Download presentation
Presentation is loading. Please wait.

1
戒菸藥物的最新進展 黃盈翔醫師 成大醫院家庭醫學部

2
香菸 吸菸 菸害 香煙 抽菸 煙害

6
歷年成人吸菸率 2009年新法上路 菸品健康福利捐20元 1997年菸害防制法通過並實施 2002年開徵菸品健康福利捐5元
2006年菸品健康福利捐10元 1973至1996年資料來源為菸酒公賣局調查資料。 1999年資料來源為李蘭教授調查資料。 2002年資料來源為國民健康局「台灣地區九十一年國民健康促進知識、態度與行為調查」 年資料來源為國民健康局「成人吸菸行為電話調查」。 ** 2002、 年吸菸率係指目前每日吸菸及偶爾吸菸,且迄今吸菸超過100支

8
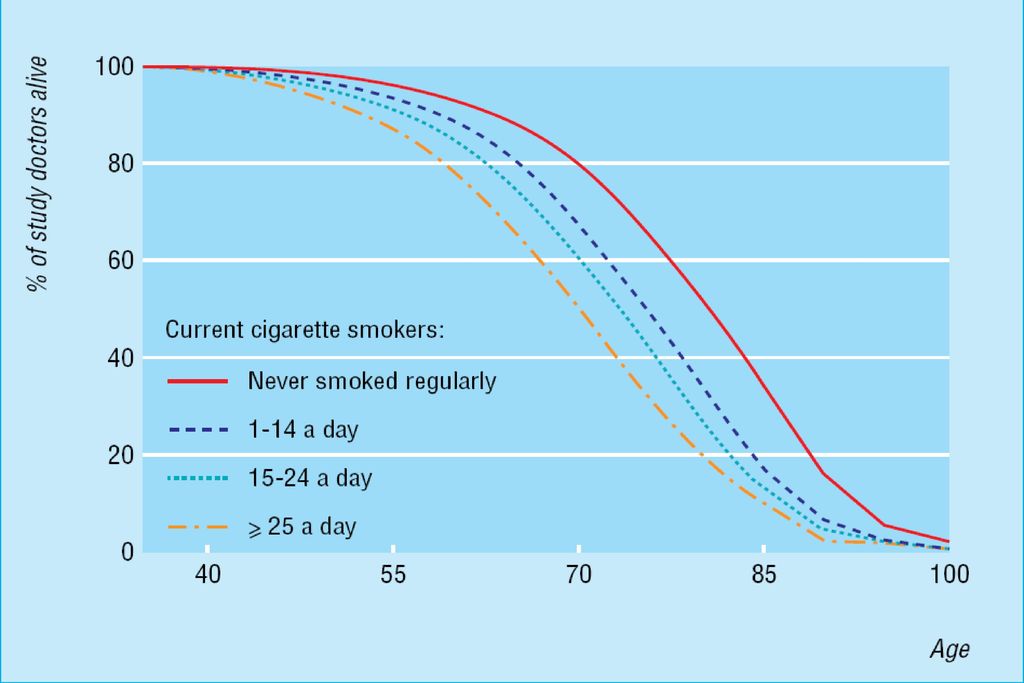
吸一根菸,少活七分鐘 吸一根菸,少活七分鐘

10
吸菸縮短你的壽命 7分鐘/1根菸 140分/天 51,100分/年 35.49 天/年 吸菸的人一年只有11個月

11
戒菸的方法 有效的方法 醫師勸導戒菸 個別行為諮商 團體行為治療 電話諮商 尼古丁補充治療(NRT)
藥物治療:Bupropion, Varenicline 不具療效或未定論方法 自助式戒菸法 同伴的鼓勵 嫌物性行為療法 公共場所禁菸 催眠治療 針灸治療 抗焦慮藥物

12
各種戒菸方式的最高成功率 12 個月後的戒菸 % 單靠意志力 3% * 自助式教材 4% * 短時間的一般科醫師忠告 5% **
單靠意志力 3% * 自助式教材 4% * 短時間的一般科醫師忠告 5% ** 短時間的一般科醫師忠告 & 從藥房購買的尼古丁替代治療 戒菸門診 10% * 戒菸門診 &尼古丁替代治療 20% * 單靠意志力是最常被使用的方法;然而,如幻燈片顯示,它的效果最差。1 自助式教材是很實用的資料來源,但是效果如何並沒有被廣泛的研究過。 一般科醫師的忠告能增加戒菸率 — 即使只是非常短時間的忠告,就能多增加 2% 的抽菸者停止抽菸 (超過沒有介入治療),12 個月的戒菸率能提升到 5%。1,2 一般來說,整體的介入越多,成功的可能性就越大。 因此,使用藥物治療再加上一些方式的積極支持,比單獨使用任何方式,有較高的戒菸率,所以是幫助戒菸者停止抽菸的最有效戒菸方法。1 皇家醫師學會的菸草顧問小組,最近也開始支持使用這一種互補的方法來治療尼古丁成癮。3 6% * * Parrot et al, Thorax ** Richmond, Int J Tuberc Lung Dis 1999. 1. Parrott S, Godfrey C, Raw M et al. Thorax 1998; 53 (Suppl 5): S1-38. 2. Richmond, RL. Int J Tuberc Lung Dis 1999; 3: 3. Royal College of Physicians of London. Nicotine addiction in Britain: A report of the Tobacco Advisory Group of the Royal College of Physicians. London: Royal College of Physicians, 2000.
,12 個月的戒菸率能提升到 5%。1,2. 一般來說,整體的介入越多,成功的可能性就越大。 因此,使用藥物治療再加上一些方式的積極支持,比單獨使用任何方式,有較高的戒菸率,所以是幫助戒菸者停止抽菸的最有效戒菸方法。1 皇家醫師學會的菸草顧問小組,最近也開始支持使用這一種互補的方法來治療尼古丁成癮。3. 6% * * Parrot et al, Thorax ** Richmond, Int J Tuberc Lung Dis Parrott S, Godfrey C, Raw M et al. Thorax 1998; 53 (Suppl 5): S Richmond, RL. Int J Tuberc Lung Dis 1999; 3: Royal College of Physicians of London. Nicotine addiction in Britain: A report of the Tobacco Advisory Group of the Royal College of Physicians. London: Royal College of Physicians,")
13
醫師介入 Cochrane Collaboration and published in The Cochrane Library
Comparison N Trials Participants Pooled RR* (95% CI) Physician advice1 Advise vs no advice (usual care) Minimal intervention Intensive intervention Intensive vs minimal advice 26 17 11 15 >22,240 13,724 8,516 >9,775 1.76 (1.58, 1.95) 1.66 (1.42–1.94) 1.84 (1.60, 2.13) 1.37 (1.20–1.56) Cochrane Collaboration and published in The Cochrane Library 2008, Issue 4.. Physician advice for smoking cessation (Review)
 Physician advice1. Advise vs no advice (usual care) Minimal intervention Intensive intervention. Intensive vs minimal advice >22, ,724. 8,516. >9, (1.58, 1.95) 1.66 (1.42–1.94) 1.84 (1.60, 2.13) 1.37 (1.20–1.56) Cochrane Collaboration and published in The Cochrane Library. 2008, Issue 4.. Physician advice for smoking cessation (Review)")
14
護士介入 Nursing intervention
Comparison N Trials Participants Pooled RR* (95% CI) Nursing intervention nursing intervention vs control(usual care) High intensity intervention Low intensity intervention 31 24 7 >15,000 11189 4016 1.28 (1.18–1.38) 1.28 (1.18–1.39) 1.27 (0.99, 1.62) Cochrane Collaboration and published in The Cochrane Library 2009, Issue 1.. Nursing interventions for smoking cessation (Review)
 Nursing intervention. nursing intervention vs control(usual care) High intensity intervention. Low intensity intervention >15, (1.18–1.38) 1.28 (1.18–1.39) 1.27 (0.99, 1.62) Cochrane Collaboration and published in The Cochrane Library. 2009, Issue 1.. Nursing interventions for smoking cessation (Review)")
15
社區藥局藥師介入 Comparison N Trials Participants Pooled RR* (95% CI) Community pharmacy personnel interventions Maguire 2001 Sinclair 1998 1 484 492 5.23 (2.25–12.15) 1.62 (0.92– 2.85) Cochrane Collaboration and published in The Cochrane Library 2008, Issue 4.. Community pharmacy personnel interventions for smoking cessation (Review)
 1.62 (0.92– 2.85) Cochrane Collaboration and published in The Cochrane Library 2008, Issue 4.. Community pharmacy personnel interventions for smoking cessation (Review)")
16
戒菸之藥物療法 尼古丁補充治療(NRT) Bupropion(ZybanR)
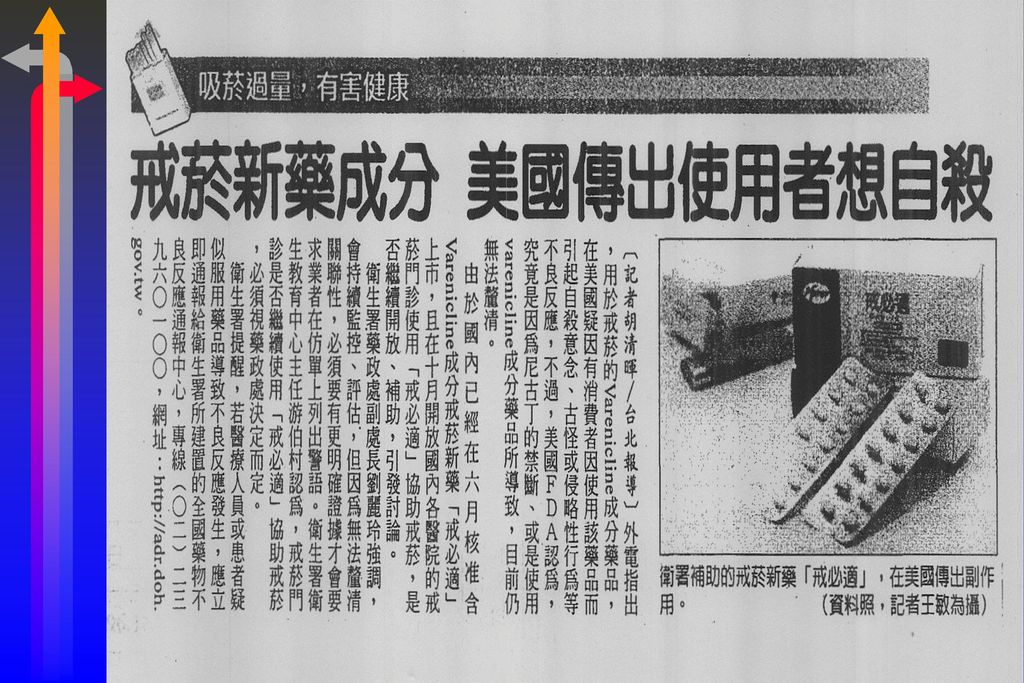
尼古丁經皮貼片(transdermal patch):定量式給藥 尼古丁口嚼錠(gum) 尼古丁噴霧劑(nasal spray) 尼古丁吸入劑(inhaler) 尼古丁舌下片(lozenge) 口含微錠(microtab)(歐洲、澳洲) Bupropion(ZybanR) Varenicline(ChampixR):200707衛生署核可 Rimbonabant(AcompliaR):已下市 戒菸疫苗(Phase II/III trial) **口嚼錠1984 by FDA, 貼片1992 by FDA, 鼻噴劑1996 by FDA, 吸入劑1998 by FDA **可以合併使用上列方式 ( TVBS)想戒煙的癮君子可要注意以下的訊息!美國今天公布戒菸疫苗的初步實驗結果,發現高達57% 接受檢測的人,在注射疫苗之後輕鬆戒菸成功,專家表示,在進一步實驗後,戒菸疫苗預計在2007年問世。 這項最新的實驗結果顯示,戒菸疫苗在人體內形成反尼古丁抗體(Anti-nicotine Ab),大幅降低癮君子的菸癮,5成7接受檢測的人,注射戒菸疫苗後戒菸成功,不過部分受測者卻發生身體不適的副作用 。 專家表示,戒菸疫苗需要經過進一步的測試,來降低副作用的產生,但初步實驗結果,令人感到十分滿意,戒菸疫苗也預計在2年後問世。
:定量式給藥. 尼古丁口嚼錠(gum) 尼古丁噴霧劑(nasal spray) 尼古丁吸入劑(inhaler) 尼古丁舌下片(lozenge) 口含微錠(microtab)(歐洲、澳洲) Bupropion(ZybanR) Varenicline(ChampixR):200707衛生署核可. Rimbonabant(AcompliaR):已下市. 戒菸疫苗(Phase II/III trial) **口嚼錠1984 by FDA, 貼片1992 by FDA, 鼻噴劑1996 by FDA, 吸入劑1998 by FDA. **可以合併使用上列方式. ( TVBS)想戒煙的癮君子可要注意以下的訊息!美國今天公布戒菸疫苗的初步實驗結果,發現高達57% 接受檢測的人,在注射疫苗之後輕鬆戒菸成功,專家表示,在進一步實驗後,戒菸疫苗預計在2007年問世。 這項最新的實驗結果顯示,戒菸疫苗在人體內形成反尼古丁抗體(Anti-nicotine Ab),大幅降低癮君子的菸癮,5成7接受檢測的人,注射戒菸疫苗後戒菸成功,不過部分受測者卻發生身體不適的副作用 。 專家表示,戒菸疫苗需要經過進一步的測試,來降低副作用的產生,但初步實驗結果,令人感到十分滿意,戒菸疫苗也預計在2年後問世。")
18
Forms of NRT – dosage and use
Gum Up to 15 or 25 sticks/day 2mg or 4mg Patch 16- or 24-hour patches 3 strengths Sublingual tablets Up to 40 tablets/day 2mg Lozenges Min 9, max 15 lozenges/day Inhalator 6–12 cartridges/day Nasal spray Up to 64 sprays/day 18

19
正確使用很重要

20
尼古丁貼片

21
尼古丁經皮膚貼片(克菸)
")
22
若1天吸菸超過20知者,建議用最高劑量(30號)開始給予
開始給予")
23
克菸貼片 療程及劑量的選擇 若1天吸菸超過20知者,建議用最高劑量(30號)開始給予
開始給予")
24
尼古丁經皮貼片的使用 每天清晨時在無毛且乾淨乾燥沒有傷口的皮膚上貼一片
25
尼古丁貼片 尼古丁貼片 21mg、14mg、7mg 貼在腰部以上皮膚, 透過皮膚吸收 2-3小時 局部皮膚會受到刺激
劑量 21mg、14mg、7mg 使用方式 貼在腰部以上皮膚, 透過皮膚吸收 藥效出現時間 2-3小時 注意事項 局部皮膚會受到刺激 睡眠障礙者容易產生失眠情況 無法應付臨時突發的菸癮

26
16 V.S. 24 小時貼片 長期使用效果一樣,沒有優劣之分 24小時貼既能避免早晨戒斷症候,適合早晨一起床就吸菸的人
24小時貼劑順從性較高,撕和貼的時間一樣 16小時貼劑使不舒服的症狀控制在晚上,而且比較不會產生耐量性 16小時貼劑比較不會影響睡眠和作夢 24小時貼劑會產生 vivid dream

27
24小時尼古丁貼片使用須知 於使用後4-8小時逐漸達到最高濃度,約2-3天達到穩定濃度
每天洗完澡後使用,到第二天要洗澡前撕下(或每天早晨使用) 最好貼在上臂、軀幹上(頸部與膝部間之無毛區域),同一個部位貼過後必須7天後再貼
 最好貼在上臂、軀幹上(頸部與膝部間之無毛區域),同一個部位貼過後必須7天後再貼.")
28
尼古丁貼片的副作用 皮膚過敏(25-50%) 下痢、消化不良、肌肉骨骼痛(3-9%) 失眠(1-3%) 因副作用停用貼片者(6-7%)
不容易入睡 可以在睡前停用,或使用16小時貼片 通常繼續使用會改善 因副作用停用貼片者(6-7%)
")
30
咀嚼到有辣味出來就含於頰部及牙齦間,等沒辣味時再嚼
尼古丁口嚼錠 每天早晨起床後使用一次後,每 小時一錠 咀嚼到有辣味出來就含於頰部及牙齦間,等沒辣味時再嚼 **和一般口香糖不同,咀嚼15下左右有辣味時,應將嚼片推置於臉頰,等到沒有辣味時(約3分鐘)再重新咀嚼,如此反覆,約可使用30分鐘。再加上意志力,可維持1- 1.5小時 **使用後30分鐘達到最高濃度,2-3小時後恢復正常 **使用前、後15分鐘避免喝飲料或吃餐點 **副作用;苦味; 打嗝、氣脹、噁心(吞入尼古丁);下頷關節酸痛; ----通常繼續使用一週以後消失
再重新咀嚼,如此反覆,約可使用30分鐘。再加上意志力,可維持1- 1.5小時. **使用後30分鐘達到最高濃度,2-3小時後恢復正常. **使用前、後15分鐘避免喝飲料或吃餐點. **副作用;苦味; 打嗝、氣脹、噁心(吞入尼古丁);下頷關節酸痛; ----通常繼續使用一週以後消失.")
31
尼古丁口嚼錠 尼古丁口嚼錠如Nicorette為可咀嚼的口香糖型式(2 mg 1984; 4mg 1990)
劑型可分為 4mg: >25支/day(1.5 mg) 2mg: ≦24支/day(0.8 mg) 克菸咀嚼錠、尼古清口嚼錠 起始劑量每日10-15錠;維持劑量 5-8錠/天 每1-2小時嚼一顆,max 24 pieces/day 20-30 分,血漿中達最高濃度 Initial 6 weeks, then taper 6 weeks
 2mg: ≦24支/day(0.8 mg) 克菸咀嚼錠、尼古清口嚼錠. 起始劑量每日10-15錠;維持劑量 5-8錠/天. 每1-2小時嚼一顆,max 24 pieces/day 分,血漿中達最高濃度. Initial 6 weeks, then taper 6 weeks.")
32
尼古丁吸入劑

33
尼古丁吸入劑 尼古丁吸入劑 劑量 10mg/藥液匣 適用對象 不習慣手上沒菸的戒菸者 使用方式 注意事項 將藥匣裝至吸入器內,
有40%懷念手中握有香菸的感覺而戒菸失敗 使用方式 將藥匣裝至吸入器內, 吸一口後 含在口中 由 口腔黏膜吸收 注意事項 吸氣時 小口吸 避免喉嚨刺激

34
不習慣手上沒有菸的感覺

35
不習慣手上沒有菸的感覺

36
尼古丁吸入劑 安裝方式(實際演練)
")
37
尼古丁吸入劑 使用方式 使用技巧 注意事項 輕輕吸, 含在口中, 過3~5秒再吐出 每次吸2~3口 每支藥液匣可連續使用20分鐘
藥液匣放入吸入器後, 即使沒有使用也需在12小時後更換

38
尼古丁吸入劑 建議用量 每日建議用量 *簡易用量換算:每日抽菸量除以4 每個藥液匣可以吸超過80口 使用規則
每天抽菸量 1-24支 25-32支 33-40支 >40支 每天建議藥液匣用量 6 8 10 12 *簡易用量換算:每日抽菸量除以4 每個藥液匣可以吸超過80口 使用規則 戒菸初期 1-12星期 戒菸中期 13-14星期 戒菸後期 15-16星期 每天使用6-12個藥液匣 每天使用3-6個藥液匣 每天使用1-3個藥液匣 建議使用時間可長達6個月,但後3個月需減少劑量

39
尼古丁口腔吸入劑副作用 副作用輕微,繼續使用並熟悉技巧後,發生頻率就會下降 常見副作用 口腔與喉嚨刺激 咳嗽與鼻炎

40
Efficacy of Nicotine Replacement Therapy (NRT)
Comparison N Trials Participants Pooled RR (95% CI) Gum 53 19,090 1.43 (1.33–1.53) Patch 41 18,237 1.66 (1.53–1.81) Nasal spray 4 887 2.02 (1.49–3.73) Inhaler 976 1.90 (1.36–2.45) Tablets/lozenges 6 3190 2.00 (1.63–2.45) Combination vs single type 7 3202 1.35 (1.11–1.63) Any NRT vs control 111 43,040 1.58 (1.50–1.66) 尼古丁替代療法 (NRT) 之療效 研究顯示, 所有的尼古丁替代療法 (NRT) 皆可增加戒菸的成功率, 且不同療法之療效無顯著差異. Key Point All types of NRT increase the odds of quitting, with little difference among methods. Cochrane Database of Systematic Reviews, Issue 1, 2009 (Status in this issue: Unchanged, commented)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. DOI: / CD pub3
 Gum , (1.33–1.53) Patch , (1.53–1.81) Nasal spray (1.49–3.73) Inhaler (1.36–2.45) Tablets/lozenges (1.63–2.45) Combination vs single type (1.11–1.63) Any NRT vs control , (1.50–1.66) 尼古丁替代療法 (NRT) 之療效. 研究顯示, 所有的尼古丁替代療法 (NRT) 皆可增加戒菸的成功率, 且不同療法之療效無顯著差異. Key Point. All types of NRT increase the odds of quitting, with little difference among methods. Cochrane Database of Systematic Reviews, Issue 1, 2009 (Status in this issue: Unchanged, commented)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. DOI: / CD pub3.")
41
血漿尼古丁濃度 – 香菸和尼古丁替代治療之間的比較
血漿尼古丁濃度 – 香菸和尼古丁替代治療之間的比較 香菸(nicotine delivery, 1-2 mg) 口香糖(nicotine delivery, 4 mg) 噴劑(nicotine delivery, 1 mg) 貼片Transdermal patch Sweeney/pg 456/figure 1 香菸 口香糖 Plasma Nicotine Concentration (μg/L) 尼古丁替代療法 (NRT)- 使用香菸及NRT治療, 尼古丁濃度及時間之比較 結果顯示, NRT無法像吸菸如此快速的將尼古丁分布至體內 Key Point Most NRT methods typically don’t deliver nicotine as rapidly and at the same level as cigarette smoking. Background No individual NRT currently available when administered as indicated matches the intensity and pattern of nicotine delivery of a cigarette, which delivers high levels of nicotine within minutes of smoking that gradually taper down over time. A slow delivery system, such as that of the nicotine patch, provides a more constant concentration of nicotine in the plasma to relieve cravings and tobacco withdrawal symptoms over time, whereas delivery methods that are faster acting, such as nasal spray or gum, can be used on demand for immediate relief of breakthrough cravings. Reference 1. Sweeney CT, Fant RV, Fagerström KO, et al. Combination nicotine replacement therapy for smoking cessation: rationale, efficacy and tolerability. CNS Drugs. 2001;15:453–467. 噴劑 貼片 Sweeney/pg 453/abstract; pg 455/col 2/¶3; pg 456/ col 1/¶1; figure 1 Time post-administration (minutes) 1. Sweeney CT, et al. CNS Drugs. 2001;15:
 口香糖(nicotine delivery, 4 mg) 噴劑(nicotine delivery, 1 mg) 貼片Transdermal patch. Sweeney/pg 456/figure 1. 香菸. 口香糖. Plasma Nicotine Concentration (μg/L) 尼古丁替代療法 (NRT)- 使用香菸及NRT治療, 尼古丁濃度及時間之比較. 結果顯示, NRT無法像吸菸如此快速的將尼古丁分布至體內. Key Point. Most NRT methods typically don’t deliver nicotine as rapidly and at the same level as cigarette smoking. Background. No individual NRT currently available when administered as indicated matches the intensity and pattern of nicotine delivery of a cigarette, which delivers high levels of nicotine within minutes of smoking that gradually taper down over time. A slow delivery system, such as that of the nicotine patch, provides a more constant concentration of nicotine in the plasma to relieve cravings and tobacco withdrawal symptoms over time, whereas delivery methods that are faster acting, such as nasal spray or gum, can be used on demand for immediate relief of breakthrough cravings. Reference. 1. Sweeney CT, Fant RV, Fagerström KO, et al. Combination nicotine replacement therapy for smoking cessation: rationale, efficacy and tolerability. CNS Drugs. 2001;15:453–467. 噴劑. 貼片. Sweeney/pg 453/abstract; pg 455/col 2/¶3; pg 456/ col 1/¶1; figure 1. Time post-administration (minutes) 1. Sweeney CT, et al. CNS Drugs. 2001;15:")
42
尼古丁替代療法(NRT)使用禁忌 不穩定心血管疾病患者 難控制的高血壓 小於18歲者 懷孕或哺乳婦女 不穩定心絞痛病人 急性心肌梗塞病人
嚴重心律不整患者 難控制的高血壓 小於18歲者 懷孕或哺乳婦女

43
尼古丁替代療法劑型比較 藥品 吸入劑 咀嚼錠 貼片 口含錠 療程 3-6個月(建議不超過一年) 成功率 20-30%(藥物+諮詢) 使用
方式 淺吸即可,一顆藥液匣 可連續使用20分鐘 不可像口香糖一樣連續咀嚼,需把握嚼-停-嚼原則藥物,置於口腔兩側,30分鐘後丟棄。 睡前更換新貼片,太早更換易導致精神亢奮,難以入眠 口頰兩側交換移動至溶解為止 ,一顆口含錠使用約20~30分鐘 優點 藥效快 可滿足戒菸時的口慾與手慾 適用所有的吸菸者 癮君子接受度高 利用咀嚼的動作滿足戒菸時的口慾 使用方便 可持續釋放相同濃度的尼古丁 使用方便,含著即可 注意 事項 吸太用力易有咳嗽等輕微症狀 過度咀嚼易引起臉頰酸痛、打嗝、胃部不適等症狀 牙齒不好者不適用 藥效來的比較慢 尼古丁劑量無法調整 易引起失眠 皮膚易過敏者不適用 易刺激口腔傷口 喉嚨痛、吞嚥困難、想吐或嘔吐 口感黏黏的,不喜口腔黏滑者不適

44
非尼古丁替代療法

45
Bupropion-SR (Zyban, Wellbutrion)
1996年,美國FDA核准使用 可合併NRT使用 副作用:癲癇(1/1000)、過敏、紅疹、皮膚癢、噁心、失眠、口乾 有肝腎功能異常者,減量使用 懷孕或哺乳婦女,不建議使用。小於18歲者安全性待確立 Initial: 150mg QD x 3 days, then 150mg BID
、過敏、紅疹、皮膚癢、噁心、失眠、口乾. 有肝腎功能異常者,減量使用. 懷孕或哺乳婦女,不建議使用。小於18歲者安全性待確立. Initial: 150mg QD x 3 days, then 150mg BID.")
46
Zyban (Bupropion) 效果與NRT相似 成功率約為對照組之2倍 戒菸前一周即應服用,連續服用7週
可減少因戒菸造成的體重增加,但機制不明。

47
Bupropion使用方法 病患應於開始戒菸前1–2週開始使用。 前3天:每天早上150mg。 第4天起:150mg每天兩次。
47

48
Bupropion禁忌與副作用 懷孕─不可用藥。FDA 懷孕分類 C;授乳者未有評估報告。 心血管疾病─通常忍受度良好,偶而有高血壓的報告
副作用─最常見的副作用是失眠(35–40%)與口乾(10%) 禁忌─有癲癇病史或飲食異常(eating disorders)、正在吃另一種bupropion或過去14天有用MAO抑制劑不可使用 48
與口乾(10%) 禁忌─有癲癇病史或飲食異常(eating disorders)、正在吃另一種bupropion或過去14天有用MAO抑制劑不可使用. 48.")
49
Antidepressants for Smoking Cessation
Comparison N Trials N Participants Pooled RR (95% CI) Bupropion vs placebo 36 11,140 1.69 (1.53–1.85) Bupropion vs NRT 6 1,106 1.23 (0.67–2.26) Limited or no evidence of long-term benefit with other antidepressants, including fluoxetine, sertraline, paroxetine, moclobemide, and venlafaxine, . Key Point Data from multiple trials have outlined the efficacy of specific antidepressant therapy (bupropion, nortriptyline) for quitting smoking. Background Multiple trials have been conducted investigating antidepressant therapy, including bupropion, nortriptyline, and several selective serotonin-reuptake inhibitors (SSRIs), for quitting smoking. A Cochrane review of the literature found 24 trials studied the use of bupropion therapy either alone or in combination with other methods (eg, NRT). Analysis of data from 19 trials that investigated bupropion monotherapy resulted in an OR of 2.06 for success in quitting smoking. Two trials of bupropion plus NRT patch treatment compared with placebo yielded an OR of only The combined OR for all trials of bupropion versus placebo was Compared with bupropion, fewer trials have been conducted with nortriptyline (24 vs 6, respectively), and in the whole of the published literature, it has only been tested for quitting smoking in approximately 500 smokers.1,2 A Cochrane analysis of all available data revealed an OR of 2.14 for quitting smoking. This increased slightly to 2.79 when only the trials of nortriptyline monotherapy were included in the analysis.1 There is limited or no evidence of long-term benefit with other antidepressants including the monoamine oxidase inhibitor, moclobemide, the atypical, venlafaxine, or the selective serotonin reuptake inhibitors, fluoxetine, sertraline, and paroxetine.1 References 1. Hughes J, Stead L, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD 2. Hughes JR, Stead LF, Lancaster T. Nortriptyline for smoking cessation: a review. Nicotine Tob Res. 2005;7:491–499. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database of Systematic Reviews 2007,Issue 1.
 Bupropion vs placebo , (1.53–1.85) Bupropion vs NRT. 6. 1, (0.67–2.26) Limited or no evidence of long-term benefit with other antidepressants, including fluoxetine, sertraline, paroxetine, moclobemide, and venlafaxine, . Key Point. Data from multiple trials have outlined the efficacy of specific antidepressant therapy (bupropion, nortriptyline) for quitting smoking. Background. Multiple trials have been conducted investigating antidepressant therapy, including bupropion, nortriptyline, and several selective serotonin-reuptake inhibitors (SSRIs), for quitting smoking. A Cochrane review of the literature found 24 trials studied the use of bupropion therapy either alone or in combination with other methods (eg, NRT). Analysis of data from 19 trials that investigated bupropion monotherapy resulted in an OR of 2.06 for success in quitting smoking. Two trials of bupropion plus NRT patch treatment compared with placebo yielded an OR of only The combined OR for all trials of bupropion versus placebo was Compared with bupropion, fewer trials have been conducted with nortriptyline (24 vs 6, respectively), and in the whole of the published literature, it has only been tested for quitting smoking in approximately 500 smokers.1,2 A Cochrane analysis of all available data revealed an OR of 2.14 for quitting smoking. This increased slightly to 2.79 when only the trials of nortriptyline monotherapy were included in the analysis.1. There is limited or no evidence of long-term benefit with other antidepressants including the monoamine oxidase inhibitor, moclobemide, the atypical, venlafaxine, or the selective serotonin reuptake inhibitors, fluoxetine, sertraline, and paroxetine.1. References. 1. Hughes J, Stead L, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD Hughes JR, Stead LF, Lancaster T. Nortriptyline for smoking cessation: a review. Nicotine Tob Res. 2005;7:491–499. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database of Systematic Reviews 2007,Issue 1.")
50
為什麼吸菸會上癮? 尼古丁在中樞神經系統之作用機轉
1/Picciotto, p. S121, para 1 尼古丁在中樞神經系統之作用機轉 a4 b2 4b2 Nicotinic Receptor 1/Picciotto, p. S121, para 1 尼古丁在中樞神經系統之作用機轉 尼古丁在中樞神經系統優先與尼古丁乙醯膽鹼 (nA Ch) 受器結合; 主要與為位於 Ventral Tegmental Area (VTA) 的42尼古丁受器結合 當與42尼古丁受器結合之後, 造成 Nucleus Accumbens (nAcc) 中 dopamine 的釋放, 進而產生吸菸的快感 Key Point Nicotine stimulates dopamine release in areas of the brain which is believed to result in the reward and satisfaction effect associated with smoking. Background After inhalation, nicotine preferentially binds to nicotinic acetylcholinergic (nACh) receptors located in the mesolimbic-dopamine system of the brain within a matter of seconds. Nicotine specifically activates 4β2 nicotinic receptors in the Ventral Tegmental Area (VTA) causing an immediate dopamine release at the Nucleus Accumbens (nAcc).1 The dopamine release is believed to be a key component of the reward circuitry associated with cigarette smoking.1 Reference 1. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S 尼古丁在中樞神經系統優先與尼古丁受器結合; 當與尼古丁受器結合之後, 造成 dopamine 的釋放, 進而產生吸菸的快感
 受器結合; 主要與為位於 Ventral Tegmental Area (VTA) 的42尼古丁受器結合. 當與42尼古丁受器結合之後, 造成 Nucleus Accumbens (nAcc) 中 dopamine 的釋放, 進而產生吸菸的快感. Key Point. Nicotine stimulates dopamine release in areas of the brain which is believed to result in the reward and satisfaction effect associated with smoking. Background. After inhalation, nicotine preferentially binds to nicotinic acetylcholinergic (nACh) receptors located in the mesolimbic-dopamine system of the brain within a matter of seconds. Nicotine specifically activates 4β2 nicotinic receptors in the Ventral Tegmental Area (VTA) causing an immediate dopamine release at the Nucleus Accumbens (nAcc).1 The dopamine release is believed to be a key component of the reward circuitry associated with cigarette smoking.1. Reference. 1. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S 尼古丁在中樞神經系統優先與尼古丁受器結合; 當與尼古丁受器結合之後, 造成 dopamine 的釋放, 進而產生吸菸的快感.")
51
戒必適® (Champix)® 0.5mg 11顆/盒 1mg 14顆/盒 第4~7天 第1~3天 第8天~12週 51 51
® 0.5mg 11顆/盒 1mg 14顆/盒 第4~7天 第1~3天 第8天~12週 51 51")
52
Champix® (varenicline): A Highly Selective 42 Receptor Partial Agonist
Nicotine Champix® Champix (varenicline): 具高選擇性之42受器部份致效劑 (左圖) 當尼古丁與42受器結合時, 會導致 dopamine 的釋放 (右圖) Champix 為42受器部份致效劑, 為一同時具有致效作用及拮抗作用之藥品. 此一特性使得 Champix 與受器結合後釋放的dopamine較少, 且同一時間仍能防止尼古丁與 42受器結合. Key Point Champix™ (varenicline) was deliberately designed for the 42 receptor, as an 42 nicotinic receptor partial agonist (with dual agonist and antagonist properties) and physically prevents nicotine from binding as an aid in smoking cessation. Binding of nicotine at the 42 nicotinic receptor in the VTA is believed to cause release of dopamine at the nAcc Champix is an 42 nicotinic receptor partial agonist, a compound with dual agonist and antagonist activities. This is believed to result in both a lesser amount of dopamine release from the VTA at the nAcc as well as the prevention of nicotine binding at the 42 receptors. 1. Coe JW et al. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco Prague, Czech Republic. 2. Picciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S121-S125.
: 具高選擇性之42受器部份致效劑. (左圖) 當尼古丁與42受器結合時, 會導致 dopamine 的釋放. (右圖) Champix 為42受器部份致效劑, 為一同時具有致效作用及拮抗作用之藥品. 此一特性使得 Champix 與受器結合後釋放的dopamine較少, 且同一時間仍能防止尼古丁與 42受器結合. Key Point. Champix™ (varenicline) was deliberately designed for the 42 receptor, as an 42 nicotinic receptor partial agonist (with dual agonist and antagonist properties) and physically prevents nicotine from binding as an aid in smoking cessation. Binding of nicotine at the 42 nicotinic receptor in the VTA is believed to cause release of dopamine at the nAcc. Champix is an 42 nicotinic receptor partial agonist, a compound with dual agonist and antagonist activities. This is believed to result in both a lesser amount of dopamine release from the VTA at the nAcc as well as the prevention of nicotine binding at the 42 receptors. 1. Coe JW et al. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco Prague, Czech Republic. 2. Picciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S121-S125.")
53
Varenicline Mechanism of Action: Efficacy for Tobacco Dependence
Efficacy of varenicline in tobacco dependence Believed to result from partial agonist activity at the 42 nicotinic receptor By preventing binding of nicotine, varenicline Reduces craving and withdrawal symptoms (agonist activity) Produces a reduction of the rewarding and reinforcing effects of smoking (antagonist activity) The most frequently reported adverse events (>10%) with varenicline were nausea(30%), headache, insomnia, and abnormal dreams. Champix 的作用機轉 Champix 的戒菸療效來自於對42受器的部份致效作用 阻斷尼古丁與受器結合, 故 Champix 可以: 減少對吸菸的渴求及戒斷症狀 (致效作用) 降低抽菸的滿足感及感官強化效果 (拮抗作用) 使用Champix較常見的副作用為噁心、頭痛、失眠以及異夢 Key point The efficacy of varenicline in smoking cessation results from its partial agonist activity at the 42 nicotinic receptor. By physically blocking the binding of nicotine, varenicline’s partial agonist activity produces an effect sufficient to alleviate symptoms of craving and withdrawal (agonist activity) while simultaneously resulting in rewarding and reinforcing of the effects of smoking (antagonist activity). Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK
 Produces a reduction of the rewarding and reinforcing effects of smoking (antagonist activity) The most frequently reported adverse events (>10%) with varenicline were nausea(30%), headache, insomnia, and abnormal dreams. Champix 的作用機轉. Champix 的戒菸療效來自於對42受器的部份致效作用. 阻斷尼古丁與受器結合, 故 Champix 可以: 減少對吸菸的渴求及戒斷症狀 (致效作用) 降低抽菸的滿足感及感官強化效果 (拮抗作用) 使用Champix較常見的副作用為噁心、頭痛、失眠以及異夢. Key point. The efficacy of varenicline in smoking cessation results from its partial agonist activity at the 42 nicotinic receptor. By physically blocking the binding of nicotine, varenicline’s partial agonist activity produces an effect sufficient to alleviate symptoms of craving and withdrawal (agonist activity) while simultaneously resulting in rewarding and reinforcing of the effects of smoking (antagonist activity). Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK")
54
試驗設計 藥物治療期 非藥物治療期 Varenicline 1 mg BID* Bupropion 150 mg BID* Placebo
1/Jorenby/p. 56/abstract; p. 57 col 2/¶1,2; col 3/¶3; p. 58/col/1/¶3,4 Varenicline 1 mg BID* Bupropion 150 mg BID* Placebo 2/Gonzales/p. 48/col 2/¶3; col 3/¶1,2,3 收錄開始 隨機分配 第12週 3/PI/p. 9/¶7 第52週 藥物治療期 非藥物治療期 B W W W W W W W W W W W W L W W W W W W W W W W W Key Point The two Phase 3 studies included 12 weeks of active treatment with non-pharmacologic follow-up for 40 weeks. Background Patients enrolled in the two Phase 3 studies were screened via a telephone interview and 2 clinic visits.1 Target quit date was set for 8 days after the first visit (week 1).1,2 Patients were randomized to receive either varenicline titrated as 0.5 mg once daily for days 1 to 3, 0.5 mg twice daily for days 4 to 7, then 1.0 mg twice daily; bupropion SR titrated as 150 mg once daily for days 1 to 3, then 150 mg twice daily; or placebo for 12 weeks.1-3 This active-treatment period was followed by a 40-week off-treatment period, for a total study duration of 52 weeks. During the follow-up period, patients visited the clinic on weeks 13, 24, 36, 44, and 52. During these visits, patients received brief (≤10 minutes) smoking cessation counseling following recommendations in the Public Health Service Clinical Practice Guideline,1,2 and cigarette/tobacco use, vital signs, expired carbon monoxide, and use of smoking cessation medications were assessed. For weeks 16, 20, 28, 32, 40, and 48, patients were contacted by telephone, and use of tobacco and smoking cessation medications was assessed.1,2 References 1. Jorenby DE, Hays JT, Rigotti NA, et al; varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA. 2006;296:56-63. 2. Gonzales D, Rennard SI, Nides M, et al; varenicline Phase 3 Study Group. varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA. 2006;296:47-55. 3. Chantix package insert. Pfizer Labs, a division of Pfizer Inc., New York, NY, USA. 4. Fiore MC, et al. US C C C C C C C C C C C C C C T T C T T C T C T C Two identically designed Phase 3 efficacy trials Varenicline 1.0 mg BID vs placebo or bupropion SR150 mg BID 12 weeks of active treatment followed by 40 weeks of non-pharmacologic follow-up 隨機分配 1/Jorenby/p. 56/abstract; p. 57 col 2/¶1,2; col 3/¶3; p. 58/col/1/¶3,4 戒菸日 1/Jorenby/p /study procedures; p 57 col 3/¶3;p58/col/1/¶2 *Titrated during Week 1. BL=baseline; W=week; C=clinic visit; T=telephone contact. 2/Gonzales/p. 48/col 2/¶3; col 3/¶1,2,3 3/PI/p. 9/¶7 4/Fiore/p. 25 ¶3; p 26, 27, Tables 3,4
.1,2 Patients were randomized to receive either varenicline titrated as 0.5 mg once daily for days 1 to 3, 0.5 mg twice daily for days 4 to 7, then 1.0 mg twice daily; bupropion SR titrated as 150 mg once daily for days 1 to 3, then 150 mg twice daily; or placebo for 12 weeks.1-3 This active-treatment period was followed by a 40-week off-treatment period, for a total study duration of 52 weeks. During the follow-up period, patients visited the clinic on weeks 13, 24, 36, 44, and 52. During these visits, patients received brief (≤10 minutes) smoking cessation counseling following recommendations in the Public Health Service Clinical Practice Guideline,1,2 and cigarette/tobacco use, vital signs, expired carbon monoxide, and use of smoking cessation medications were assessed. For weeks 16, 20, 28, 32, 40, and 48, patients were contacted by telephone, and use of tobacco and smoking cessation medications was assessed.1,2. References. 1. Jorenby DE, Hays JT, Rigotti NA, et al; varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA. 2006;296: Gonzales D, Rennard SI, Nides M, et al; varenicline Phase 3 Study Group. varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA. 2006;296: Chantix package insert. Pfizer Labs, a division of Pfizer Inc., New York, NY, USA. 4. Fiore MC, et al. US. C C C C C C C C C C C C C. C T T C T T C T C T C. Two identically designed Phase 3 efficacy trials. Varenicline 1.0 mg BID vs placebo or. bupropion SR150 mg BID. 12 weeks of active treatment followed by. 40 weeks of non-pharmacologic follow-up. 隨機分配. 1/Jorenby/p. 56/abstract; p. 57 col 2/¶1,2; col 3/¶3; p. 58/col/1/¶3,4. 戒菸日. 1/Jorenby/p /study procedures; p 57 col 3/¶3;p58/col/1/¶2. *Titrated during Week 1. BL=baseline; W=week; C=clinic visit; T=telephone contact. 2/Gonzales/p. 48/col 2/¶3; col 3/¶1,2,3. 3/PI/p. 9/¶7. 4/Fiore/p. 25 ¶3; p 26, 27, Tables 3,4.")
55
4-Week Continuous Abstinence (CA) Response Weeks 9–121
在二項研究中, 使用新一型的藥物(Champix)於 9-12 週之持續戒菸率明顯優於使用傳統戒菸藥物或安慰劑 1/Champix Summary of Product doc/p. 7/¶7 /Table Study 1 OR VAR vs Pbo 3.91 P<0.0001 VAR vs BUP 1.96 P<0.0001 Study 2 OR VAR vs Pbo 3.85 P<0.0001 VAR vs BUP 1.89 P<0.0001 60 60 50 50 44.4% 44.0% 40 40 CA Response rate (%) CA Response rate (%) 29.5% 30.0% 30 30 四週 (第9-12週) 持續戒菸反應率: 在二項研究中, 使用Champix於 9-12 週之持續戒菸率明顯優於使用 bupropion 或安慰劑 (placebo). Key Point In both studies, varenicline resulted in continuous abstinence (CA) rates at weeks 9 through 12 that were significantly higher than for placebo or bupropion. Background For the primary end point of carbon monoxide (CO)–confirmed, 4-week CA rates were defined as patient report and exhaled CO <10 ppm. 4-week CA rates with varenicline treatment were significantly higher compared with bupropion treatment or placebo.1 In study 1, 44.4% of participants in the varenicline group were continuously abstinent from smoking during weeks 9 to 12 compared with 29.5% of participants in the bupropion group and 17.7% of participants in the placebo group (both P<0.0001). This translated to an abstinence OR of 3.91 for varenicline vs placebo and an OR of 1.96 versus bupropion.1 Similarly, in study 2, 4-week abstinence rates for varenicline, bupropion, and placebo were 44.0%, 30.0%, and 17.7%, respectively. Varenicline was significantly more effective compared with placebo (OR, 3.85; P<0.0001) and bupropion (OR, 1.89; P<0.0001).1 Subjects were provided with an educational booklet on smoking cessation and received up to 10 minutes of smoking cessation counseling at each clinic visit in accordance with Agency for Healthcare Research and Quality Guidelines. Reference 1. Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK 20 17.7% 20 17.7% 10 10 1/Champix Summary of Product doc/p. 7/¶7/Table VAR 1 mg bid (n=344) BUP 150 mg bid (n=342) Pbo (n=341) VAR 1 mg bid (n=352) BUP 150 mg bid (n=329) Pbo (n=344) VAR=varenicline, Pbo=placebo, BUP=bupropion; OR = Odds ratio. 1. Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK
於 9-12 週之持續戒菸率明顯優於使用傳統戒菸藥物或安慰劑. 1/Champix Summary of Product doc/p. 7/¶7 /Table. Study 1. OR. VAR vs Pbo 3.91 P< VAR vs BUP 1.96 P< Study 2. OR. VAR vs Pbo 3.85 P< VAR vs BUP 1.89 P< % 44.0% CA. Response. rate (%) CA. Response. rate (%) 29.5% 30.0% 四週 (第9-12週) 持續戒菸反應率: 在二項研究中, 使用Champix於 9-12 週之持續戒菸率明顯優於使用 bupropion 或安慰劑 (placebo). Key Point. In both studies, varenicline resulted in continuous abstinence (CA) rates at weeks 9 through 12 that were significantly higher than for placebo or bupropion. Background. For the primary end point of carbon monoxide (CO)–confirmed, 4-week CA rates were defined as patient report and exhaled CO <10 ppm. 4-week CA rates with varenicline treatment were significantly higher compared with bupropion treatment or placebo.1 In study 1, 44.4% of participants in the varenicline group were continuously abstinent from smoking during weeks 9 to 12 compared with 29.5% of participants in the bupropion group and 17.7% of participants in the placebo group (both P<0.0001). This translated to an abstinence OR of 3.91 for varenicline vs placebo and an OR of 1.96 versus bupropion.1 Similarly, in study 2, 4-week abstinence rates for varenicline, bupropion, and placebo were 44.0%, 30.0%, and 17.7%, respectively. Varenicline was significantly more effective compared with placebo (OR, 3.85; P<0.0001) and bupropion (OR, 1.89; P<0.0001).1 Subjects were provided with an educational booklet on smoking cessation and received up to 10 minutes of smoking cessation counseling at each clinic visit in accordance with Agency for Healthcare Research and Quality Guidelines. Reference. 1. Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK % % /Champix Summary of Product doc/p. 7/¶7/Table. VAR 1 mg bid (n=344) BUP 150 mg bid (n=342) Pbo (n=341) VAR 1 mg bid (n=352) BUP 150 mg bid (n=329) Pbo (n=344) VAR=varenicline, Pbo=placebo, BUP=bupropion; OR = Odds ratio. 1. Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK")
56
Continuous Abstinence Rates Wks 9-52
100 OR=3.13 (95% CI 1.97, 4.97) p<0.0001 OR=2.66 (95% CI 1.72, 4.11) p<0.0001 40 OR=1.45 (95% CI 0.98, 2.14) p=0.064 OR= (95% CI 1.16, 2.55) p<0.0062 Response Rate (%) 20 22.1 23.0 16.4 The main secondary endpoint was continuous abstinence during weeks 9-52, again defined as not a single puff of a cigarette. Again the quit rates are very similar in the two studies and show odds ratios of 3.1 and 2.7 for Varenicline versus placebo and odds ratios of 1.5 to 1.7 for Varenicline versus Zyban. 15.0 10.3 8.4 N=349 N=329 N=344 N=343 N=340 N=340 Study I Study II Varenicline Zyban Placebo OR = odds ratio
 p< OR=2.66 (95% CI 1.72, 4.11) p< OR=1.45 (95% CI 0.98, 2.14) p= OR=1.72 (95% CI 1.16, 2.55) p< Response Rate (%) The main secondary endpoint was continuous abstinence during weeks 9-52, again defined as not a single puff of a cigarette. Again the quit rates are very similar in the two studies and show odds ratios of 3.1 and 2.7 for Varenicline versus placebo and odds ratios of 1.5 to 1.7 for Varenicline versus Zyban N=349. N=329. N=344. N=343. N=340. N=340. Study I. Study II. Varenicline. Zyban. Placebo. OR = odds ratio.")
57
Participants: A total of 412 cases receiving routine care.
Short-term smoking cessation rates in those taking single nicotine replacement therapy (NRT), combination NRT or varenicline Design: Evaluation of consecutive routine cases before and after the introduction of varenicline. Setting: National Health Service (NHS) tobacco dependence clinic in London, UK. Participants: A total of 412 cases receiving routine care. Intervention: Seven group support sessions over 6 weeks with either nicotine replacement therapy (NRT) (n = 204) or varenicline (n = 208). Abstinence measure Single NRT (n = 121) Combination NRT (n = 83) Varenicline (n = 208) Odds ratio (95% CI) Adjusted odds ratio (95% CI) Difference (95% CI) % CO verified 57.9 (70/121) 66.3 (55/83) 72.1 (150/208) 1.88 (1.18–3.02) 1.96 (1.15– 3.33) 14.2% (3.6%–25.0%) % DH self-report 66.1 (80/121) 74.7 (62/83) 80.3 (167/208) 2.09 (1.26–3.47) 2.27 (1.27– 4.05) 14.2% (4.2%–24.2%) Addiction 2008;103:
, combination NRT or varenicline. Design: Evaluation of consecutive routine cases before and after the introduction of varenicline. Setting: National Health Service (NHS) tobacco dependence clinic in London, UK. Participants: A total of 412 cases receiving routine care. Intervention: Seven group support sessions over 6 weeks with either nicotine replacement therapy (NRT) (n = 204) or varenicline (n = 208). Abstinence measure. Single NRT (n = 121) Combination NRT (n = 83) Varenicline (n = 208) Odds ratio (95% CI) Adjusted odds ratio (95% CI) Difference (95% CI) % CO verified (70/121) 66.3 (55/83) 72.1 (150/208) 1.88 (1.18–3.02) 1.96 (1.15– 3.33) 14.2% (3.6%–25.0%) % DH self-report (80/121) 74.7 (62/83) 80.3 (167/208) 2.09 (1.26–3.47) 2.27 (1.27– 4.05) 14.2% (4.2%–24.2%) Addiction 2008;103:")
58
Varenicline: A First-Line Treatment Option for Smoking Cessation
Clin Ther 2009;31:

59
Varenicline for Smoking Cessation
Comparison N Trials N Participants Pooled RR (95% CI) Varenicline vs placebo 6 2,582 2.33 (1.95 –2.80) Varenicline vs Bupropion 3 1,622 1.52 (1.22– 1.88) Varenicline vs NRT 1 757 1.31 (1.01– 1.71) . Key Point Data from multiple trials have outlined the efficacy of specific antidepressant therapy (bupropion, nortriptyline) for quitting smoking. Background Multiple trials have been conducted investigating antidepressant therapy, including bupropion, nortriptyline, and several selective serotonin-reuptake inhibitors (SSRIs), for quitting smoking. A Cochrane review of the literature found 24 trials studied the use of bupropion therapy either alone or in combination with other methods (eg, NRT). Analysis of data from 19 trials that investigated bupropion monotherapy resulted in an OR of 2.06 for success in quitting smoking. Two trials of bupropion plus NRT patch treatment compared with placebo yielded an OR of only The combined OR for all trials of bupropion versus placebo was Compared with bupropion, fewer trials have been conducted with nortriptyline (24 vs 6, respectively), and in the whole of the published literature, it has only been tested for quitting smoking in approximately 500 smokers.1,2 A Cochrane analysis of all available data revealed an OR of 2.14 for quitting smoking. This increased slightly to 2.79 when only the trials of nortriptyline monotherapy were included in the analysis.1 There is limited or no evidence of long-term benefit with other antidepressants including the monoamine oxidase inhibitor, moclobemide, the atypical, venlafaxine, or the selective serotonin reuptake inhibitors, fluoxetine, sertraline, and paroxetine.1 References 1. Hughes J, Stead L, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD 2. Hughes JR, Stead LF, Lancaster T. Nortriptyline for smoking cessation: a review. Nicotine Tob Res. 2005;7:491–499. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database of SystematicReviews 2008, Issue 3.
 Varenicline vs placebo. 6. 2, (1.95 –2.80) Varenicline vs Bupropion. 3. 1, (1.22– 1.88) Varenicline vs NRT (1.01– 1.71) . Key Point. Data from multiple trials have outlined the efficacy of specific antidepressant therapy (bupropion, nortriptyline) for quitting smoking. Background. Multiple trials have been conducted investigating antidepressant therapy, including bupropion, nortriptyline, and several selective serotonin-reuptake inhibitors (SSRIs), for quitting smoking. A Cochrane review of the literature found 24 trials studied the use of bupropion therapy either alone or in combination with other methods (eg, NRT). Analysis of data from 19 trials that investigated bupropion monotherapy resulted in an OR of 2.06 for success in quitting smoking. Two trials of bupropion plus NRT patch treatment compared with placebo yielded an OR of only The combined OR for all trials of bupropion versus placebo was Compared with bupropion, fewer trials have been conducted with nortriptyline (24 vs 6, respectively), and in the whole of the published literature, it has only been tested for quitting smoking in approximately 500 smokers.1,2 A Cochrane analysis of all available data revealed an OR of 2.14 for quitting smoking. This increased slightly to 2.79 when only the trials of nortriptyline monotherapy were included in the analysis.1. There is limited or no evidence of long-term benefit with other antidepressants including the monoamine oxidase inhibitor, moclobemide, the atypical, venlafaxine, or the selective serotonin reuptake inhibitors, fluoxetine, sertraline, and paroxetine.1. References. 1. Hughes J, Stead L, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD Hughes JR, Stead LF, Lancaster T. Nortriptyline for smoking cessation: a review. Nicotine Tob Res. 2005;7:491–499. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database of SystematicReviews 2008, Issue 3.")
60
Drug costs for nicotine replacement therapy (NRT) and varenicline users (£).
Single NRT (n = 121) Combination NRT (n = 83) All NRT (n = 204) Varenicline (n = 208) Cost per patient treated 99.2 169.6 127.8 136.8 Cost per quitter* 171.5 255.9 208.6 189.7 Cost per quitter† 150 227 183.6 170.4 *% Carbon monoxide (CO) verified abstinence. †% Department of Health (DH) self-report abstinence. Addiction 2008;103:
 Combination NRT (n = 83) All NRT (n = 204) Varenicline (n = 208) Cost per patient treated Cost per quitter* Cost per quitter† *% Carbon monoxide (CO) verified abstinence. †% Department of Health (DH) self-report abstinence. Addiction 2008;103:")
61
Varenicline: adverse events
Varenicline (n=349) 30 Bupropion SR (n=329) Placebo (n=344) 25 Incidence (%) 20 15 10 5 Nausea Headache Insomnia Abnormal dreams Gonzales D, et al. JAMA 2006;296:47–55 61
 30. Bupropion SR (n=329) Placebo (n=344) 25. Incidence (%) Nausea. Headache. Insomnia. Abnormal dreams. Gonzales D, et al. JAMA 2006;296:47–")
64
Rimonabant (Acomplia®)
For treating obesity and tobacco addition Approved in UK Cannabinoid recepror modulators First potent selective CB1 20mg/day x 1 year Champix 的作用機轉 Champix 的戒菸療效來自於對42受器的部份致效作用 阻斷尼古丁與受器結合, 故 Champix 可以: 減少對吸菸的渴求及戒斷症狀 (致效作用) 降低抽菸的滿足感及感官強化效果 (拮抗作用) 使用Champix較常見的副作用為噁心、頭痛、失眠以及異夢 Key point The efficacy of varenicline in smoking cessation results from its partial agonist activity at the 42 nicotinic receptor. By physically blocking the binding of nicotine, varenicline’s partial agonist activity produces an effect sufficient to alleviate symptoms of craving and withdrawal (agonist activity) while simultaneously resulting in rewarding and reinforcing of the effects of smoking (antagonist activity). Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK
 降低抽菸的滿足感及感官強化效果 (拮抗作用) 使用Champix較常見的副作用為噁心、頭痛、失眠以及異夢. Key point. The efficacy of varenicline in smoking cessation results from its partial agonist activity at the 42 nicotinic receptor. By physically blocking the binding of nicotine, varenicline’s partial agonist activity produces an effect sufficient to alleviate symptoms of craving and withdrawal (agonist activity) while simultaneously resulting in rewarding and reinforcing of the effects of smoking (antagonist activity). Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK")
65
電子菸為非法產品~~

68
祝福 吸菸者戰菸成功

Similar presentations




家 族與腫瘤細胞的增生、血管生成及進展有密切的相關,其中又以 MMP-2.>")
 資料來源 : 邱淑媞局長 98 年底戒菸工作討論會講義資料.>")

 ä 雄激素拮抗剂( Anti-androgen ) ä 全雄阻断( TAB.>")















> 200 mg/dL或三酸甘油酯(TG)> 150 mg/dL或高密度脂蛋白(HDL-C)< 40 mg/dL或低密度脂蛋白(LDL-C)>>")