Download presentation
Presentation is loading. Please wait.

1
中国协和医科大学 北京协和医院神经科 万新华
运动障碍病 中国协和医科大学 北京协和医院神经科 万新华

2
运动障碍病的定义 锥体外系疾病:Extrapyramidal diseases 运动障碍疾病:Movement Disorders
由于脑基底节或黑质结构功能紊乱导致的以随意运动调节功能障碍为特征的一组疾病 运动障碍疾病:Movement Disorders 发生于意识清醒病人的随意运动调节功能障碍为特征的一组疾病

3
运动障碍病的特点 通常与基底节或多巴胺神经递质传导功能紊乱有关;
临床上导致运动调节功能障碍,而非运动能力本身;故肌力、感觉和小脑一般不受影响; 临床上主要表现为:肌张力降低-运动过多 所致的异常不自主运动和肌张力增高-运动减少所致的运动贫乏两大类; 所有不自主运动受病人精神状态影响,紧张时加重,睡眠时消失。

4
运动障碍病分类 运动增多类 腹部异动症(Abdominal dyskinesias)
静坐不能性运动(Akathitic movements) 协调不能/共济失调 (Asynergia / ataxia) 手足徐动症(Athetosis) 投掷症(Ballism) 舞蹈症(Chorea) 辩距不良(Dysmetria) 肌张力障碍(Dystonia)
 协调不能/共济失调 (Asynergia / ataxia) 手足徐动症(Athetosis) 投掷症(Ballism) 舞蹈症(Chorea) 辩距不良(Dysmetria) 肌张力障碍(Dystonia)")
5
运动增多类 偏侧面肌痉挛(Hemifacial spasm) 惊跳症(Hyperekplexia〕
睡眠源性异动症 (Hypnogenic dyskinesias) 肢残跳动 (Jumpy stumps〕 痛肢趾(指)多动症 (Painful legs-moving toes / fingers syndrome) 肌阵挛 (Myoclonus)
 肢残跳动 (Jumpy stumps〕 痛肢趾(指)多动症 (Painful legs-moving toes / fingers syndrome) 肌阵挛 (Myoclonus)")
6
运动增多类 myorhythmia(Whipple’s disease) 肌蠕动 (Myokymia)
发作性异动症(Paroxysmal dyskinesias , PKD 和PNKD) 不安腿 (Restless legs) 刻板症 (Stereotypy) 抽动症 (Tics) 震颤 (Tremor)
 不安腿 (Restless legs) 刻板症 (Stereotypy) 抽动症 (Tics) 震颤 (Tremor)")
7
运动减少类 运动不能/运动迟缓(Akinesia / bradykinesia, parkinsonism) 失用(Apraxia)
阻滞性抽动症(Blocking tics) 紧张症,精神运动性抑郁和强迫症性迟缓 (Catatonia, psychomotor depression, and obsessional slowness) 冻结现象( Freezing phenomenon) 甲状腺功能低下性迟缓 ( Hypothyroid slowness) 僵人综合症(Stiff-person syndrome)
 紧张症,精神运动性抑郁和强迫症性迟缓. (Catatonia, psychomotor depression, and obsessional slowness) 冻结现象( Freezing phenomenon) 甲状腺功能低下性迟缓 ( Hypothyroid slowness) 僵人综合症(Stiff-person syndrome)")
8
THE PREVALENCE OF MDs ENCOUNTERED IN MD CLINICS
MOVEMENT DISORDER NUMBER OF PATIENTS PERCENT Parkinsonism 7,564 32.9 Parkinson’s disease 5,410 Progressive supranuclear palsy 381 Multiple system atrophy 349 Cortical-basal ganglionic degeneration 143 Vascular 265 Drug-induced 227 Hemiparkinsonism-hemiatrophy 81 Gait disorder 187 Other 521

9
THE PREVALENCE OF MDs ENCOUNTERED IN MD CLINICS
MOVEMENT DISORDER NUMBER OF PATIENTS PERCENT Dystonia 6,798 31.3 Primary dystonia 5,247 focal % segmental % generalized % Secondary dystonia 1,551 Hemidystonia 191 Tardive dystonia 472 Other 888

10
THE PREVALENCE OF MDs ENCOUNTERED IN MD CLINICS
MOVEMENT DISORDER NUMBER OF PATIENTS PERCENT Tremor 3,013 13.9 Essential tremor 2,082 Cerebellar 151 Midbrain (‘rubral’) 86 Primary writing 59 Orthostatic 16 Other 619
 86. Primary writing. 59. Orthostatic. 16. Other")
11
THE PREVALENCE OF MDs ENCOUNTERED IN MD CLINICS
MOVEMENT DISORDER NUMBER OF PATIENTS PERCENT Tics (Tourette’s syndrome) 1,022 4.7 Chorea 658 3.1 Huntington’s disease 282 Hemiballism 62 Other 314 Tardive syndromes 583 2.7 Myoclonus 547 2.5
 1, Chorea Huntington’s disease Hemiballism. 62. Other Tardive syndromes Myoclonus")
12
THE PREVALENCE OF MDs ENCOUNTERED IN MD CLINICS Hemifacial spasm 359
MOVEMENT DISORDER NUMBER OF PATIENTS PERCENT Hemifacial spasm 359 1.7 Ataxia 316 1.5 Paroxysmal dyskinesias 169 0.8 Stereotypies(other than TD) 163 0.7 Restless legs syndrome 108 0.5 Stiff-person syndrome 32 0.1 Psychogenic movement disorder 434 2.0 GRAND TOTAL 21,766 100
 Restless legs syndrome Stiff-person syndrome Psychogenic movement disorder GRAND TOTAL. 21,")
13
帕金森病 《黄帝内经》中早已对震颤麻 的症状有所描述。 我国唐代著名医学家孙 思邈在《千金方》中也曾报 道一例震颤麻痹患者。
我国古代医学的奠基之作 《黄帝内经》中早已对震颤麻 的症状有所描述。 我国唐代著名医学家孙 思邈在《千金方》中也曾报 道一例震颤麻痹患者。 首先我们来回顾一下帕金森病的历史。帕金森病在我国已有“悠久历史”,我国古代医学的奠基之作《黄帝内经》中早已对震颤麻痹的症状有所描述。唐代的著名医学家孙思邈在《千金方》中也曾报道了一例震颤麻痹患者。 直到1817年,英国医生James Parkinson报告了6例病例,首次提出“震颤麻痹”并对该疾病进行了描述。

14
Monograph by James Parkinson
AN ESSAY ON THE SHAKING PALSY CHAPTER I DEFINITION-HISTORY-ILLUSTRATIVE CASES SHAKING PALSY. (Paralysis Agitans.) Monograph by James Parkinson 1817
 Monograph by James Parkinson")
15
帕金森病的流行病学 发病率 患病率 发病年龄 全世界:5-24/ 105 (美国: 20.5/105) 随年龄增长而增高
全世界:5-24/ 105 (美国: 20.5/105) 随年龄增长而增高 患病率 全世界:57-371/105 (美加 300/105) 未诊断率:35%-42% 北京、上海和西安调查:65岁2.1%,约40~70%未诊断 发病年龄 平均 62.4 岁 30岁前少见; 40岁前 4-10% The incidence of parkinson syndrome and Parkinson’s disease rises with age, and has been reported at between five and twenty-four cases per hundred thousand. The best available incidence studies--those from the Rochester, Minnesota, database--suggest the incidence of parkinson syndrome in the U.S.A. is 20.5 per 100,000 population. Because the population is slowly aging, and the recognition of parkinsonism is improving, it is expected that the incidence will slowly rise. Door-to-door prevalence surveys of the general population have revealed that 35-42% of the cases of parkinson syndrome in the general population remain undiagnosed. Most of those would be early cases, those with akinetic-rigid form of parkinsonism, or those who have been mistaken as having had a neurological disease such as essential tremor. The reported prevalence rates range from per 100,000 population. In the U.S. and Canada it is estimated that the prevalence is 300 per 100,000 population. This should be regarded as a conservative estimate. A review of 934 patients found the onset of parkinson syndrome was at age 61.6, while the onset of Parkinson’s disease was at age 62.4 years. Parkinsonism is very rare before age 30 and only 4-10% of the cases have onset before the age of 40 years.
 随年龄增长而增高. 患病率. 全世界:57-371/105 (美加 300/105) 未诊断率:35%-42% 北京、上海和西安调查:65岁2.1%,约40~70%未诊断. 发病年龄. 平均 62.4 岁. 30岁前少见; 40岁前 4-10% The incidence of parkinson syndrome and Parkinson’s disease rises with age, and has been reported at between five and twenty-four cases per hundred thousand. The best available incidence studies--those from the Rochester, Minnesota, database--suggest the incidence of parkinson syndrome in the U.S.A. is 20.5 per 100,000 population. Because the population is slowly aging, and the recognition of parkinsonism is improving, it is expected that the incidence will slowly rise. Door-to-door prevalence surveys of the general population have revealed that 35-42% of the cases of parkinson syndrome in the general population remain undiagnosed. Most of those would be early cases, those with akinetic-rigid form of parkinsonism, or those who have been mistaken as having had a neurological disease such as essential tremor. The reported prevalence rates range from per 100,000 population. In the U.S. and Canada it is estimated that the prevalence is 300 per 100,000 population. This should be regarded as a conservative estimate. A review of 934 patients found the onset of parkinson syndrome was at age 61.6, while the onset of Parkinson’s disease was at age 62.4 years. Parkinsonism is very rare before age 30 and only 4-10% of the cases have onset before the age of 40 years.")
16
帕金森病的主要症状: TRAP 三大症状: 静止性震颤( resting Tremor) 肌强直( Rigidity) 运动不能( Akinesia) 姿势反射障碍(Postural instability): (随病情进展出现,也是PD的核心症状)
")
17
帕金森病的运动症状 步态和轴位姿势 头部症状 上、下肢远端症状 轴位上的姿势改变 在床上翻身困难 步态缓慢,拖步 慌张步态 面具脸
步态缓慢,拖步 慌张步态 上、下肢远端症状 小字症 精细动作损害 静息性震颤 足趾肌张力障碍 头部症状 面具脸 说话犹豫、语调低平及 构音障碍 瞬目减少 眼球调节障碍 强迫性闭眼 吞咽困难 流涎

18
帕金森病的非运动症状 精神和睡眠 植物神经 感觉 运动症状前的人格改变 直立性低血压 抑郁 胃肠运动受损 焦虑 膀胱功能障碍 非常逼真的梦
断续的睡眠 感觉 麻木和刺痛感 感觉异常:如温热感 静坐不能:感觉不安 嗅觉缺失 视觉集中敏感性受损 植物神经 直立性低血压 胃肠运动受损 膀胱功能障碍 体温调节障碍 瞳孔对光反射减弱 脂溢性皮炎 体重减轻 性功能障碍

19
定义 帕金森综合征:以震颤、运动迟缓、肌张力增高和平衡障碍为临床特征的一组疾病症侯群 帕金森病:病因不明的帕金森综合征
继发性帕金森病:由已知原因所致的帕金森综合征,如脑炎或MPTP引起 帕金森叠加综合征或非典型性帕金森病:具有帕金森综合征和其它症状的一组神经变性疾病

20
帕金森综合征分类(1) 原发性帕金森病(Primary) 继发性帕金森病(Secondary) 药物引起(抗精神病药) 感染(脑炎、梅毒)
代谢性(肝脑变性、缺氧、甲状腺功能紊乱) 结构性(脑肿瘤、脑积水、脑外伤) 中毒性(CO、二硫化碳、锰、氰化物、MPTP) 血管性(动脉硬化)
 结构性(脑肿瘤、脑积水、脑外伤) 中毒性(CO、二硫化碳、锰、氰化物、MPTP) 血管性(动脉硬化)")
21
帕金森综合征分类(2) 帕金森叠加综合征(Parkinsonism-plus syndrome)
进行性核上性麻痹(Progressive supranuclear palsy, PSP) 多系统萎缩(Multiple system atrophy,MSA) 纹状体黑质变性(Striatonigral degeneration,SND) Shy-Drager综合征(SDS) 橄榄桥脑小脑萎缩(Olivopontocerebellar atrophy,OPCA) 皮层基底节变性(Corticobasal degeneration,CBD) 弥散型露易小体病(Diffuse Lewy body disease,LBD)
 多系统萎缩(Multiple system atrophy,MSA) 纹状体黑质变性(Striatonigral degeneration,SND) Shy-Drager综合征(SDS) 橄榄桥脑小脑萎缩(Olivopontocerebellar atrophy,OPCA) 皮层基底节变性(Corticobasal degeneration,CBD) 弥散型露易小体病(Diffuse Lewy body disease,LBD)")
22
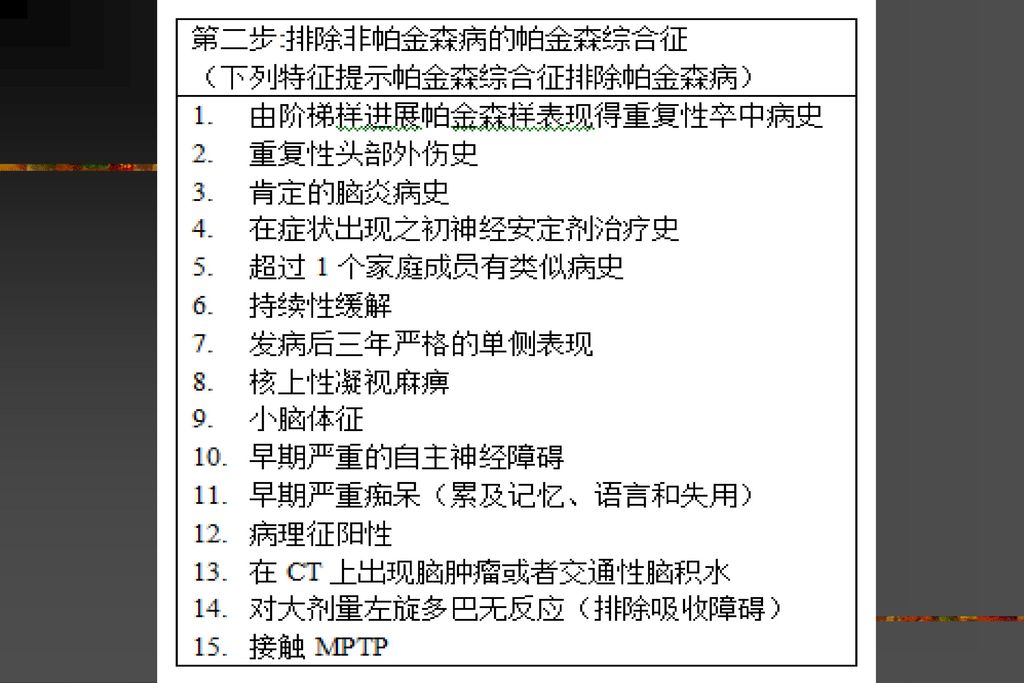
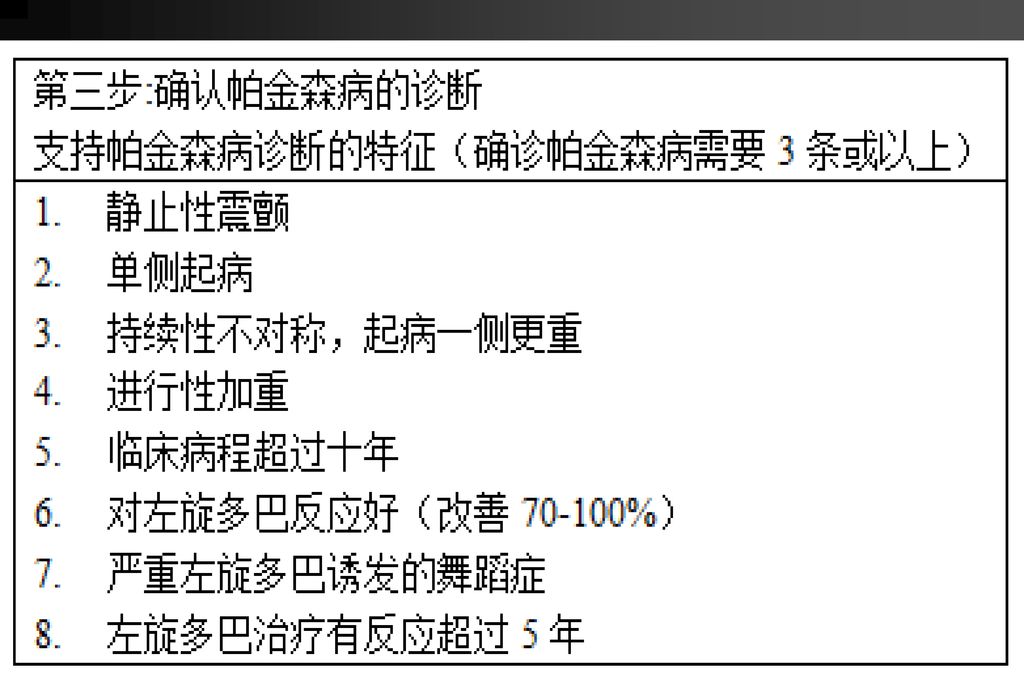
临床诊断标准

23
临床诊断标准

26
PD与帕金森叠加综合征的鉴别 震颤 僵直 运动慢而减少 姿势平衡障碍 锥体束征 小脑征 植物N功能不良 痴呆 轴和项扭转痉挛 核上性凝视麻痹
对L-Dopa反应 ++++ ++ good + +++ Poor PD OPCA Shy PSP Striatonigral -Drager Degeneration Absent 0=不发生, +=少见, ++=常见, +++=很常见 Goetz CG, et al. 1995

27
PD 的病因 不清; 与老化有关但不是单纯的accelerated aging 遗传 常染色体显性(或隐性)遗传家族发病
阳性家族史、双胞胎研究 环境 大部分病例为散发性,支持环境因素的作用 遗传与环境的相互作用? The cause in idiopathic Parkinson’s disease is unknown, but it is not accelerated aging. Rarely is Parkinson’s disease inherited as a dominant disorder. Mutation of Alpha synuclein gene (chromosome 4q) has been identified in one large Italian family, the Contursi family, and in five Greek families. Mutation of the parkin gene has been identified as the cause of autosomal-recessive juvenile parkinsonism. In the overwhelming majority of familial cases of Parkinson’s disease, no genetic abnormality has been identified. In the majority of cases the disease is believed to be caused by environmental factors. The place of birth and residence seem to play a greater role than the race. Blacks living in the U.S. have nearly five times the risk as Blacks living in Nigeria. Blacks and Whites living in the same community in the U.S. have similar risks of Parkinson’s disease.
 has been identified in one large Italian family, the Contursi family, and in five Greek families. Mutation of the parkin gene has been identified as the cause of autosomal-recessive juvenile parkinsonism. In the overwhelming majority of familial cases of Parkinson’s disease, no genetic abnormality has been identified. In the majority of cases the disease is believed to be caused by environmental factors. The place of birth and residence seem to play a greater role than the race. Blacks living in the U.S. have nearly five times the risk as Blacks living in Nigeria. Blacks and Whites living in the same community in the U.S. have similar risks of Parkinson’s disease.")
28
基底神经节 Neuroanatomy of the Basal Ganglia
The basal ganglia are a group of nuclei lying deep in the subcortical white matter of the frontal lobes that organize motor behavior. Due to their subcortical location, the basal ganglia are ideally situated to provide communication between the cortex and thalamus via a feedback loop. Sensorimotor information from the cortex is processed by the basal ganglia, which consists of the striatum, the internal globus pallidus (GPi), the external globus pallidus (GPe), the subthalamic nucleus (STN) and the substantia nigra pars reticulata (SNr). Cortical information is relayed to the striatum (the “input” nuclei) via glutamatergic neurons. This cortical information is regulated within tight controls by a constant dopaminergic input from the substantia nigra pars compacta (SNc). Therefore, adequate amounts of dopamine are key for the proper functioning of this complex neuronal network. Parent et al. Trends Neurosci 1993: 16; 111–115. Parent et al 1993
, the external globus pallidus (GPe), the subthalamic nucleus (STN) and the substantia nigra pars reticulata (SNr). Cortical information is relayed to the striatum (the input nuclei) via glutamatergic neurons. This cortical information is regulated within tight controls by a constant dopaminergic input from the substantia nigra pars compacta (SNc). Therefore, adequate amounts of dopamine are key for the proper functioning of this complex neuronal network. Parent et al. Trends Neurosci 1993: 16; 111–115. Parent et al")
29
帕金森病病理改变
30
帕金森病的病理生化改变 黑质和蓝斑核含黑色素的多巴胺神经元大量丧失(50-70%) 以及胶质细胞增生。
路易氏(Lewy)小体:胞桨内园形嗜酸性致密包含体 ,周围呈晕轮状。含大量共核蛋白 。 纹状体多巴胺含量显著减少(80-99%),生化异常与临床症状的严重程度成正比。 进行性多巴胺神经元变性和死亡 。
小体:胞桨内园形嗜酸性致密包含体 ,周围呈晕轮状。含大量共核蛋白 。 纹状体多巴胺含量显著减少(80-99%),生化异常与临床症状的严重程度成正比。 进行性多巴胺神经元变性和死亡 。")
31
帕金森病病理诊断标准 ①多巴胺能神经元减少 (>50%)和黑质中存在胶质细胞
②在黑质或蓝斑中至少存在一个路易小体(在这些区域的3~4张病理切片,不重叠 ) ③没有能产生其他原因帕金森症的病理证据
 ③没有能产生其他原因帕金森症的病理证据.")
32
Braak 临床分期(2003) 运动障碍前期: stage 1:(IX,X运动神经背核) 嗅觉;
stage II:(延髓) 睡眠,头痛,运动减少,情感; stage III:(桥脑被盖) 体温调节,认知,抑郁,背疼; 运动障碍期: (致密部) stage IV:四主症; 运动-精神障碍期: stage V:(新皮层) 运动波动,频发疲劳; stage VI:(新皮层) 错乱,视幻觉,痴呆,精神症状
 睡眠,头痛,运动减少,情感; stage III:(桥脑被盖) 体温调节,认知,抑郁,背疼; 运动障碍期: (致密部) stage IV:四主症; 运动-精神障碍期: stage V:(新皮层) 运动波动,频发疲劳; stage VI:(新皮层) 错乱,视幻觉,痴呆,精神症状.")
33
帕金森病疾病临床分期 Hoehn-Yahr 疾病分期评分 I 期 : 单侧受影响 II 期 : 双侧受影响但无姿势平衡障碍
IV 期 : 病人日常生活明显受限 ,但在他人帮助下仍可进行 一定活动 V 期 : 病人生活完全不能自理 ,必须卧床

34
疾病严重度评估 UPDRS:创建于1980s 新修订的UPDRS 新修订的UPDRS的附件 日常生活的非运动症状 日常生活的运动症状
运动检查 运动并发症 新修订的UPDRS的附件 ‘建议的’进一步评估量表,例如:认知/SCOPA-cog,白天思睡/SCOPA-sleep

35
帕金森病的治疗

36
左旋多巴时代前后PD病人的存活率 This shows 215 parkinson patients who had onset and first clinic visit before January 1, 1974, when levodopa was least accessible to most of these patients. The observed survival is significantly reduced compared to expected survival in the general population of the same year of birth and same sex, with p< Since the widespread use of levodopa, 565 parkinson patients had onset and were first seen after December 31, 1973 when levodopa was readily available in the study area, and covered by medical insurance. The survival is reduced compared to expected (p=0.029). The difference between the observed and expected survival in these patients is much smaller than in patients who had restricted access to levodopa.
. The difference between the observed and expected survival in these patients is much smaller than in patients who had restricted access to levodopa.")
37
PD治疗目的 改善病人的运动和非运动症状 提高病人的日常生活能力 减少药物治疗后的并发症 治愈疾病

38
帕金森病治疗方法 药物治疗 外科治疗 促多巴胺释放药物 左旋多巴类制剂 B型单胺氧化酶抑制剂(MAO-BI)
抗胆碱能药物 促多巴胺释放药物 左旋多巴类制剂 多巴胺受体激动剂 B型单胺氧化酶抑制剂(MAO-BI) 儿茶酚胺氧位甲基转移酶抑制剂(COMTI) 脑保护剂 外科治疗 毁损术(苍白球或丘脑) 脑深部刺激术(DBS) 干细胞治疗 基因治疗
 儿茶酚胺氧位甲基转移酶抑制剂(COMTI) 脑保护剂. 外科治疗. 毁损术(苍白球或丘脑) 脑深部刺激术(DBS) 干细胞治疗. 基因治疗.")
39
治疗PD药物的分类 Dopaminergic agents COMT inhibitors 恩托卡朋
Levodopa 美多巴、息宁 Dopamineagonists 泰舒达、溴隐亭 、协良行、普拉克索 COMT inhibitors 恩托卡朋 MAO-B inhibitors 司吉宁 Others Anticholinergics 安坦 Amantadine 金刚烷胺 Dopaminergic therapy with levodopa or dopamine agonists is the cornerstone of symptomatic management of Parkinson’s disease. As can be seen in the next slide, levodopa replaces dopamine presynaptically, while dopamine agonists act directly on receptors post-synaptically. Levodopa is administered with a peripheral decarboxylase inhibitor, either benserazide or carbidopa. The newest class of drugs, the COMT inhibitors, also increase the bioavailability of levodopa, by inhibiting peripheral or central catechol O-methyl transferase. Other agents are anticholinergics, the MAO-B inhibitor selegiline, and the antiviral amantadine.

40
Diagram of LD Metabolism
Levodopa is actively transported across the gut barrier and the blood-brain barrier via the large neutral amino acid carrier. It is believed to be subsequently taken up by the presynaptic nigral neuron, where it is converted into dopamine and can then be released in a physiologic fashion into the synaptic cleft. When levodopa is administered along with other dietary amino acids, competition will exist for transport across both the gut and the blood-brain barriers. This is the primary reason why administration with food is generally not advised, since levodopa will not be fully absorbed when administered in this fashion. In the peripheral circulation, levodopa is rapidly decarboxylated into dopamine, where it is then quickly degraded. Dopamine itself does not cross the blood-brain barrier, and can stimulate the area postrema, causing significant nausea and vomiting. In the early days of levodopa therapy, many patients had considerable difficulty tolerating levodopa because of its emesis-producing characteristics. A few years after levodopa was brought into clinical practice, a decarboxylase inhibitor was developed which prevents peripheral degradation of dopamine, thereby enabling a much larger percentage of levodopa to actually cross the blood-brain barrier into the central compartment. There are a number of decarboxylase inhibitors available around the world, the two most common being carbidopa in the United States and benserazide in Europe and elsewhere. With a decarboxylase inhibitor, the drug is rapidly absorbed into the brain, usually 30 to 45 minutes after oral ingestion, and once in the central nervous system the drug has a half-life of about 60 to 90 minutes.

41
一、多巴胺受体激动剂 机制:直接作用突触后多巴胺受体
使用:对早期病人可单用,也可与多巴制剂合用治疗中、晚期病人。不易引起异动症和症状波动,并可推迟和减少多巴制剂的使用。 用法:小剂量开始,缓慢增加剂量,使用剂量应个体化。 副作用:消化道症状、体位性低血压、幻觉及意识模糊等。注意嗜睡发作。

42
二、单胺氧化酶B抑制剂 机制:抑制多巴胺的氧化降解,减少氧化自由基的生成。神经保护作用?
使用:对早期病人可单用,也可与多巴制剂合用治疗中期病人。不易引起异动症和症状波动。 用法:司吉林(seleegiline)、丙炔苯丙胺(deprenyl);5-10mg, 两次/日。 副作用:消化道症状、体位性低血压。失睡多见,故不宜晚上用。
、丙炔苯丙胺(deprenyl);5-10mg, 两次/日。 副作用:消化道症状、体位性低血压。失睡多见,故不宜晚上用。")
43
三、左旋多巴制剂 机制:补充外源性多巴胺前体 左旋多巴合并多巴脱羧酶抑制剂是目前最有效的 药物。
作用:对各期病人均有效。多主张出现姿势平衡障碍或工作受到影响时使用。它对运动迟缓和肌强直疗效好,对震颤亦有效。 药物:左旋多巴+苄丝肼 =美多巴 左旋多巴+ 卡比多巴= 息宁

44
左旋多巴制剂剂型 普通剂型: 左旋多巴控释剂:息宁 左旋多巴弥散型制剂或水剂 美多巴: 200mg 左旋多巴 + 50mg 苄丝肼

45
左旋多巴制剂治疗原则 小剂量开始,个体化调整(病人需求和生活质量),求长效,而不求全效。
一般 mg bid,每2-4天后,加125mg/天,以达到能维持一般生活质量的最低剂量为维持剂量。 饭前或饭后1小时服用

46
四、儿茶酚甲基转移酶(COMT)抑制剂 机制:抑制外周和/或中枢多巴的降解代谢,使血浆或脑内多巴胺明显增加;
作用:增加左旋多巴的生物利用度和作用时间,而不增加左旋多巴的峰值血桨浓度;可增加左旋多巴通过血脑屏障进入脑; 适用症:出现剂末效应或“开-关”现象,与左旋多巴同时服用; 药物:恩托卡朋(entacapone,comtan) ;100 ~ 200 mg 副作用:肝脏损害
 ;100 ~ 200 mg. 副作用:肝脏损害.")
47
五、其它对症治疗:抗胆碱能药物 1867年Ordenstein首先使用 作用:只对以震颤为主的早期病人有效 机制:胆碱能抑制剂
药物:安坦 (2-4mg tid) 副作用:口干、排尿障碍、扩瞳、心动过速、记忆减退、意识模糊等。对65岁 以上和认知障碍者不用。
 副作用:口干、排尿障碍、扩瞳、心动过速、记忆减退、意识模糊等。对65岁 以上和认知障碍者不用。")
48
五、其它对症治疗:金钢烷胺 1969年Schwab等使用 作用:早期病人的运动迟缓和震颤、或与左旋多巴联合用药,可出现耐受性。
机制:弱兴奋性氨基酸受体阻断剂。 药物:金钢烷胺 (50-100mg, bid or tid) 副作用:恶心、眩晕,可加重精神症状。肾功能减退时不用。忌急撤药。
 副作用:恶心、眩晕,可加重精神症状。肾功能减退时不用。忌急撤药。")
49
L-dopa 的并发症 5 年 病程 药效 DA储存 2.0 1.47 1.37 并发症 剂未现象 开关现象 异动症 僵住现象 认知功能障碍

50
随疾病进展出现的并发症 治疗相关的运动并发症 (2) 疾病发展相关的症状和并发症 (3)植物神经功能障碍
运动波动、异动、运动不能危象 (2) 疾病发展相关的症状和并发症 冻结、姿势平衡不能、言语困难、吞咽困难、认知障碍 、睡眠障碍、情绪异常 (3)植物神经功能障碍 体位性低血压、多汗、便秘、性功能障碍
 疾病发展相关的症状和并发症. 冻结、姿势平衡不能、言语困难、吞咽困难、认知障碍 、睡眠障碍、情绪异常. (3)植物神经功能障碍. 体位性低血压、多汗、便秘、性功能障碍.")
51
运动并发症 运动症状波动 (Motor Fluctuations) 异动症 (Dyskinesia) 剂末效应(Wearing-off)
“开-关 ”现象 (On-off) 僵住(Freezing) 异动症 (Dyskinesia) 关期肌张力不全 (Early-morning dystonia) 峰期不自主舞蹈样运动 (Peak-dose dyskinesia) 剂初和剂未期异动症 (Onset and end-of-dose dyskinesia)
 僵住(Freezing) 异动症 (Dyskinesia) 关期肌张力不全 (Early-morning dystonia) 峰期不自主舞蹈样运动 (Peak-dose dyskinesia) 剂初和剂未期异动症 (Onset and end-of-dose dyskinesia)")
52
症状波动—原因 外周原因: 中枢原因: 胃排空速度减慢 饮食中蛋白太多 血中半衰期缩短 对多巴胺受体脉冲式刺激 多巴胺贮存能力下降
多巴胺受体的变化 Factors that influence peripheral levodopa kinetics include delayed gastric emptying, competition from dietary protein and the short plasma half-life of the traditional “immediate release” levodopa. Central causes of motor fluctuations are those that are produced from central nervous fluctuations, including pulsatile delivery of exogenous dopamine through levodopa to the striatal receptors, impaired storage capacity and alteration of both postsynaptic and presynaptic dopamine receptors.

53
出现运动并发症的危险因素 年轻发病 疾病程度严重 左旋多巴剂量高 病程长
On the left top is a picture of a normal midbrain with abundant pigmentation of the substantia nigra. Below that is the midbrain from a Parkinson’s disease patient with the substantia nigra depigmented. The second set at the top is the microscopic section of normal substantia nigra. Below that is the section from substantia nigra of a Parkinson’s patient. It shows profound loss of pigmented neurons and gliosis. On the extreme right is a pigmented neuron containing a Lewy body inclusion. The Lewy body is characterized by dense pink center and light pink periphery. Together, the loss of substantia nigra dopaminergic neurons and the presence of Lewy body inclusions are regarded as the hallmark of idiopathic Parkinson’s disease pathology.

54
持续性多巴胺能刺激(CDS) 概念: 概念的核心 目的:
给予长半衰期的多巴胺能药物或者改进多巴胺能药物的给药模式,提供更加持续的多巴胺受体刺激。 概念的核心 优化多巴胺能药物的药物代谢动力学 使纹状体多巴胺浓度保持基本稳定 纹状体多巴胺受体受到持续激活 目的: 预防/治疗运动并发症

55
帕金森病的外科治疗 手术类型 适应征 震颤 僵直 行动迟缓 异动症 步态 僵住 苍白球毁损术 +/++ ++ + 丘脑毁损术 -
深部电极刺激 胎脑移植 不确定

56
Lecture Notes References
The most recent version of the Parkinson’s disease treatment algorithm is shown on this slide. Nonpharmacologic management of Parkinson’s disease and patient education are very important. The Internet is a resource for this information. Three good Web sites are: WE MOVE ( The National Parkinson’s Foundation ( and the American Parkinson’s Disease Association ( Although selegiline is listed as a neuroprotective agent in the algorithm, clinical data from the follow-up to the DATATOP study do not support its putative neuroprotective properties. The decision to start drug therapy is dictated by signs of functional impairment. The algorithm has been modified to add the new clinical information that has been discussed in this presentation, ie, otherwise healthy patients aged 70 to 75 years can be started on dopamine agonist therapy. Patients over 60 years old who are not in good health should begin therapy with levodopa. At this time, there is no long-term data on the benefit of adding COMT inhibitor to L-dopa at the start of therapy to decrease long-term complications. COMT inhibitors will not delay the onset of motor fluctuations and are better used in the latter stages of illness when wearing off develops. References 1. Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson's disease (2001): treatment guidelines. Neurology. 2001;56 (suppl 5):S1-S Parkinson Study Group. Impact of deprenyl and tocopherol treatment on Parkinson's disease in DATATOP subjects not requiring levodopa. Ann Neurol. 1996;39:29-36.
 for the management of Parkinson s disease (2001): treatment guidelines. Neurology. 2001;56 (suppl 5):S1-S Parkinson Study Group. Impact of deprenyl and tocopherol treatment on Parkinson s disease in DATATOP subjects not requiring levodopa. Ann Neurol. 1996;39:")
57
舞蹈征(chorea) 在希腊文中指跳舞 表现为快速、不规则的、主要影响肢体远端的不自主运动,常为双侧性 常伴有肌张力低
多见于小舞蹈病、Huntington病、肝豆状核变性等病

58
肝豆状核变性 诊断 血清铜兰蛋白<150 (260~360)mg/L 影响因素:避孕药、类风关、个体病程波动
24小时尿铜:>100微克,血清铜不准 MRI:底节、脑桥、中脑,延髓不受累 警惕 儿童不明原因肝病 神经精神症状原因不明 家族史

59
肝豆状核变性 治疗 分期、分型,终身间断维持治疗 症状前治疗最好用锌剂,起效慢,可用于妊娠
青霉胺治疗前青霉素皮试,750~1000mg/d(10~30%不能耐受,过敏反应) 24小时尿铜:200~500微克,或较前增加一倍 >1年(24小时尿铜达300~400微克),间断用药
 24小时尿铜:200~500微克,或较前增加一倍. >1年(24小时尿铜达300~400微克),间断用药.")
60
肌张力障碍(Dystonia) 最常见的运动障碍病(Movement Disorders)之一
定义:一种不自主、持续性的肌肉收缩引起扭曲、重复运动或姿势异常的综合征 患病率30/10万。 表现多样,临床较多存在概念陈旧、诊断名称混淆,易误诊、漏诊

61
临床特点 收缩顶峰状态有短时持续而呈现特殊的姿势 异常运动的方向及模式较为恒定 随意运动时加重,可呈进行性发展 常因紧张、生气、疲劳而加重
感觉诡计(sensory tricks)
")
62
临床特点 Dystonia持续性、模式化、特定条件下加重的特点使其有别于: 肌阵挛 抽动症 舞蹈病 震颤 痉挛状态
痉挛状态 但Dystonia可伴有其他形式的不自主运动

63
抽动症(Tics) 感觉驱动 暂时可被抑制-有鉴别意义 控制后的放松时加重-抽动释放 紧张、劳累时加重,注意力集中或娱乐时减轻
慢性波动性病程 睡眠中可以持续存在 可伴有OCD、ADHD、自残行为

64
重 点 运动障碍病的概念、分类及常见疾病 帕金森病的病因、发病机制 帕金森病的诊断步骤 帕金森综合症 帕金森病的治疗及并发症处理

Similar presentations



正确 2 )多词 3 )缺词 4 )错词 删除 补漏 更正 “1126” 原则 “1225” 原则 “1117” 原则.>")
家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")






 河南中医学院第一附属医院 杜正光>")








>")