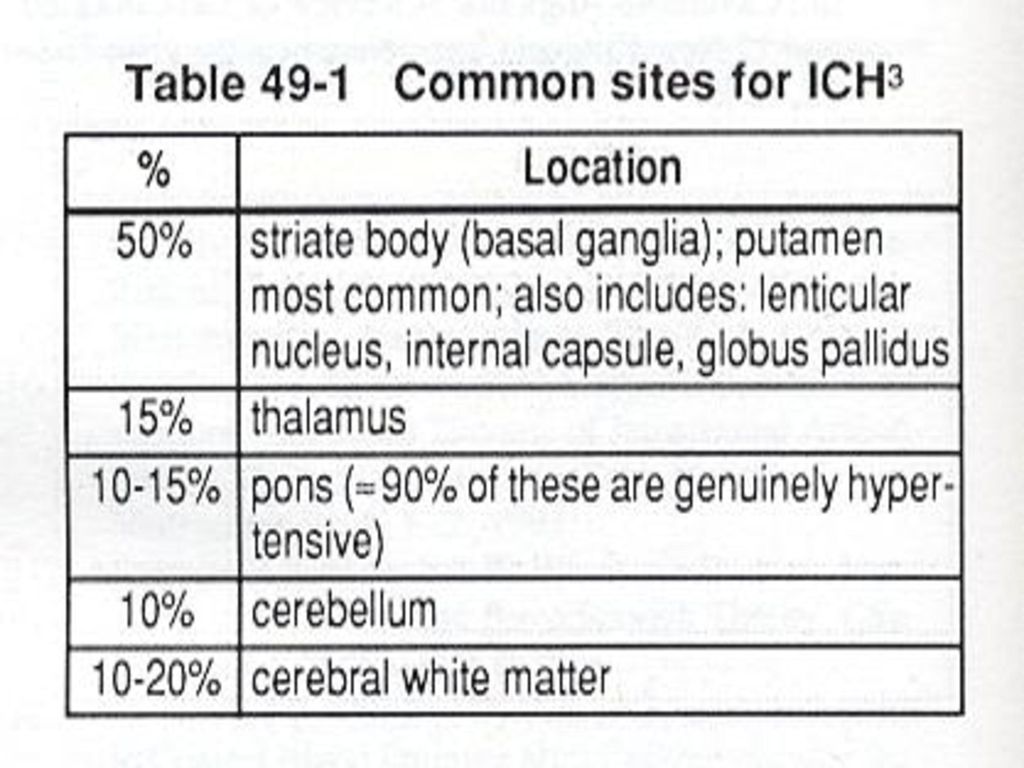
Intracranial hemorrhage
ICH in putamum and subcortical area 3cm, volume 20cc surgical decompression ICH in cerebellum 2cm, volume 10cc surgical consideration EVD or ICP monitor was considered in acute hemoventricle.

12
Putaminal hemorrhage

13
Thalamic hemorrhage

14
Cerebellar hemorrhage

15
Lobar hemorrhage

16
Subcortical hemorrhage

17
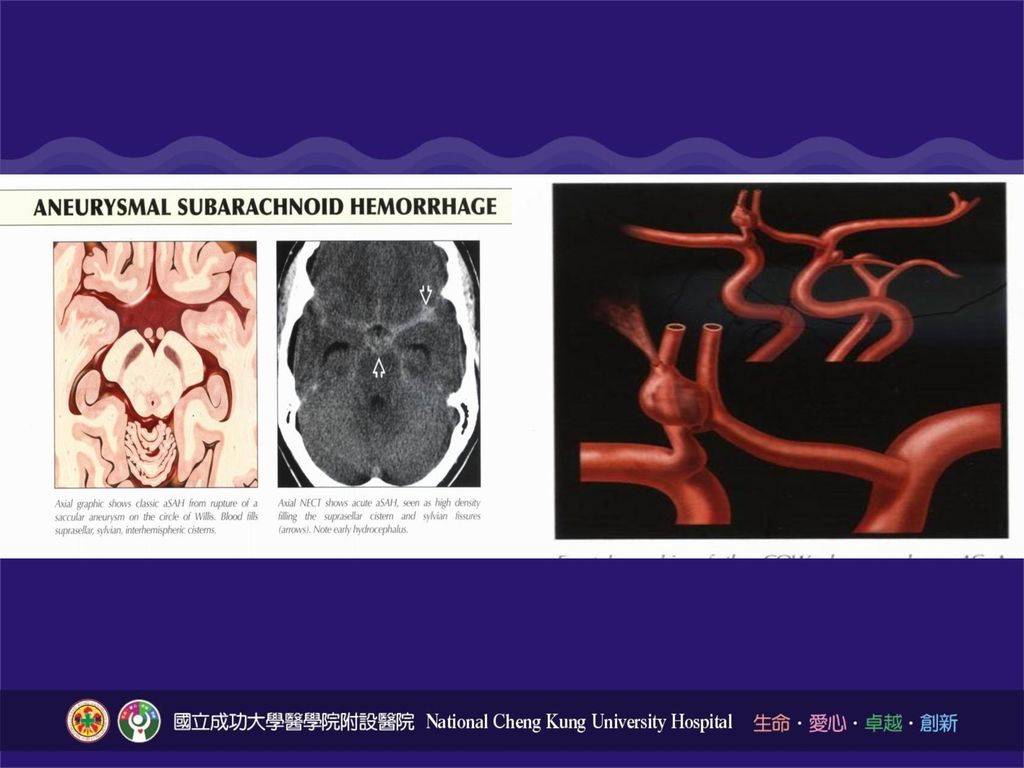
SAH (Ⅰ)(蜘蛛膜下腔出血) 80% caused by ruptured intracranial aneurysm
5% due to AVMS 10% unknown causes

18
臨床表現 劇烈頭痛, 噁心,昏倒..(Sudden onset of explore headache, usually with vomiting, syncope) 頸部僵硬(Nuchal rigidity) Kernig’s sign Brudzinski’s sign

19
檢查 病史(History) 理學及神經學檢查(PE and NE) 電腦斷層(CT scan) 電腦斷層血管攝影(CTA)
核磁共振(MRI) 核磁共振血管攝影(MRA) 大腦血管攝影(Cerebral angiography)
 核磁共振血管攝影(MRA) 大腦血管攝影(Cerebral angiography)")
20
SAH Conventional angiography CT angiography

21
Spontaneous SAH (Aneurysm Rupture) 蜘蛛膜下腔出血 ( 顱內動脈瘤破裂 )
 蜘蛛膜下腔出血 ( 顱內動脈瘤破裂 )")
23
SAH (II) Watch-out:rebleeding due to incomplete clipping, clipping
Sites of predominance : IC-pc aneurysm anterior communicating aneurysm basilar artery aneurysm. Treatment: 1. Early operation ( within 3 days) 2. Delayed operation ( 14 days) Including:aneurysm clipping aneurysm wrapping aneurysm coagulation ICP monitor insertion Watch-out:rebleeding due to incomplete clipping, clipping erosion, double aneurysm.
 2. Delayed operation ( 14 days) Including:aneurysm clipping. aneurysm wrapping. aneurysm coagulation. ICP monitor insertion. Watch-out:rebleeding due to incomplete clipping, clipping. erosion, double aneurysm.")
24
動脈瘤破裂併發症重症加護 再出血 (Rebleeding) 內科治療:控制血壓 外科治療:clipping…
血管內治療:intravascular coil 腦水腫 (Brain Edema): IICP control 抽筋 (Seizure):抗抽筋藥物使用預防
: IICP control. 抽筋 (Seizure):抗抽筋藥物使用預防.")
25
Spontaneous SAH (Aneurysm Rupture)
Mannitol 75cc ~ 100 cc IVD Q4h Solumedrol 40mg IVD Q6h Gaster 1Amp IVD Q12h Depakine 800mg IVD st then 600mg Q8h Nimodipine run 5cc /hr * 2 hrs then 10cc/hr Perdipine 3cc/hr titrate keep SBP 120 ~150mmHg Pain control: Tramadol, Keto, Codeine Volume: balance

26
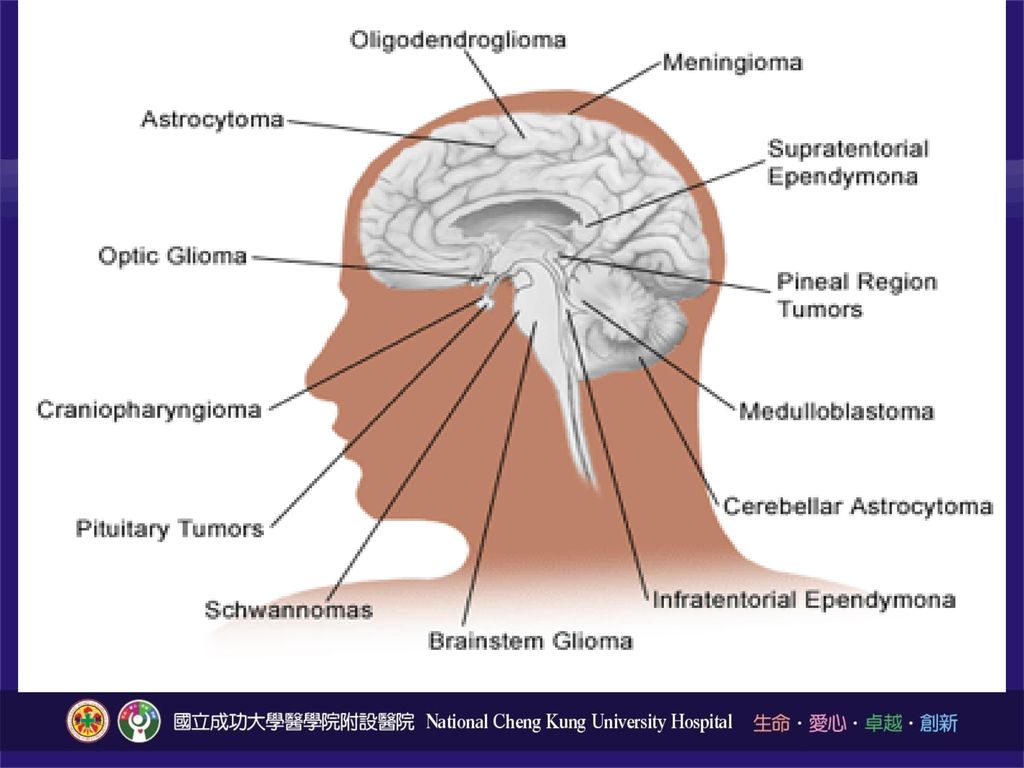
Brain Tumor 由大腦中的組織或是神經細胞所產生的腫瘤 (neurons, glial cells 如 astrocytes, oligodendrocytes, ependymal cells,或 Schwann cells, meninges, skull, blood vessels, pituitary and pineal gland 等或是由顱外所轉移入的) Primary / Secondary 約佔所有惡性腫瘤的1.4%; 因惡性腫瘤死亡的2.4%人口 佔小兒惡性腫瘤的20-25%之多
 Primary / Secondary. 約佔所有惡性腫瘤的1.4%; 因惡性腫瘤死亡的2.4%人口. 佔小兒惡性腫瘤的20-25%之多.")
28
Brain Tumor Symptoms IICP : headache, nausea/vomiting, conscious change Seizures : late onset, 誘發因子, 前驅症狀, 先兆, 發作… Focal neurological deficits 內分泌功能異常

33
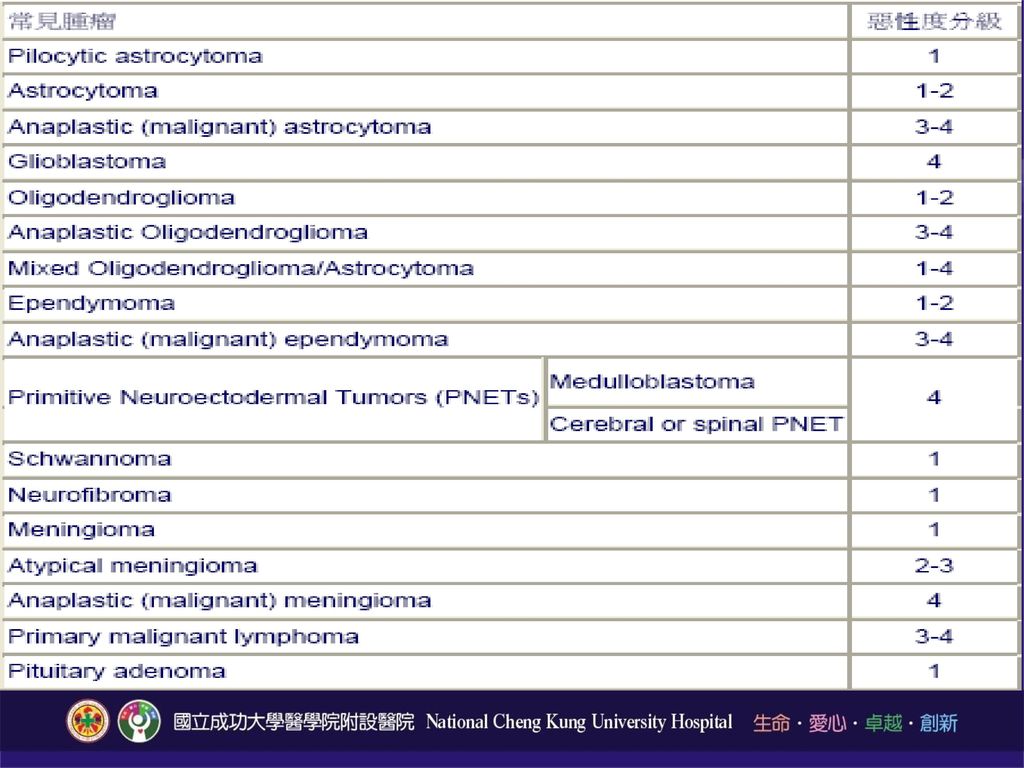
腦瘤 A. 神經上皮性組織腫瘤 a.星狀細胞瘤 I.Astrocytoma, (12.6%) II.Malignant astrocytoma III.GBM (glioblastoma multiforme) (6.3%) IV.Pilocytic astrocytoma b.Oligodendroglioma (1.6%) c.Ependymoma (1.6%) d.mixed glioma e.Choroid plexus tumors:如choroid plexus papilloma (0.5%) f.起源不明之上皮性腫瘤如astroblastoma g.神經細胞性及混合神經膠細胞性瘤: 如gangliocytoma, ganglioglioma h.松果體腫瘤:如pineocytoma, pineoblastoma
 II.Malignant astrocytoma III.GBM (glioblastoma multiforme) (6.3%) IV.Pilocytic astrocytoma b.Oligodendroglioma (1.6%) c.Ependymoma (1.6%) d.mixed glioma e.Choroid plexus tumors:如choroid plexus papilloma (0.5%) f.起源不明之上皮性腫瘤如astroblastoma g.神經細胞性及混合神經膠細胞性瘤: 如gangliocytoma, ganglioglioma h.松果體腫瘤:如pineocytoma, pineoblastoma.")
34
腦瘤 B. Embryonal tumors: a. medulloepithelioma b. neuroblastoma c. ependymoblastoma d. retinoblastoma e. PNET (primitive neuroectodermal tumors)如 Medulloblastoma (1.5%) C.腦脊髓神經腫瘤(6.6%) a. schwannoma (或neurilemoma, neuroma) b. neurofibroma
如. Medulloblastoma (1.5%) C.腦脊髓神經腫瘤(6.6%) a. schwannoma (或neurilemoma, neuroma) b. neurofibroma.")
35
腦瘤 D. Meningeal tumor a. meningioma (23.3%) b. 腦膜細胞以外由中胚層來者 I.良性:chondroma, lipoma, fibroma II.惡性:chondrosarcoma,rhabdomyosarcoma c.原發性黑色素細胞瘤 d.起源不明者: hemangioblastoma,hemangioericytoma E.造血組織 如malignant lymphoma、plasmacytoma
 b. 腦膜細胞以外由中胚層來者 I.良性:chondroma, lipoma, fibroma II.惡性:chondrosarcoma,rhabdomyosarcoma c.原發性黑色素細胞瘤 d.起源不明者: hemangioblastoma,hemangioericytoma. E.造血組織 如malignant lymphoma、plasmacytoma.")
36
腦瘤 F. Germ cell tumors 如germinoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma, teratoma G. Cystic and tumor like lesions 如Rathke's cleft cyst, epidermoid cyst, Dermoid cyst,第三腦室colloid cyst H. 腦下垂體腫瘤:如pituitary adenoma (20.6%) pituitary carcinoma I. Local extension from regional tumors a. craniopharyngioma (分adamantinomatous, squamous, papillary type) b. paraganglioma c. Chordoma d. chondroma J. Metastatic tumors
 pituitary carcinoma. I. Local extension from regional tumors a. craniopharyngioma (分adamantinomatous, squamous, papillary type) b. paraganglioma c. Chordoma d. chondroma. J. Metastatic tumors.")
37
Primary Brain Tumors Malignant Benign
Gliomas (Astrocytomas, anaplastic astrocytomas, Glioblastomas, Oligodendrogliomas, Gangliogliomas, Ependymomas) Lymphomas Medulloblastomas Germ cell tumors Pineoblastomas others Benign Meningiomas Pituitary adenomas Vestibular schwannomas Craniopharyngiomas Pilocytic astrocytomas Colloid cysts Hemangioblastomas Epidermoid cysts others
 Lymphomas. Medulloblastomas. Germ cell tumors. Pineoblastomas. others. Benign. Meningiomas. Pituitary adenomas. Vestibular schwannomas. Craniopharyngiomas. Pilocytic astrocytomas. Colloid cysts. Hemangioblastomas. Epidermoid cysts. others.")
38
Metastasis Lung cancer Breast cancer Colon cancer …

39
Metastatic Tumor

40
Glioma Astrocytoma Grade I: pilocytic Grade II: astrocytoma
Grade III: anaplastic astrocytoma Grade IV: Glioblastoma multiforme Oligodendroglioma

41
Glioblastoma

42
Glioblastoma

43
Meningioma 最常見顱內良性腫瘤, 約佔所有腦瘤的15% Female : Male 2:1
常見於 convexity, parasagital, falx, skull base, posterior fossa, ventricle…等位置

44
Meningioma

46
Cerebellopontine Angle Meningioma

47
Olfactory Groove Meningioma

48
Pituitary Tumor 良性腺瘤佔大多數

51
Craniopharyngioma

52
Vestibular Schwannoma

53
Brain Abscess

54
Medullablastoma

55
Treatment Watch and follow-up Surgery total removal
as maximal as possible Chemotherapy Radiation therapy Radiosurgery

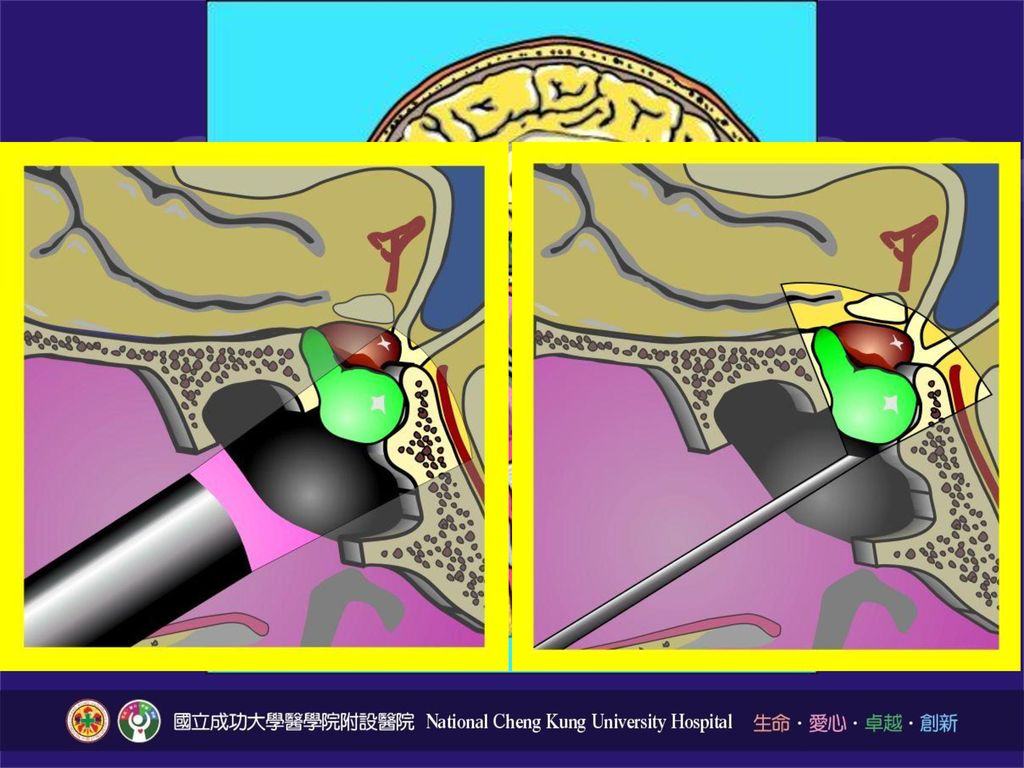
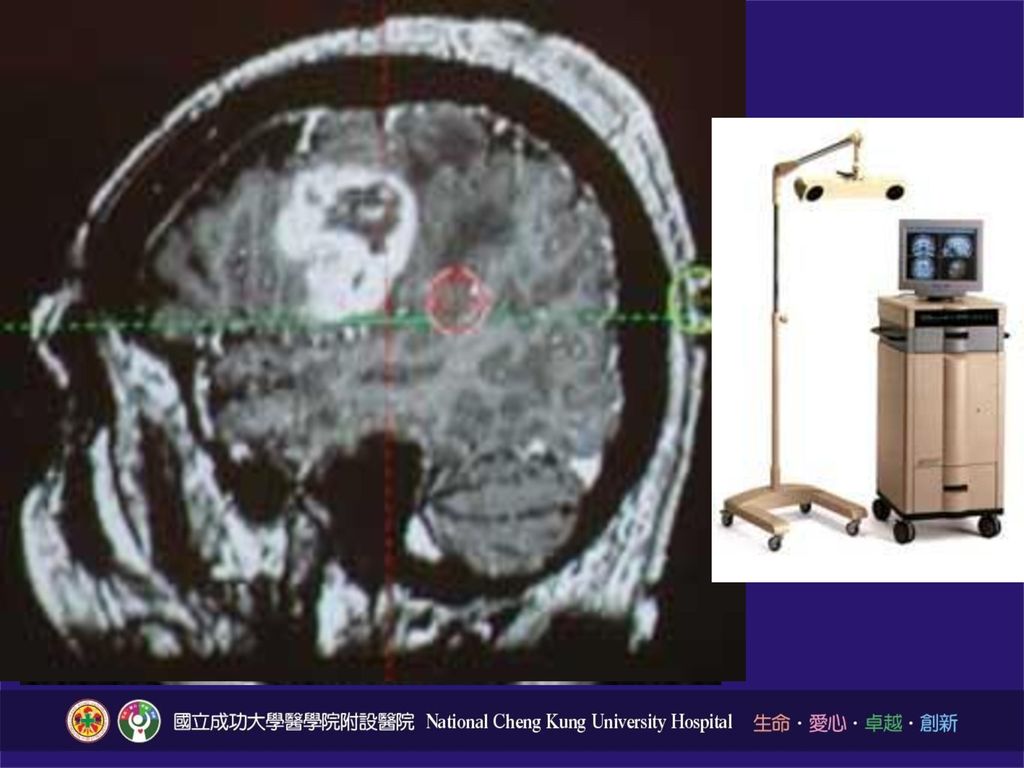
57
Stereotatic Radiosurgery (SRS)
")
58
Glasgow Coma Scale Eyes open (睜眼反應) 4 3 2 1 Spontaneous To speech
To pain None Best Verbal response (最佳語言反應) 5 Alert Confused Drowsy Groans Motor respons(最佳語言反應) 6 Obey Localized pain Withdrawal Abnormal flexion Extension
 5. Alert. Confused. Drowsy. Groans. Motor respons(最佳語言反應) 6. Obey. Localized pain. Withdrawal. Abnormal flexion. Extension.")
59
肌肉張力 肌肉等級(muscle gradations) 運動程度(Description)
5分 正常(normal) 對抗重力及充分阻力情形下可在全部運動範圍內活動 4分 良好(good) 對抗重力及部分阻力情形下可在全部運動範圍內活動 3分 尚可(fair) 對抗重力情形下,可在全部運動範圍內活動 2分 不佳(poor) 去除重力後,可在全部運動範圍內活動 1分 微弱(trace) 具有輕微肌肉收縮力量,關節並無活動 0分 無(zero) 無肌肉收縮現象
 對抗重力及充分阻力情形下可在全部運動範圍內活動. 4分 良好(good) 對抗重力及部分阻力情形下可在全部運動範圍內活動. 3分 尚可(fair) 對抗重力情形下,可在全部運動範圍內活動. 2分 不佳(poor) 去除重力後,可在全部運動範圍內活動. 1分 微弱(trace) 具有輕微肌肉收縮力量,關節並無活動. 0分 無(zero) 無肌肉收縮現象.")
60
開顱手術後常見之問題 出血(延遲性腦出血、傷口出血) 腦水腫 顱內壓升高 癲癇(局部、全身性、癲癇重積狀態) 意識改變 水腦症
其他(CSF leakage, infection)…
…")
61
影響意識狀態因素 構造性腦病變:天幕上(上腦幹功能障礙) 天幕下(網狀系統破壞) 代謝性瀰漫性病變:肝、腎病變、電解質
不平衡、中毒、感染、低 血糖、缺氧、 缺血、癲癇 發作 精神性:譠妄、歇斯底里

62
腦瘤術後照顧 每1-2小時記錄vital signs、GCS、muscle power 、I/O 依意識情況,決定攝食方式和熱量。
靜脈輸液給予N/S 或2.5% G/S,禁食病患每天給予35ml/kg( ml),可進食病患維持暢通即可。 Steroid with Dexamethasone (Decadron/Rinderon) 4-8 mg Q 6-8h。 降腦壓藥 mannitol g/kg, Q4-12h 癲癇發作可給予 dilantin、depakine。 Prevent stress ulcer: H2 blocker / PPI。
,可進食病患維持暢通即可。 Steroid with Dexamethasone (Decadron/Rinderon) 4-8 mg Q 6-8h。 降腦壓藥 mannitol g/kg, Q4-12h. 癲癇發作可給予 dilantin、depakine。 Prevent stress ulcer: H2 blocker / PPI。")
63
腦瘤術後照顧 注意傷口引流管之種類、引流量、顏色等
適當使用止痛及鎮靜劑、避免病人躁動及非醫囑拔管之可能性; 意識回復的病人可考慮移除氣管內管 注意有無CSF滲漏之可能性 (尤其是腦下垂體瘤或後顱窩手術之患者) 比較術前和術後之GCS 、pupil size/light reflex 和 muscle power; 若有差異則考慮追蹤電腦斷層
 比較術前和術後之GCS 、pupil size/light reflex 和 muscle power; 若有差異則考慮追蹤電腦斷層.")
64
神外自費材料同意書

66
ICP monitor placement 置放ICP monitor,協助歸零校正,並記下序號 貼在機身及ICP線上,勿拉扯

67
ICP monitor placement
68
ICU病人請每天記錄GCS, muscle power及病人原有的neurologic sign的變化,注意I/O (若沒有特殊因素, 維持約+500ml/day, Aneurysm clipping術後為預防vasospasm, +500~1000ml/day), 每天check X-ray, electrolyte, ABG等data
, 每天check X-ray, electrolyte, ABG等data")
69
ICU病人請每天記錄GCS, muscle power, pupil size & reflex (brain surgery or head trauma), 或muscle power& DTR (spine surgery or trauma) 及病人原有的neurologic sign的變化
, 或muscle power& DTR (spine surgery or trauma) 及病人原有的neurologic sign的變化")
70
GCS change 一般而言指的是motor下降了兩分以上, Pupil size or reflex有改變, 或其他變化, 要做以下處理
Systemic problem Focal neurologic problem (通常伴隨pupil size or reflex改變, seizure, or IICP)
")
71
顱內出血患者發生意識狀態改變? 延遲性出血 (Delayed hemorrhage) 腦水腫(Cerebral edema)
癲癇(Posttraumatic seizure) 水腦症(Hydrocephalus) 代謝性問題Metabolic abnormalities ( e-, gas ) 感染Infection ( meningitis, abscess ) 其它部位受傷Associated injury ( shock, spine )
 水腦症(Hydrocephalus) 代謝性問題Metabolic abnormalities ( e-, gas ) 感染Infection ( meningitis, abscess ) 其它部位受傷Associated injury ( shock, spine )")
72
Systemic problem Airway有無問題
Check ABG有無CO2 retention, acidosis, hypoxemia 體溫有無發燒, 有無sepsis sign Check electrolyte注意有無electrolyte imbalance Check sugar注意有無hypo- or hyperglycemia Check CBC注意有無anemia

73
Focal neurologic problem
通常伴隨pupil size or reflex改變, seizure, or IICP Brain CT, 通常non-contrast即可, 緊急時請打電話連絡CT room 連絡當天值班的神外醫師

74
IICP的處理 頭高30度, 增進venous return
Hyperventilation: 適用已intubation的病人, keep PaCO2 30~35mmHg (注意! 只適用短時間, 時間一久, vasoconstriction, 反而引起ischemic change) Hyperosmotic agent: 降ICP效力Glycerol < Mannitol < 3% NaCl CSF drainage: 對於有ventriculostomy的病人可以使用, prn放CSF 5 cc Barbiturate coma: Pentothal 3~5mg/kg/hr *24hours then 2.5mg/kg/hr Craniectomy
 Hyperosmotic agent: 降ICP效力Glycerol < Mannitol < 3% NaCl. CSF drainage: 對於有ventriculostomy的病人可以使用, prn放CSF 5 cc. Barbiturate coma: Pentothal 3~5mg/kg/hr *24hours then 2.5mg/kg/hr. Craniectomy.")
75
Mannitol Loading:以60Kgw為例,相當於75-120g,可打1-2瓶 每天劑量:300-1000ml
考慮rebound phenomenon, 是否準時給藥,給藥方便性 75ml Q4h 100ml Q4h 100ml Q3h 150ml Q3h 60g/300ml/btl 作用開始:30-60 mins 作用時間:6-8 hours 半衰期: mins Loading: g/kg infused 成人一般劑量 g/24hours 給藥速率:drip 30-60min (勿全速給藥)
")
76
Glycerol Post concussion syndrome Minor head injury
成年人一般劑量250cc,間隔4小時以上 內含5% fructose,糖尿病人使用要注意 注射太快可能導致溶血

77
Pentothal Barbiturate Coma Pentothal (500) 5Amp in N/S 100 cc Protocol
Loading: 10 mg/Kg IV x 4hrs (24cc/hr ) Maintain: 1 ~ 1.5mg/Kg/hr ( 2.4 ~ 10cc/hr ) 目標:Pentothal level 3-5 mg% & ICP < 24 mmHg 若ICP小於20mmHg, 續用48hrs 再taper Pentothal
 Maintain: 1 ~ 1.5mg/Kg/hr ( 2.4 ~ 10cc/hr ) 目標:Pentothal level 3-5 mg% & ICP < 24 mmHg. 若ICP小於20mmHg, 續用48hrs 再taper Pentothal.")
78
Drain tube V/B, J-vac, Hemovac 美式引流袋

79
V/B, J-vac, Hemovac 一般是放在epidural space或是subgaleal layer, 除非是chronic SDH的病人會放在subdural space, 就在brain的表面, 所以不可壓, 否則會造成acute SDH, 若不確定看op note或詢問operator 放在epidural space or subgaleal layer術後一定要壓, 製造vacuum的效果, 同時要q1h milking, 避免術後產生EDH 常見的craniotomy或craniectomy術後第一天的引流量約 cc, 如果都沒有什麼量流出來, 要檢查有無阻塞, 小心術後發生EDH 有一種情況要改成不壓: 若是術後幾天流出來的fluid 顏色變淡, 類似CSF, 請改成勿壓

80
引流管 Drainage Tube
81
Chronic SDH (慢性硬腦膜下出血)
Risk factor: old age, brain atrophy, coagulopathy Vaccum ball (VB) 勿壓 (硬腦膜下引流管) 平躺, 多喝水, 不用Mannitol
 勿壓 (硬腦膜下引流管) 平躺, 多喝水, 不用Mannitol.")
82
VB可不可以壓? Epidural Subdural drainage ( CSDH )
83
美式引流袋 接EVD用的收集袋, 可同時調整高度決定引流量與監測ICP
Ventriculostomy: EVD tube放在lateral ventricle裡, 可引流CSF, 可監測ICP Cisternostomy: EVD tube放在cistern裡

84
External Ventricular Drainage ( EVD ) ( 腦室引流管 )
 ( 腦室引流管 )")
85
Dysfunction 當monitor上的wave form消失或數字有疑問時, 依序檢查: 管路有無打折, 控制閥是否關閉 重新歸零
將收集瓶放到低於耳洞的高度, 檢查管線內液體是否會流動: 會: 表示ventriculostomy是通的, 只是裡面的CSF不多 不會: 表示管路阻塞, 請通知當天值班的神外醫師

86
CSF收集瓶 注意事項: CSF 引流的量 CSF 顏色 引流瓶通引流袋的卡夾 CSF收集袋

87
藥物的使用 腎功能不好的病人儘量不要使用mannitol, Euglucon, Glucophage, Gaster, or muscle relaxant等 HTN的病人在ICU盡量以短效的藥物為主, 病房則以長效的為主, 常用的藥物如Norvasc¸ long-acting ACEI都需要3 天以上藥量的loading, 不適合用於ICU緊急的病患 Steroid適合用於 vasogenic brain edema, 例如brain tumor引起的perifocal edema, 至於在trauma上並沒有證實有效, 除了central cord syndrome Phenytoin (Dilantin) or Valproate (Depakine): 對於severe brain injury, 特別是temporal lobe injury 有預防early post-traumatic seizure的效果
 or Valproate (Depakine): 對於severe brain injury, 特別是temporal lobe injury 有預防early post-traumatic seizure的效果.")
88
藥物的taper 視病人的病情而定, 如果在taper過程中consciousness有改變, 請回到前一個dose
對elective的病人, 若術前brain swelling不是很厲害, conscious clear,可以在用滿3天後開始taper, 然後一天一個dose 對於trauma的病人, 通常在3-5天可能有delay hemorrhage or perifocal edema, 所以taper的時間要延後, 可以從5-7天之後再開始, 2天一個dose 如果是pure EDH, 而且術後conscious clear, 可以早一點taper

89
Mortality 若有病人病情惡化, AAD, 死亡, 連絡當天值班的神外醫師

91
Craniectomy vs. Craniotomy
Burr Hole ( 顱骨鑽孔 )
92
Craniectomy vs. Craniotomy

93
溫馨提醒 Seizure GCS downhill (pupil dilatation, ICP>20, CPP<70) MP downhill Drain problems Vital sign unstable DI Abnormal lab data Call me

94
NS=戰場

95
Thanks for your attention

96
有問題嗎?

Similar presentations









: 50ml/100g/min CBF= 腦灌注壓 / 腦血管阻力 腦灌注壓 (CPP)=MAP-ICP(or CVP) a. MAP 50~150mmHg,CBF 維持恆定 b. PaCO2:>")

 第一节.>")
 病理生理学系 Department of Pathophysiology 高远生.>")








 河南中医学院第一附属医院 杜正光>")